Review of plastic dental crowns – stages of their manufacture, indications for installation and current prices
Article navigation
- Short description
- What types of plastic crowns are there?
- Materials
- Manufacturing methods
- Indications and contraindications
- Pros of crowns
- Flaws
- Stages of dental restoration
- Installation Features
- How long can you wear it?
- Life time
- Price
Question for a specialist
Today dentistry has a variety of materials for prosthetics. Among others, plastic stands out, which has fairly good aesthetic characteristics and low cost. Should I wear plastic crowns permanently? Of course not. But some types can be used for quite a long time. Next, we will talk about the features of dental crowns made of plastic, the pros and cons of these orthopedic structures, their service life and prices.
Advantages and disadvantages
Plastic teeth have been used since the 30s. They are most often used on the frontal group (incisors and canines) and try not to place them as chewing teeth, where a large load falls.
- Pros: easy to manufacture; low cost and, as a result, price; good aesthetic properties (worse than porcelain crowns, but still)
- Cons: wear out quite quickly; due to porosity, they lose color over time (this is called hygroscopicity) and accumulate pathogenic microflora on their surface; may irritate the gums; cause allergies in some cases
Brief description of products
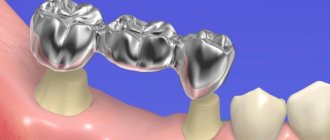
Plastic crowns are artificial dental crowns in the form of single caps made from dental plastics. They are used to protect a tooth when it is severely damaged, as well as to restore the aesthetics of a smile. The “cap” is attached to the abutment tooth, core inlay or implant (more precisely, to the abutment on the implant). Externally, it imitates a natural tooth quite well, because plastic can be easily painted to the desired shade. What the prosthesis looks like is shown in the photo below. Plastic crowns are classified as non-removable. To restore several teeth in a row, plastic crowns are combined into a bridge.
CHAPTER 16. MANUFACTURE OF METAL-PLASTIC AND METAL-COMPOSITE DENTURES
, solid dentures are now widely used
especially with aesthetic cladding.
Such prostheses, in addition to metal-ceramic,
include
metal-plastic
(metal-acrylic) and
metal-composite.
These structures have good mechanical properties, are very aesthetic and closely imitate natural teeth. Plastic has been used as a facing material for metal dentures, especially for front teeth, for quite a long time. However, its inherent disadvantages, such as the possibility of developing toxic-allergic reactions, high abrasion, low color stability, prompted the development of a new class of materials - composites. Currently, in orthopedic dentistry, a wide arsenal of veneering materials is used in the manufacture of metal-composite dentures.
16.1. SEQUENCE OF CLINICAL AND LABORATORY STAGES IN THE MANUFACTURE OF METAL-PLASTIC AND METAL-COMPOSITE DENTURES
Metal-plastic and metal-composite dentures are currently quite widely used in orthopedic dentistry clinics. These dentures are classified as non-removable; they consist of a metal frame and a facing layer made of plastic or composite materials. The manufacturing technology of such dentures includes the manufacture of a cast metal frame, covering it with a plastic or composite lining and contains the following steps.
— Stage 1 - clinical:
◊ examination of the patient, diagnosis, choice of treatment plan and design of the medical device - metal-plastic or metal-composite dental prosthesis;
◊ preparation of abutment teeth under anesthesia;
◊ at the same stage it is possible to obtain impressions and register central occlusion or central ratio; the prepared abutment teeth must be covered with temporary plastic crowns, especially for vital teeth.
— Stage 2 - laboratory:
◊ making dismountable plaster models of jaws and plastering them into an articulator or occluder;
◊ wax modeling of the prosthesis frame and preparing it for casting.
— Stage 3 - laboratory:
◊ obtaining a metal frame of a denture by casting (usually carried out in a foundry laboratory by a dental foundry technician).
— Stage 4 - laboratory:
◊ fitting a metal frame of a denture to a collapsible plaster model of the jaw.
— Stage 5 - clinical:
◊ fitting the metal frame of the denture to the supporting teeth in the oral cavity;
◊ determination of the color of plastic or composite cladding.
— Stage 6 - laboratory:
◊ production of lining (plastic or composite) on the metal frame of the denture;
◊ polishing a manufactured metal-plastic or metal-composite denture.
— Stage 7 - clinical:
◊ application and fixation of a metal-plastic or metal-composite denture in the oral cavity.
