What is caries and its 4 stages
Human teeth have a multilayer structure. The inner layer is the pulp, consisting of blood capillaries and nerve endings, followed by dentin, which forms the pulp cavity. The root part of the teeth is covered with cement, the crown part is covered with enamel about 2 mm thick. It protects the inner layers from traumatic external influences. Scientists have found that this is the hardest tissue in the human body. It consists of 97% inorganic substances. But even such a durable fabric can begin to collapse for various reasons (they will be discussed a little later). This process is called caries.
Caries is a dental disease that causes pathological destruction of hard tooth tissues.
The process starts with the enamel. Without treatment, the disease progresses and destroys dentin and reaches the pulp. Its development can be triggered by a number of external and internal factors. Without treatment, it can result in tooth loss and infection of periodontal tissue. According to statistics, this is the most common disease on the planet; more than 93% of the world's population suffered from it. Timely initiation of treatment therapy guarantees a positive result. In its development, caries goes through 4 stages without treatment:
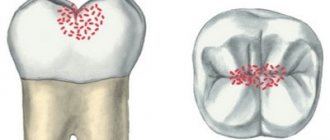
- spot stage – demineralization of a local area of the surface, visually noticeable as a white matte spot. There are no other symptoms;
- superficial phase – destruction of the enamel layer. A reaction to external stimuli appears (hot, cold, sweet, sour);
- medium – the pathological process begins to destroy dentin. Pain is added to the early symptoms;
- deep – the affected area increases, pain becomes constant.
Causes and features of deep caries
The main reason for the development of caries is bacterial plaque that accumulates on tooth enamel, most often in hard-to-reach places. Microorganisms living in these deposits produce acid during their life, which gradually softens and destroys the enamel. The process is accelerated by low resistance of dental tissue to external influences, poor diet, and hereditary predisposition.
Deep dental caries never begins immediately; the process progresses gradually.
First, a whitish or yellowish spot appears on the affected area. Then it darkens, the surface loses its smoothness and shine, becomes rough, and tissue destruction begins. When destructive changes reach the last stage, the deepest layers of dentin are affected. If the thickness of the remaining tissues that separate the carious cavity from the nerve is too small, the tooth reacts to the influence of any irritants with pain.
The last stage of caries without treatment can be complicated by diseases such as pulpitis and periodontitis. When they develop, inaction is fraught with tooth loss, which can only be restored through implantation.
Indications for treatment
You should make an appointment with a doctor if a white spot on the enamel surface becomes noticeable or its color has darkened. This should also be done if a piece of a tooth breaks off or a crack appears on it, or the border of a previously placed filling has darkened. A clear indication is the formation of a carious cavity, the appearance of a reaction to irritants, and pain. You will have to postpone going to the dentist if you have an infectious disease or herpes in the acute phase. Treatment during pregnancy must be agreed upon with the attending obstetrician-gynecologist.
Important: the sooner the patient contacts the dentist, the easier it will be to stop the pathological process. Therefore, a preventive visit to the doctor is no less important than a visit to the doctor when symptoms appear.
Deep chronic caries
The chronic form is characterized by a slower course: demineralization of the tooth occurs gradually, which inhibits destruction. In addition, the processes occurring during fissure caries cause blockage of the dentinal tubules, which makes the dentin less permeable to infection. As a result, pulp irritation also decreases, as a result of which pain in chronic caries is less pronounced and acute. Inflammation may not affect the nerve for a long time, since the inside of the pulp chamber is covered with replacement secondary dentin. Sensitivity to temperature influences is also less pronounced.
Despite this, chronic deep caries can be no less, or even more dangerous, than acute caries. Since the process often occurs with minor or no symptoms, by the time you contact a doctor, it sometimes manages to destroy a significant part of the tooth. Under unfavorable circumstances, inflammation can also affect the tissue surrounding the tooth. The long course of chronic caries often leads to the appearance of a specific unpleasant odor from the mouth.
Methods used to treat the disease at different stages
Varying degrees of damage to dental tissue dictate the need for an individual approach in each specific case. So, at the white spot stage, it is necessary either to mineralize the enamel to restore it, or to remove the stain using a minimally invasive infiltration method without affecting healthy tissue. If necrotic substances are present, they must be carefully removed, the cleaned surface must be treated with an antiseptic and a seal must be placed. If the pathology has led to significant destruction of the dental unit, then in addition to the described actions it will be necessary to restore the shape of the tooth. This is done using the method of restoration or dentures.
