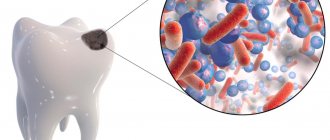
Endodontic treatment of tooth roots requires all the knowledge and skill of the dentist. After all, if even the slightest mistake is made, all subsequent work on filling and prosthetics will be done in vain. Our clinic's endodontists have extensive experience in successful root canal treatment and are proud of the good results of their work.
Reasons for performing root canal treatment are:
- deep complicated caries;
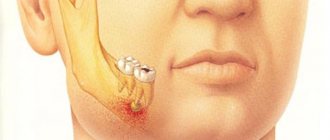
- acute and chronic pulpitis;
- periodontitis, etc.
The goal of treatment is to clean the dental ducts and put a filling so that infection does not penetrate into them.
How is the treatment carried out?
The doctor uses special tools to drill a hole in the head of the unit being restored. Through it, it removes diseased pulp and dentin, and also disinfects the outlet space, and then seals it.
There are two main processing methods:
- apical-coronal, i.e. the doctor processes the dental canal from top to bottom, from the head to the mouth of the root;
- coronal-apical, i.e. on the contrary - from bottom to top.
The key to a high-quality procedure is accurate diagnosis of the roots, which is ensured by radiography. The picture is taken before, during and after the procedure. This is necessary in order to assess the length and shape of the dental outlet as accurately as possible. After all, these indicators are individual for each person.
During the procedure, antimicrobial agents are used that have the following effects:
- destroy harmful microflora;
- improve the condition of the preserved tissues of the unit;
- do not cause allergic reactions.
Our clinic actively uses laser technologies, which give excellent results.
They carefully remove dead remains of pulp and dentin without damaging living tissue.
Leave your phone number. The clinic administrator will call you back.
By leaving a request on the site, you consent to the processing of personal data
Make an appointment
Initial consultation
400 rubles
The image shows poorly treated root canals in the lower sixth unit.
BEFORE AFTER
BEFORE AFTER
Duration of dental work
It goes without saying that the time range for performing a particular operation varies significantly depending on the complexity of the initial condition. A small filling measuring 1x1x1 mm is, of course, faster to place than to restore a completely destroyed tooth. Much also depends on the experience and manual skills of the doctor. Some doctors work at cosmic speed (up to 3 times faster than their slower colleagues), but there are only a few such unique specialists in the entire country. The third main link that significantly influences the pace of treatment is the patient’s mood and behavior. Someone obediently opens his mouth and closes it only after the entire event is completed. And some people need rest every 5 minutes, a break with auto-training, they definitely need to ask a lot of questions right during the treatment process, go to the toilet several times, make a phone call, etc. But still, the average time required for a specific operation can be predicted. Here is a table for the most common procedures in dentistry. Below are comments on some columns.