Materials for production
Plastic dental crowns are usually made from materials obtained by mixing two components - liquid and powder. As a result, a plastic mass is formed from which the prosthesis is already made. But some manufacturers produce ready-made paste in small dispensers. There are acrylic monomer and non-monomer materials - for example, Tempron from GC (Japan). As well as plastic composite non-monomer compositions - for example, DentaCrown from Itena (France), Protemp 4 from 3M ESPE (USA). There are also initially solid PMMA (thermoplastic plastic) blocks. Telio CAD from Ivoclar Vivadent is also such a material.
There are plastic crowns in which the plastic is specially reinforced at the production stage - for greater strength and wear resistance of the structure. For example, this could be reinforcement - strengthening a plastic cap with a metal or fiberglass mesh. There are also metal-plastic products - they are based on a metal cap, which is covered on top or only on the side with a layer of light synthetic material1.
Methods for making dentures
The production of plastic dental crowns can be carried out in two ways:
- direct: in the dentist's office, i.e. in the presence of the patient. Very fast method of prosthetics,
- indirect: in a dental laboratory based on previously taken impressions of the patient’s dentition. It takes longer, but as a result the product “sits” more accurately on the support and adheres to it without gaps.
Plastic crowns can be made using cold or hot polymerization (hardening of plastic compounds). There are also stamped and milled plastic "caps". The latter are distinguished by the highest production accuracy, because are cut on computerized machines, which eliminates any errors.
Another option is standard, that is, templated plastic crowns. These are used in removable or adaptive dentures on implants. Essentially, these are just ready-made teeth that are inserted into an acrylic base.
Long-term temporary plastic crowns
The use of temporary crowns in orthopedic dentistry is advisable and fully justified. Neglect of this rule may lead to negative consequences, which include:
- pain in the area of the prepared tooth as a consequence of the development of pulpitis, temperature and chemically caused;
- lack of aesthetics, which is especially important when treating frontal teeth;
- inability to fully chew food;
- speech problems (pronouncing some sounds may be difficult);
- violation of occlusion;
- dysfunction of the temporomandibular joint, etc.
The best option for replacing defects are temporary long-term plastic crowns. Unlike conventional temporary crowns, which are often made directly (in the patient’s mouth) and installed for a short period of time (usually a few days), this type of restoration is created in a dental laboratory from hot polymerization plastic, which allows them to be used for a longer period of time, taking into account all features of orthopedic treatment.
Manufacturing stages
There are several laboratory stages in the manufacture of such crowns:
- creation of two plaster models (one working, the other auxiliary) based on the impressions obtained, which are then checked for compliance with the central occlusion and plastered into a special articulator;
- design of the gingival margin on the working model (the technician cuts it off until its deepest imprint in the sulcus is reached);
- giving the model an anatomical shape (wax is used for this purpose), the created reproduction, as a rule, has a larger volume, taking into account that the plastic will subsequently undergo additional processing after hardening;
- creating a plaster block from a tooth model;
- vertical, angled or other plastering of the cuvette, which is subsequently separated after the wax is cast;
- placing the plastic in a pre-cooled cuvette;
- polymerization of plastic followed by finishing (grinding, polishing).
After this, the temporary crown is sent to the clinic for fitting - the doctor checks it for compliance with the occlusal relationships, evaluates the shape and color. Then it is again given to the dental technician, who makes adjustments (if necessary) and carries out the final processing of the product.
The final stage is the fixation of a temporary long-term plastic crown with cement, the shade of which is selected for each plastic separately.
Indications and contraindications
Plastic crowns are suitable for installation on both chewing and front teeth. And also for implants. But, we repeat, this will be temporary prosthetics. However, you cannot do without it in the following cases:
- it is necessary to preserve or restore the aesthetics of the smile while a permanent prosthesis is being made: this becomes especially important when the upper front teeth are prosthetic - after all, the entire smile depends on their appearance,
- it is necessary to protect the ground teeth from infection from outside or from injury,
- you need to maintain the level of the gum before installing a permanent prosthesis: the point here is that the layer of enamel on the stump can be worn down quite strongly, plus the stump is ground down with a slight ledge near the gum. And if the permanent crown takes a long time to be made - more than 2-3 weeks, then the gum tissue will simply grow onto the ledge (bottom of the stump). Therefore, permanent installation will be painful, there will be bleeding, inflammation of the gums, pain and discomfort in wearing.