Diagnosis and treatment
To diagnose deep caries, the dentist uses the following methods:
- Patient interview. The specialist is interested in complaints and the duration of the manifestation of pathological symptoms.
- Examination of the oral cavity and diseased tooth. The doctor visually examines the affected area, identifying significant tissue destruction or the presence of a small external defect.
- Probing. A dental probe helps determine whether the floor of the cavity is sensitive or painless.
- Thermometry. Using this method, the tooth's reaction to temperature stimuli is checked.
To clarify the diagnosis, EDI (electroodontodiagnosis) and radiography may be needed.
High-quality treatment of deep caries consists of eliminating the infection, removing destroyed tissue and filling the cleaned cavity. All manipulations are carried out under reliable anesthesia. One appointment may not be enough to complete the therapeutic process. A second visit is required if the doctor doubts that the pulp is not infected. In this case, after treating and cleaning the cavity, the dentist installs a temporary restorative filling. If the tooth does not bother the patient for several days and does not react to temperature stimuli, then during the second visit the doctor places a permanent filling. Then he grinds and polishes the surface, giving it an anatomical shape.
Protocol for classical treatment of deep caries
- Diagnosis of the degree of tissue damage (including using x-rays)
- Performing local anesthesia
- Drilling out the affected dentin, giving the cavity a geometric shape (if pulp damage is detected, depulpation will be performed)
- Antiseptic treatment
- Adding calcium preparation
- Installing a temporary filling
- After 2–3 days, remove the temporary filling; if the condition of the cavity is satisfactory, fix the permanent filling
- Sanding and polishing
Note: specialists from the “Smile” clinic network have extensive practical experience in caries treatment. The use of modern equipment allows us to provide assistance to patients in clinical situations of any severity.
Treatment of complicated caries
The principle of atraumatic restorative treatment of caries (ART-method) consists of manual removal of lesions without the use of rotary instruments and without anesthesia at the stage of cavity preparation. The conservatively prepared cavity is subsequently restored using glass ionomer cement (GIC), which chemically binds to tooth tissue and also provides ion exchange, affecting the remineralization of dentin affected by caries.
The ART technique is a minimally invasive procedure that minimally disturbs the patient and allows for rapid restoration of areas affected by caries. 80% of ART restorations that occupy one surface of a permanent tooth last on average up to 5 years, and in the case of ART restorations on several surfaces, only 60% of them can function for up to 2 years. Given this, it is understandable why the American Academy of Pediatric Dentistry has endorsed the use of the ART approach for performing interim therapeutic restorations (ITRs). Temporary restorations are performed if, due to lack of materials or the patient's refusal to cooperate, it is not possible to install a final filling. Treatment of early childhood caries with temporary restorations has become a common practice, providing effective results according to modern dental approaches to the treatment of primary teeth (CDT code 2941). The use of such an algorithm in the treatment of caries in permanent teeth (CDT code 2940) is less effective due to limitations in terms of durability and esthetics of glass ionomer cement restorations.
The negative role of caries in early childhood, the psychological and communicative advantages of using ITR restorations in the treatment of severe forms of caries are well known and have been highlighted in a number of publications. However, no reports have been found on the use of this approach in adolescents or adults, although the psychological and communication problems of patients associated with visible caries lesions remain the same. Glass ionomer cements used in ART techniques do not have sufficient aesthetic characteristics and physical properties necessary for performing extensive restorations in permanent teeth. The clinical example described in this article demonstrates the ability to perform temporary restorations with a modified ART technique using a new, bioactive, dual-curing glass ionomer cement with tailored esthetic and physical properties consistent with the quality of today's advanced composite materials.
Modified technique
When using resin-modified glass ionomers (RMGIs) instead of traditional GICs, it is necessary to take into account the need to make changes to the traditional ART technique. For example, it is necessary to carry out light polymerization, use rotary instruments to correct occlusion and shape the contour of the restoration, as well as for subsequent grinding and polishing of the filling. None of the above steps are typical for the traditional ART technique. Modified glass ionomer cements have improved esthetic and physical properties compared to conventional GIC, but their use is not possible without high-speed handpieces or without providing access to light for polymerization.
However, taking into account modern dental approaches, the advantages of modified glass ionomer cements justify the use of a modified ART technique. These benefits include stopping the progression of caries and ensuring pulp vitality while improving the patient's internal comfort and social adaptation. Promptly performed temporary restorations help stop the destruction of healthy enamel and dentin, protect the dental pulp, provide opportunities for routine oral hygiene, and at the same time take part in tissue remineralization.