| Type of procedure | Number of visits | Average reception time | Main interval | Recommended appointment time | Total treatment period |
| Dentist consultation | 1-3 | 15 minutes | 5-60 min | 30 min | |
| Consultation with a dentist-therapist | 1-2 | 10 min | 5-15 min | 15 minutes | |
| Consultation with a dental surgeon | 1-2 | 15 minutes | 5-30 min | 15 minutes | |
| Consultation with an orthopedic dentist | 1-3 | 20 minutes | 5-60 min | 30 min | |
| Consultation with an orthopedic dentist with drawing up a treatment plan | 1-3 | 30 min | 10-60 min | 1 hour | |
| Periodontist consultation | 1-2 | 20 minutes | 5-60 min | 30 min | |
| Consultation with a periodontist with filling out a periodontal chart | 1-2 | 1 hour | 30-90 min | 1 hour | |
| Orthodontist consultation | 1-3 | 15 minutes | 5-30 min | 15 minutes | |
| Consultation with a pediatric dentist | 1 | 15 minutes | 10-60 min | 15 minutes | |
| Treatment of caries | 1-2 | 30 min | 10-60 min | 1 hour | 1-7 days |
| Placing a filling | 1 | 15 minutes | 5-30 min | 1 hour | |
| Artistic tooth restoration | 1 | 40 min | 20-60 min | 1 hour | |
| Treatment of pulpitis | 1-4 | 1,5 hour | 0.5-2 hours | 1,5 hour | 1-10 days |
| Treatment of periodontitis | 1-4 | 1,5 hour | 0.5-2 hours | 1,5 hour | 1-3 weeks |
| Unsealing channels | 1-2 | 1,5 hour | 0.5-3 hours | 2 hours | 1-7 days |
| Filling a wedge-shaped defect | 1 | 30 min | 15-60 min | 1 hour | |
| Treatment of caries in children | 1 | 15 minutes | 10-60 min | 1 hour | |
| Treatment of pulpitis in children | 1-3 | 30 min | 20-60 min | 1 hour | 1-10 days |
| Control inspection | 1 | 20 minutes | 5-40 min | 30 min | |
| Professional oral hygiene | 1 | 40 min | 20-90 min | 1 hour | |
| In-office bleaching | 1 | 1 hour | 20-90 min | 1,5 hour | |
| Home whitening | 2(1) | 15 minutes | 10-20 min | 30 min | 2-6 weeks |
| In-canal whitening | 2-4 | 15 minutes | 5-30 min | 30 min | 1-2 weeks |
| Making a crown | 2-3 | 40 min | 30-90 min | 1 hour | 1-3 weeks |
| Making a tab | 2 | 40 min | 30-90 min | 1 hour | 3-10 days |
| Making a veneer | 2-4 | 40 min | 20-90 min | 1 hour | 1-4 weeks |
| Making a bridge | 2-5 | 2 hours | 1-3 hours | 2 hours | 2-4 weeks |
| Making a crown for an implant | 2-3 | 20 minutes | 15-60 min | 1 hour | 1-3 weeks |
| Manufacturing of crowns and CEREC inlays | 1(2) | 2 hours | 2 hours | 1+1 hour | 1 day |
| Manufacturing of a removable partial denture | 2-5 | 20 minutes | 10-30 min | 30 min | 2-3 weeks |
| Making a complete removable denture | 3-6 | 20 minutes | 5-30 min | 30 min | 2-4 weeks |
| Removable denture repair | 2 | 10 min | 0-15 min | 15 minutes | 1-3 days |
| Repair of crowns, bridges | 0-1 | 15 minutes | 0-60 min | 15 minutes | |
| Cementing a fallen crown | 0-1 | 10 min | 0-20 min | 30 min | |
| Removal of a mobile, baby tooth | 1 | 5 minutes | 1-15 min | 15 minutes | |
| Removal of a tooth | 1 | 15 minutes | 5-40 min | 1 hour | |
| Wisdom tooth removal | 1 | 20 minutes | 1-60 min | 1 hour | |
| Removal of an unerupted (impacted) tooth | 1 | 30 min | 15-90 min | 1,5 hour | |
| Closed curettage | 1 | 10 min | 5-15 min | 15 minutes | |
| Open curettage | 1 | 20 minutes | 10-30 min | 30 min | |
| Closing gum recession | 1 | 40 min | 20-60 min | 1 hour | |
| Guided tissue regeneration | 1 | 40 min | 20-60 min | 1 hour | |
| Implant installation | 1 | 30 min | 20-60 min | 1 hour | |
| Single-stage implantation | 1 | 40 min | 30-90 min | 1,5 hour | |
| Augmentation (building up) of bone tissue | 1 | 40 min | 20-90 min | 1,5 hour | |
| Closed sinus lift | 1 | 15 minutes | 5-20 min | 1 hour | |
| Open sinus lift | 1 | 40 min | 15-60 min | 1,5 hour | |
| Orthodontic treatment with braces | 5-50 | 1.5 years | 0.5-3 years | 15 minutes | 1.5-2 years |
| Orthodontic treatment with lingual braces | 5-50 | 2 years | 0.5-3.5 years | 15 minutes | 1.5-2.5 years |
| Orthodontic treatment with aligners (Invisalign, etc.) | 5-15 | 9 months | 0.5-1.5 years | 15 minutes | 0.5-1 year |
Comments:
1. This refers to the time frame for one procedure: treatment of one tooth, placement of one filling, removal of one tooth, and so on. Performing two or more similar operations in one visit (especially with adjacent teeth) usually reduces the time required for each of them. So, if a doctor places a filling on one tooth in 50 minutes, he can install two fillings of the same size not in 100 minutes, but in 80. Three in 100 minutes, and so on...