There are practically no contraindications to installation. But one can highlight the risk of allergies, especially if conventional plastics are used rather than composite monomer-free compounds. It is the monomer that most often causes allergies. At risk are children, people of retirement age and those who are already allergic to anything. Another contraindication is the inability to wear prosthetics at a given time. For example, if you have recently suffered a serious illness or in the coming weeks it will not be possible to maintain good oral hygiene.
Advantages of plastic crowns
The advantages of plastic crowns lie in the characteristics of the material. After all, it is inexpensive, easy to process and has the color of natural enamel. The positive aspects look like this:
- you can quickly restore a damaged tooth: literally in 1 hour, maximum in 1 day,
- good aesthetics: plastic does not stand out from the dentition,
- low cost,
- allows you to protect the ground tooth, adjacent gums or tissue around the implant: while a permanent prosthesis is being made or while the implant is taking root,
- prevents neighboring teeth from moving towards the defect (“holes” in the row).
As for the ground teeth, if you leave everything as it is (and do not put a temporary plastic crown on the stump), then the remaining layer of dentin without enamel will be attacked by microbes, destroyed by acids or trauma. Since in general dentin is much weaker than enamel. This is reflected in pain throughout the tooth. The shape of the stump may be disrupted - i.e. the prosthesis being manufactured simply will not fit.
Preparation
Preparation for a plastic crown should always be carried out with an eye to the fact that the material used as a prosthesis is not the strongest, which leads to greater wall thickness. With antagonist teeth, the structure should be separated by at least 1, preferably 1.5 mm. The fabrics must be removed evenly from all sides and almost vertical walls must be created.
- To create a ledge in the area of the tooth neck, the proximal surfaces are first separated
- They begin to prepare the vestibular and oral surfaces (with cone-shaped or cylindrical burs), also forming a ledge. As a result, it should be up to 1 mm wide (0.5-0.8 is possible). The best shoulder shape is straight and circular with a smooth surface and a wall perpendicular to the tooth axis
- A gap of the indicated 1-1.5 mm is made between the tooth being ground and the antagonists, and the crown is prepared to a cone depending on the tooth in one direction (chewing surface or cutting edge)
- Using an end bur, the ledge is deepened 0.1 mm into the gingival margin. It is important not to make the depression larger due to the fact that plastic has the negative property of swelling and putting pressure on the mucous membrane (swelling or even tissue death). To prevent injury, gum retraction can be performed. This completes the tooth preparation with a plastic crown.
What shortcomings can be found
There are few disadvantages (in number) of plastic crowns on teeth, but they are quite significant. See for yourself:
- fragility of the material,
- a high probability of gum inflammation during long-term use due to a not very tight fit to the gum and support (this does not apply to milled dentures made using CAD/CAM technologies),
- there is a high probability of caries appearing under the prosthesis if the period of wearing it is exceeded,
- risk of allergies,
- rapid loss of color, darkening, pigmentation from food and other dyes: due to the presence of micropores on the surface.
Afterwards, the plastic prosthesis is replaced with a more durable, aesthetic, durable one - for example, ceramic, metal-ceramic, zirconium dioxide, ceramic composite. That is, a permanent one that will last for many years.
South Korean implant Osstem - 20,000 rub.
Hurry up to sign up for a free consultation and lock in promotional prices.
Call now or request a call
Opening hours: 24 hours a day - seven days a week
Plastic crowns. - presentation
Lavrukhina Anastasia 3rd year, 5th group
* An artificial crown is a dental prosthesis that covers the clinical crown of a tooth and restores its anatomical shape, size and function. According to the method of fixation, artificial crowns are classified as non-removable types of dentures.