Clinical case
A 28-year-old woman, due to feelings of internal anxiety, turned to the author of the article for help. She claimed that her teeth had recently become more "sensitive" and at the same time had changed in appearance for the worse, so she asked for dentures to be made as she claimed that she hated the way her teeth looked and was just wasting her money to correct this situation.
After analyzing the patient’s medical history, and without diagnosing any systemic or bad habits, we came to the conclusion that the cause of the present cervical caries may be excessive consumption of sweet iced tea, and rare visits to the doctor for professional hygiene. Plaque scores were acceptable except for areas around demineralized and carious lesions that were “too sensitive to brush.” The patient listened to the recommendation of a friend who suggested replacing sugar with xylitol when making tea, but prolonged sensitivity to temperature stimuli and discomfort during brushing and eating, as well as an unacceptable aesthetic appearance, forced the patient to seek dental care.
Treatment protocol
The patient is a key figure in the dental treatment process, so his scrupulousness and feelings about the chosen treatment methods should be taken into account. Patients with limited financial resources may be satisfied with the fastest possible restoration without fully considering the possible long-term consequences. Tooth extraction followed by complete dentures is one such quick treatment method. After a brief discussion regarding the time and cost of temporary restorations, the patient agreed to similar treatment of the maxillary anterior teeth during the consultation visit. She also approved the use of 20% benzocaine solution as a local anesthetic followed by the use of 1 ml of 4% articaine 1:100,000 solution for infiltration anesthesia in the root area of 6-11 teeth. ACTIVA BioActive-Base/Liner and ACTIVA BioActive-Restorative (Pulpdent) were selected for operative restoration of lesions as low-cost options for reducing sensitivity and achieving acceptable esthetic results. The outcome of this simple treatment approach, taking into account the wishes of the patient, his attitude towards his own dental health and feelings of discomfort due to aesthetic problems, will be discussed below in parallel with the stages of treatment.
Photographs taken before treatment show the carious lesions present (Photo 1 and Photo 2). Removal of the diseased tissue using a hand excavator helped clean the surface of the tooth, followed by grinding of the edges of the cavities using a high-speed handpiece (Figure 3). Treatment of several teeth by manual preparation helped convince the patient that the use of dental instruments was painless, so she tolerated the preparation and cavity preparation stages well, despite the fact that this was her first visit to the dentist.
Photo 1. The patient came in because of complicated cervical caries.
Photo 2. The patient came in because of complicated cervical caries.
Photo 3: Finishing the edges and surface of the cavity using rotary instruments.
A clean and prepared cavity margin plays an important role in ensuring the longevity of temporary restorations. Complete removal of the affected dentin near the pulp chamber is not necessary, since in the process of mineral exchange between the tooth tissues and the glass ionomer material, the hardness of the affected tissues will be restored to their natural state. Maintaining pulp vitality is one of the advantages of temporary restorations. In the author's experience, cases of iatrogenic pulpitis after glass ionomer cement restorations have occurred extremely rarely, but the risk of their occurrence must be taken into account, especially in cases where the thickness of the residual dentin is less than 0.5 mm.
ACTIVA Base/Liner has a lower acidity level than ACTIVA Restorative. It is also less filled and therefore has more free monomers on the surface. As a consequence, it can be argued that the liner is more active than the restorative material and adheres to the dentin without prior etching or bonding. When the dentin thickness above the pulp chamber was less than 0.5 mm, a thin layer of ACTIVA Base/Liner was placed using a static mixer tip and cured for 20 seconds with Flashlite Magna 4.0 (DenMat) (Figure 4).
Photo 4. When the dentin thickness above the pulp chamber was less than 0.5 mm, a thin layer of ACTIVA Base/Liner was applied and cured for 20 seconds.
After this, the edges of the enamel were etched with 38% phosphoric acid for 15 seconds, after which they were washed off and slightly dried, avoiding overdrying the surface. If it was necessary to create contact points, a Mylar matrix was used, and ACTIVA BioActive-Restorative restorative material was placed in one portion, after which it was contoured and illuminated (photo 5). Each restoration was cured for 20 seconds, after which the material was left undisturbed for 3 minutes to complete the dual-curing process. Both the liner and the base material adapted to the cavity walls without forming pores. Sanding was performed using a handpiece and hex finishers followed by Enhance Polishing Cups (DENTSPLY Caulk). The temporary restorations performed at the patient's first visit are shown in Figure 6.