2. Something can be completed entirely in one visit. In other cases, 2 or more visits are required. Zero in this column means that in a significant number of cases such manipulation cannot be performed and you need to be mentally prepared for another (more complex) one.
3. If there are several techniques and they differ significantly in time, this will be indicated in separate comments. In the absence of a comment, it should be assumed that each of the visits continues approximately the same.
4. The most common range, which includes 90% of such manipulations.
5. This is the recommended time for the initial appointment, when neither you nor the doctor yet know exactly the degree of complexity, but you can roughly guess what the first appointment will be filled with. Usually it is slightly longer than the average time, since it includes possible delays, preparatory procedures (anesthesia, etc.), recommendations and discussion.
6. This is the period from the first to the last visit for work performed in several visits. An empty column is left where there is no need to come again.
7. When it is difficult to immediately determine the required specialization of a dentist, it is better to contact a general dentist (general dentist) for the first time. Even if he is forced to send you to a more specialized specialist, he can be questioned on many other (very often also existing) dental issues.
8. Quite often, one consultation is not enough, since data from additional studies (x-rays, orthopantomograms, CT, MRI, etc.) is required.
9. The first consultation can be either shorter than subsequent ones (if it is useless to assume anything without additional research - it will be like fortune telling) or longer (when the main issues are clarified immediately, and at the second consultation only a verdict is made from 2-3 previously selected probable diagnoses).
10. The consultation may take an hour or more, but the first appointment should not take that long. It is better to conduct a complex, detailed discussion the second or third time, when the doctor at home has thoroughly “digested” the difficult case. Well, half an hour is enough to clarify basic questions.
11. Dental therapists are sometimes divided into endodontists (who treat canals) and restorers (who specialize in highly aesthetic dental restorations with filling material). The duration of their consultations is approximately the same.
12. Usually one consultation with a dental therapist is enough. But subject to the availability of the necessary radiographs or computed tomography. If they are not available, but can be done in the same clinic, then basically everything is determined on the first visit. If the required equipment is not available, then there is a need for a second consultation after the patient brings the necessary research results.
13. An implantologist is also a dental surgeon. Consultation on implantation usually lasts a little longer than on tooth extraction.
14. When planning implantation and other bone operations, computed tomography plays a key role. If you have it, it is better to send it to the doctor in advance by email. This will shorten the visit time or even one entire visit. Of course, you need to give the surgeon the opportunity to familiarize yourself with it, i.e. Make an appointment for at least the next day.
15. 15 minutes is usually not enough to study a CT scan, so send it in advance. Or at least verbally warn about the need to allocate more time to you.
16. An orthopedic dentist is a specialist whose consultation is necessary first of all in the presence of problems from different areas of dentistry. If you need to treat, remove, straighten, and replace teeth at the same time (or some 2-3 options from the above), you need to go to an orthopedist. He refers it to a therapist, surgeon, or orthodontist if necessary. It is not recommended to go to him, for example, after all your teeth have been treated by a therapist. Because some manipulations may be unnecessary. And others, on the contrary, are missing - which will require a return to the therapist.
17. If prosthetics are needed not for 1-2 teeth, but for a significant number, be prepared for the fact that at the first appointment only diagnostic impressions will be taken. And the main discussion will come next time, when the doctor (and dental technician) use the cast diagnostic models to plan the optimal treatment plan.