By function: Restoring Fixing (temporary and permanent) By manufacturing method: Stamped (steel, gold) Cast (gold or special alloys) Cast with lining (metal-ceramics, metal-plastic) Manufactured by polymerization (composite, plastic) Manufactured by milling (Cerec system )
1) Accurately match the shape of the tooth being restored 2) Have a well-defined equator 3) Tightly cover the neck of the tooth throughout, plunging into the gingival groove by 0.3 mm 4) Restore contact points with neighboring teeth 5) Meet aesthetic requirements
Significant destruction of the coronal part of the tooth (IROPZ = 0.6-0.8) Incorrect position of the tooth Abnormal tooth shape Change in tooth color Pathological abrasion of hard tooth tissues
The general indication for their use is aesthetic requirements: to restore the anatomical shape of defects of carious or non-carious origin, anomalies in the shape, size or position of the anterior group of teeth (in rare cases, premolars); to replace small defects in the dentition in the anterior section with plastic bridges, then the crowns are used as supporting ones. In this case, certain clinical conditions must exist. In particular, with a low wide clinical crown, pathological abrasion of teeth, allergies, deep bite and absence of lateral teeth.
* For the manufacture of plastic crowns, hot-curing acrylic plastics are used, which have significant disadvantages: low strength, low wear resistance, color instability, high coefficient of thermal expansion, irreversible and relatively rapid aging processes of the material.
According to the classical algorithm, preparation begins with separation, removing a uniform layer of hard tissue from the contact surfaces to a thickness of 0.5-0.8 mm and giving the surfaces a slight inclination relative to the vertical axis of the tooth. Then the vestibular and oral surfaces are prepared, which should also slightly cone.
When preparing the anterior group of teeth in the upper jaw, it is necessary to maintain the shape of the palatal tubercles, which determines good fixation of the crown. Hard tooth tissues in places of occlusal contacts are removed to a thickness of at least 2 mm. The preparation of all tooth surfaces should be carried out taking into account the topography of the tooth cavity and safety zones.
It is preferable to prepare teeth for permanent plastic crowns by forming a ledge in the cervical area. As a rule, a circular ledge is formed at an angle of 90° to the vertical axis of the tooth with a width of 0.5 to 1.0 mm, which ensures: exclusion of contact of the edge of the crown with the gum (prevention of inflammation of the marginal periodontium); high-quality fixation of the crown by creating a stump of a more complex geometric shape; placement of the artificial crown within the previous contours of the tooth; a more aesthetic result of prosthetics due to the thickened edge of the crown located on the ledge.
If the preparation was carried out with the formation of a ledge, before taking an impression it is advisable to retract the gums using a retraction thread, which makes it possible to obtain a clearer tooth-gingival boundary. To make a plastic crown, anatomical impressions are taken from both jaws. The working impression is usually obtained using alginate materials. When making an impression with silicone materials, a one-stage or two-stage technique is used to obtain two-layer (two-phase) impressions.
The color of the artificial crown is determined directly by the color of the tooth to be restored, before its preparation, or by the color of the tooth of the same name, if the tooth being restored has been changed in color or has already been prepared. When choosing a color, you can focus on the color of the teeth next to the tooth being restored.
The color determination is carried out in natural light and excluding direct sunlight on the tooth using a special color scale for the material from which the crown will be made. Sharp color contrasts (bright makeup, lipstick, patient’s clothing), and bright light from a dental lamp should be avoided.
Obtaining and preparing a plaster model. Based on the resulting working impression, a model is made from ordinary medical plaster or super plaster. When assessing the quality of the resulting plaster model, special attention is paid to the accuracy and integrity of the representation of the periodontal sulcus, the stump of the prepared tooth and the teeth located next to it. A layer of compensation varnish can be applied to the stump of the prepared tooth, which creates space for the fixing material and facilitates the application of the finished crown in the oral cavity. Compensatory varnish is applied to the entire gypsum stump, not reaching 0.5 mm to the clinical neck of the tooth.
There are two known methods of indirect (on a plaster model of the jaw) production of a plastic crown: creating a wax model of the crown, followed by replacing the wax with plastic and its polymerization; layer-by-layer modeling of the crown with polymer material directly on the model with subsequent polymerization
This clinical stage includes assessing the quality of the crown, checking and, if necessary, fitting the crown on the prepared tooth in the oral cavity so that it meets all clinical requirements. The inner surface of the crown must exactly correspond to the relief of the stump of the prepared tooth. If during the modeling and crown manufacturing stages the surface of the plaster stump of the tooth was damaged, the inner surface of the crown will be distorted. To eliminate this discrepancy, irregularities that do not correspond to the relief of the imprint of the tooth stump are removed from the inner surface of the crown using a spherical bur. The edge of the plastic crown must have a contour corresponding to the relief of the gingival edge of the tooth.