Photo 5. Volumetric installation of ACTIVA BioActive-Restorative material followed by contouring and polymerization.
Photo 6. Results after treatment.
After a 24-hour follow-up visit, there were no signs of hypersensitivity; the patient even thanked the doctor for convincing her to save her own teeth. Three days later, the patient inquired about the possibility of teeth whitening at home, stating that she had no sensitivity to chemical, thermal or brushing irritants, and stated that she was looking forward to her next dental visit.
Discussion
Every new problem in restorative dentistry should open the door to new opportunities, which sometimes bring pleasant surprises. Treatment of caries requires restorative intervention, as well as correction of diet, lifestyle and oral hygiene skills at home. Maintaining pulp vitality should be the main priority in treatment, but remineralization of the affected areas of enamel and dentin is important for the preservation of the tooth itself. Historically, the best technique for treating early caries has been the ART technique, which uses either conventional or modified glass ionomer cements. Although in terms of durability, restorations made using the ART technique can still compete with the use of traditional materials that require more invasive preparation methods, but in terms of aesthetics, physical properties and wear of filling surfaces, glass ionomer restorations clearly lose.
ACTIVA BioActive liner and restorative material consists of a curable, biocompatible urethane derivative and glass ionomer ions that are involved in the remineralization of enamel and dentin. These materials also have increased density, making them suitable for restoring all tooth surfaces and all classes of cavities. The remarkable aesthetics, durability, surface appearance of the restoration, as well as the simplified mixing and application technique of ACTIVA materials, made them ideal for use in both minimally invasive restoration techniques and traditional restorative approaches.
To control caries lesions, ion exchange and remineralization potentials must exceed those of traditional materials. From a clinical point of view, excellent functional and aesthetic results have been achieved with ACTIVA materials, and the possibility of iatrogenic pulpitis and pulp necrosis has been minimized. Another surprise during treatment was the change in the patient's attitude towards his natural teeth. Although the restoration method was different from the conventional ART technique, and there was still a small difference between the price of ACTIVA materials and other conventional and modified glass ionomer cements, all this was compensated by the saved patient time and his satisfaction with the treatment results.
Conclusion
Traditional and modified glass ionomer materials are an important link in the treatment of caries using atraumatic minimally invasive techniques or when performing temporary restorations. As the author continues to study the biologically active properties of restorations made using ACTIVA materials, he becomes increasingly interested in expanding the use of intermediate or temporary restorations as long-term therapeutic restorations with comparable levels of esthetics and durability comparable to modern complex composite restorative systems. can also be achieved with modified glass ionomer cements. The use of a reliable, durable, aesthetic and bioactive composite material may provide a new approach to tooth preservation and treatment of early dental caries in adults.
Author: Nels Ewoldsen, DDS, MSD
How to care for treated teeth
Dentists advise not to eat for a couple of hours after installing a permanent filling (residual effects of anesthesia can cause injury to the oral mucosa). During the day, do not apply increased pressure to the sealed area, i.e. do not chew nuts and other particularly hard foods. It is possible that the filling will cause slight discomfort. If it does not go away within a week, you should contact your dentist to correct the shape of the filling. Dental care after visiting the clinic is the same as usual: brushing your teeth twice a day, rinsing your mouth after eating and drinking sugary drinks.
The dental network offers services for the diagnosis and effective treatment of dental caries at any stage of its development. Contacting our branches has significant advantages:
- treatment by highly qualified doctors;
- compliance with treatment protocols that meet international standards;
- family and savings discounts;
- stable cost of services;
- Convenient daily work schedule.
You can contact any of the branches of our clinic in Moscow, located within walking distance from metro stations:
- Art. Alekseevskaya (VDNKh district, etc. Mira), address: st. 3rd Mytishchiskaya house 3, building 2;
- Art. Shelepikha, address: Shelepikhinskaya embankment, address: building 34, building 1.
Modern technologies and techniques used in our clinic make each stage of treatment effective. The high qualifications of our specialists serve as a guarantee of quality and safety. The health of your teeth is in good hands!
Treatments to relieve suffering
In advanced cases, specific individual techniques are used.
- Anesthesia. It is necessary. The dentin located near the pulp is especially sensitive, so when working with the tooth, pain may occur.
- The affected tissue is removed accompanied by cooled air and water. This is necessary to reduce the likelihood of overheating the tooth surface.
- Anti-inflammatory pads and pastes are used. This is necessary to strengthen the internal tooth tissues located above the pulp, remove bacteria, preventing the development of complications.