18. If you need a detailed treatment plan with cost calculations, then you also need to warn about this. It will take a few extra minutes to complete.
19. A dental therapist and a dental surgeon can also serve as a periodontist.
20. Filling out a periodontal chart with measurements of each tooth at at least 6 points takes significant time. Often it is not carried out on the first visit.
21. The first consultation with the orthodontist is introductory. It can be used to photograph and take diagnostic impressions. After calculating the diagnostic models, that is, at the next visit, a substantive discussion of the treatment plan will take place.
22. The examination itself, diagnosis and discussion of treatment with parents in most cases takes 15 minutes. But the time it takes to establish contact with a child (find an approach to everyone, don’t scare them, get permission to open your mouth) can vary greatly depending on the age, temperament and mood of the little patient. Each pediatric dentist determines it himself. Some people believe that if an agreement cannot be reached in 15 minutes, then further attempts are futile. Other doctors are ready to patiently adjust the child and take twice or three times longer.
23. Treatment of caries most often ends with the installation of a filling. But if the tooth is more than 50% damaged, an inlay or onlay is recommended.
24. In one visit, caries is treated if a filling is installed. If an inlay or onlay is being made, 2 visits are required. Also, sometimes in case of deep caries and suspicion of pulpitis, a permanent filling is not placed immediately, but the patient is allowed to find and observe the tooth for a week.
25. Treatment of 2-3 adjacent teeth significantly shortens the average time for each of them. Since one anesthesia and one application of a rubber dam is enough, carious tissue on contact surfaces is removed more easily and quickly.
26. In general, placing a filling is only part of the procedure for treating caries, wedge-shaped defects, traumatic chipping of a tooth, etc. Before installing a filling, the tooth must be prepared in one way or another. But sometimes there are cases when this preparation is minimal (takes less than a minute).
27. Although (as can be seen from the other columns of this line) the time for filling a tooth in most cases does not exceed 30 minutes, often additional manipulations take almost the same amount. Therefore, when making an appointment for a filling, it is better to reserve 1 hour.
28. Artistic restoration is a filling with special additional characteristics.
29. An artist can paint his picture for decades. Also, a dental artist, in principle, is not limited by time for sculpting a masterpiece. But still, usually some reasonable limits are respected.
30. Treatment for pulpitis varies greatly in duration. And by the number of visits, and by the time of each of them. Firstly, there are 2 methods of treating pulpitis: vital (when the pulp is removed during the first visit under anesthesia) and outdated, but rarely used devital (when “arsenic” is first applied, and depulpation is resorted to directly on the second visit). Secondly, the pace of treatment strongly depends on the number of canals: there can be from 1 to 5 of them in a tooth. Thirdly, some doctors permanently fill the canals on the first visit (most), others put a temporary drug in the canals, and the final filling channels will be carried out next time. Fourthly, the smartest dentists try to sculpt a filling for a newly treated tooth already on the first visit. Others postpone this stage to another day, or even recommend restoring a pulpless tooth not with a filling, but with a more serious structure - a crown, inlay, onlay (which is correct).
31. Thus, everything fits into one visit when the removal of the pulp (under anesthesia), filling the canal with permanent material, and restoring the tooth with filling material are carried out immediately. There will be 4 visits if: first, arsenic is applied, then the pulp is removed and a temporary preparation is left in the canals, then the canals are completely filled, and finally, the tooth is restored with a permanent filling (but this scenario is rare). If agreement is reached to restore the tooth not with a filling, but with an orthopedic construction, then more visits may be required. But they will relate to the treatment of pulpitis only indirectly. Therefore, we do not take them into account here; they need to be added additionally, looking at the corresponding rows of the table.
32. Approximately 1.5 hours are needed to treat a single-canal tooth entirely or a 3-4-canal tooth without final restoration (a permanent filling is placed at the next visit).
33. If the doctor does not meet the deadline in an hour and a half, he always has the opportunity to stop at some stage: put the medicine in the tooth and put a temporary filling. And complete the labor-intensive processing of the canals on your next visit.