During fitting, the quality of the manufactured crown is assessed according to all basic requirements: tight fit to the tooth stump, especially in the area of the clinical neck; the anatomical shape characteristic of the tooth for which the crown is made; restoration of interdental contact points; the crown should not violate the occlusion with antagonist teeth when in contact with antagonist teeth.
Temporary provisional (protective) plastic crowns are made on prepared teeth in order to: preserve the function and aesthetics of the prepared teeth visible when smiling and speaking for the period of prosthetics; protection of prepared teeth with living pulp from infection, thermal and chemical irritants; preventing displacement of supporting teeth that have lost contact with antagonists and neighboring teeth, preventing their functional overload; fixing the initial state of central occlusion; prevention of distal shift of the lower jaw; maintaining the natural contour of the gingival margin. In some cases, temporary crowns are used to expand the periodontal groove (mechanical retraction of the gums) before obtaining the final working impression in the manufacture of metal-ceramic and all-ceramic structures.
Temporary plastic crowns must meet certain requirements: restore the shape and function of the prepared teeth; ensure the viability and integrity of the tissues of the prepared teeth with minimal reaction of the tissues of the prosthetic bed; have sufficient strength and wear resistance during the expected period of production of permanent dentures; ensure the aesthetics of teeth and dentition, functional comfort with good hygienic qualities.
For the manufacture of temporary dentures, polymer materials are used: acrylates, polycarbonates, composites. Temporary crowns can be made by indirect (laboratory) and direct (clinical) methods. With the indirect method, the production of these structures is carried out by a technician from polymer acrylic materials on plaster models. The direct method of prosthetics involves making a crown by a doctor in the patient’s mouth.
The prosthesis is made by a dental technician according to the rules for making crowns on plaster models made of polymers for permanent structures. The plastic crown is fixed in the mouth, usually the next day after the teeth are prepared. A prosthesis made in this way ensures optimal marginal adaptation of the structure and occlusal relationship with antagonist teeth, minimizing the risk of toxic effects of polymers on dental tissues and the oral mucosa.
Direct (clinical) methods for making temporary structures. They are used when it is necessary to obtain and fix temporary crowns immediately after tooth preparation. The structure is made by a doctor in the patient’s mouth from polymers for temporary structures.
In recent years, CAD/CAM technologies have become widespread in dentistry. Using the CEREC-3 device, the orthopedic dentist receives an optical impression of the prepared tooth, adjacent teeth and antagonist teeth. Using a computer, the crown is modeled within 5 minutes and milled from a special plastic block within 10 minutes.
What is included in the stages of dental restoration?
Making plastic crowns is not a very complicated process. However, the dentist and dental technician must observe all the nuances of production in order for the product to cope with its function. Prosthetics consists of the following stages:
- the best method of prosthetics is selected: first, the patient undergoes an examination by a doctor, then an X-ray diagnosis follows, then the option of a permanent prosthesis is selected and/or implantation is discussed,
- preparation: diseased teeth or their roots are removed, the enamel surface is cleared of plaque and stone, root canals are prepared, the enamel is ground, an implant or pin is installed (stump inlay),
- impressions are taken,
- making a plastic crown in the office or in a dental laboratory,
- installation of a temporary plastic prosthesis for the patient.
Read on the topic: what is better to choose – implantation or prosthetics, and why?
Manufacturing stages
Clinical stages
- Tooth preparation, selection of color of artificial prosthesis
- Taking an impression, transferring the resulting material to the laboratory
- Next come the laboratory stages (listed below), the dental technician hands over the finished design to the doctor
- Initial fit in the mouth, polishing if necessary
- Fixation of the prosthesis with permanent cement
Laboratory stages
- Making models based on the impressions received (marble gypsum, super gypsum is used)
- Installation of the model in a wax template (occluder) in the position of central occlusion. Some technicians skip this step
- Making wax models
- Plastering into a ditch, getting rid of wax (digestion)
- Preparation of plastic by mixing ingredients
- Packing plastic into a cuvette, cooking (polymerization) for 45 minutes
- Removing and processing the crown, transferring the work to an orthopedist
The laboratory stages of making plastic crowns are shown in the video:
Installation features - how to install and how to remove
The plastic crown is fixed using special cement, which quickly hardens after installation. But, at the same time, the cement is not as strong as that of fixed permanent dentures. Therefore, sometimes the plastic crown falls off - if there is no damage, the doctor will be able to put it back. Before permanent prosthetics, the dentist will easily remove the temporary cap and clean the support from excess “glue” using ultrasound or special compounds.