34. As with pulpitis, treatment of periodontitis can take varying amounts of time and number of visits. In addition to the variety in the number of canals and the possibility of transferring the final restoration of the tooth to a separate visit for periodontitis, in most cases the canals are not completely filled at the first appointment. It is not so much the tooth itself that needs to be cured, but the inflammatory tissue around it (cyst). This usually takes 2-3 weeks. But some doctors consider it advisable to add a fresh portion of the drug (calcium hydroxide) several times. Two or three times or even several months - until they are completely sure that the bone tissue around the tooth has healed. On the other hand, among dentists there are also supporters of treating periodontitis in one visit (in some situations they achieve no less success than those who adhere to multi-visit tactics).
35. One visit - if the canals are immediately processed, filled with permanent material, the tooth is restored with a permanent filling. 2 visits - this is if, according to the classical treatment regimen, the treatment is carried out with temporary injection of Ca(OH)2 into the channels. In 3 or more appointments - when the antiseptic is changed several times, or tooth restoration takes a separate stage.
36. Unsealing the canals is necessary for periodontitis, when the tooth has previously been treated endodontically, but the treatment did not give a successful result. This type of work in most cases is much more complicated than primary intervention for periodontitis. Because instead of empty canals, the dentist must treat those previously filled by the previous doctor. This is often very difficult and unpredictable. You can go through the canal to the top in one minute, or you can not even advance a quarter of the length in a whole hour. It all depends on the material and the efforts of the previous doctor: it is very difficult (and sometimes even impossible) to remove cement or resorcinol-formalin paste from the canals. An attempt at forced unfilling can only lead to the formation of perforation (false channel), which will completely minimize the chances of saving the tooth. Therefore, to reduce risks, such manipulation must be carried out carefully, without fanatical use of force. Theoretically, the time and number of techniques are unlimited, but in practice, extra effort can only be spent up to a certain limit. This limit is individual for each doctor and patient. But for most, average numbers can be derived in this situation.
37. Usually, on the first visit, either the canals can be unsealed, or a decision is made that further attempts are inappropriate. But if there are some intermediate results, the chances of achieving success a second time are relatively high - you can continue the work you started in the second round.
38. Unsealing canals is a monotonous procedure. For many patients, sitting with their mouth open in the dentist’s chair for more than 2 hours is difficult. By reducing the dose to one hour, there will be little chance of achieving a good result.
39. Before you begin to remove the filling material itself from the canal, you need to drill out the old filling, and sometimes remove the pin.
40. Since fillings for wedge-shaped defects last less, and many doctors warn patients about this without providing a guarantee, there is a tendency among dentists to place them less responsibly. And, accordingly, faster than it should. In fact, the approach to treating a tooth and isolating it with a cofferdam should be no less thorough than when treating caries. Even, perhaps, more careful - after all, it is more difficult for a filling to hold onto a wedge-shaped defect, and therefore the installation technique will not forgive even small errors.
41. Here we are talking, of course, not about silvering, but about the full treatment of caries by filling a tooth.
42. One hour is needed to form a trusting relationship with a child. The younger the patient, the more time it takes to persuade.
43. Pulpitis of baby teeth is treated according to a simplified scheme. The canals are not treated as thoroughly as permanent teeth. With pulpitis of a permanent tooth, the treatment time for the canals is also shorter than in adults, since they are wider.
44. Technologies of vital (in one visit) and non-vital (in two visits) treatment are found in both permanent and baby teeth. Tooth restoration with a filling can be carried out at the second or third appointment.
45. The patient should come for a follow-up examination to the dentist every six months (unless more often was recommended). Depending on your specialization, the examination should be carried out either by the specialist you primarily visited (general practitioner, orthopedist, periodontist, orthodontist) or by a general dentist (generalist).
46. This refers to the time spent brushing all your teeth at once. The procedure includes air-abrasive treatment (Air-Flow), ultrasonic cleaning and polishing of teeth with paste.