When using prosthetics on implants, screw fixation can be used; in this case, the prosthesis will be conditionally removable (since the dentist will be able to remove it without damage). Here a small hole is created in the crown, a small screw is screwed through it, and the groove is closed on top with a filling. If necessary, the filling is removed, the screw is unscrewed, and the prosthesis is removed, changed, cleaned, and put back.
Service life
The service life depends on the manufacturing method and the characteristics of the materials used. Thus, for those manufactured by the direct method, the service life is 1-2 months. For laboratory ones – up to 1 year. For those models whose walls are reinforced with fiberglass or metal thread, as well as those made by milling, the service life can be 1.5-2 years. But, of course, if you take good care of the prosthesis - clean it regularly and do not subject it to heavy loads.
DENTAL PROSTHESIS ON 4 IMPLANTS - from RUR 170,000.
The price includes all procedures for installing Osstem implants (South Korea), including anesthesia and diagnostics.
Hurry up to sign up for a free consultation and fix your prices.
Call now or request a call
Opening hours: 24 hours a day - seven days a week
How much does prosthetics cost?
The cost also depends on the manufacturing method, the quality of the plastic and its quantity, and the method of fixation. An ordinary plastic crown made in a doctor’s office costs from 1,000 rubles. The laboratory price is already higher - from 2000 thousand. The most expensive ones are milled ones; they can cost 3500-5000 rubles.
1Vyazmitina A.V. Materials science in dentistry, 2002.
Your questions and answers
QUESTION Hello, how long can I wear a temporary plastic crown on a tooth? Svetlana
ANSWER Hello, Svetlana. It all depends on what your dentist told you and what type of prosthetic treatment you are having. Ideally, if prosthetics are on your “native” tooth, then wearing a temporary plastic crown is not recommended for longer than 2-3 weeks. It is less common to walk with her for up to 12 months. For example, if you were given an implant with a temporary crown, and now it is healing. This is a slow process that requires some time. And after engraftment, it is necessary to change the temporary crown to a permanent one - made of ceramics, metal-ceramics or zirconium dioxide.
Author: Sambuev B. S. (Thank you for your help in writing the article and the information provided)
Clinical and laboratory stages of manufacturing a plastic crown.
Answer:
| Clinical stages (performed by a doctor) | Laboratory steps (performed by a dental technician) |
| K1. Odontopreparation. 2. Obtaining an impression. 3. Determination of crown color. | |
| L1. Making a plaster model. 2. Modeling a crown from colorless wax on a manufactured plaster model | |
| K2.1. Fitting a plastic crown into the oral cavity 2. Making adjustments to the shape of the crown, size, relationship with antagonists for various types of closure of the lower jaw. | |
| L2. Final grinding and polishing of the plastic crown | |
| K3. 1.Fixing the crown on the tooth with cement (preliminary disinfection and drying). 2. If there is excess cement, remove it using a probe. |
Metal stamped crowns, indications for their use. Rules for preparing hard tooth tissues for a stamped metal crown.
Metal stamped crowns, indications for use:
1) Significant destruction of the lateral (chewing) teeth as a result of caries, wedge-shaped defects, if the defects cannot be eliminated from fillings, inlays
2) In order to correct the abnormal position and shape of the chewing teeth.
3) For fixation of fixed dentures.
4) Splinting
5) Temporary fixation of orthopedic and orthodontic devices.
6) Convergence, divergence, advancement of teeth if significant grinding is necessary.
Rules for preparing hard tooth tissues for a stamped metal crown:
Odontopreparation of 5 tooth surfaces. A layer of tissue equal to the thickness of the crown (0.25-0.3 mm) is removed from the cutting edge or chewing surface. Sharp angles between the buccal and contact surfaces are smoothed out.
As a result of preparation, the tooth takes on a cylindrical shape with a crown diameter that does not exceed the diameter of the tooth neck. This makes it easy to apply a crown, the edges of which, entering the gingival pocket, will tightly cover the tooth neck.
Clinical and laboratory stages of manufacturing a stamped metal crown.
Answer:
| Clinical stages (performed by a doctor) | Laboratory steps (performed by a dental technician) |
| 1. Examination of the oral cavity and selection of prosthesis design. | |
| 2. Treatment of the tooth for a metal crown and separation. | |
| 3. Taking impressions of the upper jaw and lower jaw. | |
| 4. Casting models of the upper and lower jaws. | |
| 5. Plastering the models into the occluder in central occlusion. | |
| 6. Engraving and drawing of the clinical neck of the tooth. | |
| 7. Tooth modeling for a metal crown. | |
| 8. Cutting out a plaster die and drawing a laboratory neck of the tooth. | |
| 9. Casting a gypsum block. | |
| 10. Casting metal dies (2 dies for making one crown). | |
| 11. Selection and heat treatment of sleeves. | |
| 12. Crown beating (pre-punching). | |
| 13. Stamping of the crown (final). | |
| 14. Crown whitening. | |
| 15. Processing and polishing of the crown. | |
| 16. Trying on a crown. | |
| 17. Fixing the crown in the oral cavity with cement, that is, handing over the crown to the patient. |
Clinical and laboratory stages of manufacturing a combined stamped crown (according to Belkin).
Answer:
| Clinical stages (performed by a doctor) | Laboratory steps (performed by a dental technician) |
| K.1. 1. Odontopreparation 2. taking an impression 3. determining the color of the future structure | |
| L.1. 1. Making a plaster working model and a metal crown. | |
| K.2. 1. fitting the model into the oral cavity, then removing it. 2.Drilling a 2mm hole on the vestibular surface. 3. Pouring wax into the crown, fitting, excess wax is squeezed out through the hole | |
| L.2. 1. making a model. 2. Heating the crown on an alcohol lamp or boiling. 3. whitening and polishing the crown, cutting out the vestibular surface, modeling it with wax 4. replacing wax with plastic 5. processing, grinding, polishing. | |
| K.3. fitting and fixation of the finished crown. |
Cast crowns, metal-acrylic and metal-ceramic crowns. Clinical and laboratory stages of their production.
Cast crowns
| Clinical | Laboratory |
| 1. Odontopreparation 0.5-0.6 mm Stump shape 3-5g. Obtaining a 2-layer print. | |
| 1. Making a collapsible model. Wax modeling of a crown. Replacing wax with metal. Processing and polishing, grinding. Sent to the clinic. | |
| 2. Fitting and fixing the finished crown using cement |
Metal acrylic
| Clinical | Laboratory |
| 1. Odontopreparation is 0.5-0.6 mm, but in the vestibular side the preparation is deeper. Obtaining a 2-layer print. Definition of color. | |
| 1. Making a collapsible model, modeling the frame, creating contact points for attaching plastic to the vestibular surface. Replacing wax with metal. Frame processing | |
| 2. fitting the crown | |
| 2. Grinding, polishing, modeling the vestibular surface using wax on plastic. Grinding, polishing. | |
| 3. Fitting and fixing the crown into the oral cavity |
Metal-ceramic
| Clinical | Laboratory |
| 1. Odontopreparation up to 2 mm Creation of a ledge. Obtaining a 2-layer print. Definition of color | |
| 1.Making time. Plastic crowns for prepared teeth. Making a collapsible model, modeling the frame, replacing wax with metal. | |
| 2. fitting the crown. | |
| 2. Manufacturing of ceramic coating | |
| 3. Fitting the crown | |
| 3. Glazing (final production) | |
| 4. Fitting and fixing the finished crown using cement. |
Pin structures and their elements. Indications for use. Requirements for the condition of the root and surrounding tissues.
Pin structures and their elements. Indications for use. Requirements for the condition of the root and surrounding tissues.
A pin tooth is a permanent prosthesis that completely replaces the crown of a natural tooth and is strengthened in its root canal using a pin.
Pin tooth elements:
1. a pin entering the root canal;
2. artificial crown.
Indications for use:
• complete absence of crowns of the upper front teeth and first premolars.
Requirements for the tooth root:
1. The root should protrude above the gum or be at its level;
2. Stopped chronic processes in the area of the tooth apex;
3. The protruding part of the root must have solid walls not affected by caries;
4. The ratio of root length to crown length is 2:1;
5. Root stability.
The root canal must be sealed up to or beyond the root apex and be of sufficient length and width.
Stump pin teeth are solid-cast structures consisting of a pin, an inlay and a stump of the tooth crown. The stump of the crown (tooth) is covered with an artificial crown.