47. In rare cases, if patients are hypersensitive, it must be performed under local anesthesia - then it is more advisable (in order not to do many injections at once) to split the procedure into 2 visits. The first one cleans the upper jaw, the second one cleans the lower jaw. Or vice versa.
48. The amount of tartar and plaque varies from patient to patient. It depends on the quality of personal hygiene and the duration of the last professional cleaning. If you haven’t brushed your teeth at the dentist for many years and plaque is clearly visible even on the front surface, then be mentally prepared for a longer appointment.
49. This is whitening in the dentist's chair.
50. Usually pure procedure time: 3-4 times x 15 min = 45-60 min. But with increased tooth sensitivity, not everyone can withstand the allotted time completely and stop the process earlier. Anesthesia for whitening is not recommended.
51. You do home whitening at home yourself, but you need a dentist to make individual trays into which the whitening preparation will be applied.
52. Whitening trays are made approximately 1.5-2 hours after taking impressions. You can wait or have an in-office whitening session at this time. Or you can come separately and just pick up the finished mouth guards.
53. This is the period for home whitening itself. Some people's teeth respond to lightening faster, others slower. The initial coloration and sensitivity of the teeth also affect the duration of the procedure.
54. Endodontic whitening is performed only for pulpless teeth. The whitening agent is placed inside the tooth, covered with a temporary filling, and the patient wears it for several days.
55. If the effectiveness of whitening the first time turns out to be insufficient, you can repeat the procedure one more time or two.
56. We are talking about a permanent crown made of metal-ceramic or all-ceramic. The production of a temporary crown is included in the specified average time (this is mandatory).
57. Ideally, the crown is made in 2 visits. In the first step, the tooth is prepared, impressions are taken, and a temporary crown is made. In the second, a permanent crown made in a dental laboratory is tried on and fixed with permanent cement. But this is only if all the parameters are performed perfectly the first time. In reality, you often have to adjust, fix, or improve something. This is especially true for prosthetics of front teeth. It is possible to satisfy all the aesthetic needs of the patient on the first try either if you have an outstanding dental technician, or if these requests are completely unpretentious. Therefore, not two, but three visits should be considered quite normal - the crown adjusted by the technician should be much closer to high quality standards.
58. The first appointment lasts longer than the second or third. But if the crown is fixed with composite cement, then the final visit may take about an hour.
59. The most common time for making a crown in a dental laboratory is 2 weeks. Of course, if the laboratory has little work to do, you can make a crown faster. But a good laboratory rarely experiences a lack of orders. Therefore, as a rule, she asks for increased payment for accelerated execution.
60. There are 2 types of inlays: stump and coronal. Both take approximately the same time to produce. This also applies to overlays.
61. The core inlay is usually produced more quickly. But, as in the case of crowns, the workload of the laboratory also plays an important role.
62. A veneer is a laboratory ceramic restoration on the front surface of a tooth. In this case, the inner surface is not ground down or is only partially ground down (this is its difference from a crown - it requires preparation of the tooth from all sides). Lumineers are a subtype of veneers. Initially it was just a commercial name for the product. Now other companies offer their products under this brand.
63. Veneers, by definition, require a particularly scrupulous attitude to aesthetics. Therefore, additional color and shape corrections with this type of work are the rule rather than the exception. 2 visits are a big success, 3-4 are quite normal.
64. Since veneers are often ordered more than one at a time, the more of them there are, the less time is spent on average on one tooth.
65. A bridge prosthesis consisting of three units (two crowns on the supporting teeth and an artificial tooth located between them) is the easiest to make. In this case, two visits may be enough. But the longer the prosthesis, the more complex the production process. Therefore, more visits may be required before the aesthetics, comfort, and fit of the prosthesis are achieved.
66. The first appointment, at which impressions are taken, lasts less than when installing a crown on a tooth - because there is no need to grind anything down. The second or third visits take about the same time.
67. This technology makes it possible to perform an orthopedic design without the participation of a dental laboratory. The doctor takes an optical impression, models the future crown or inlay on a computer, and a milling machine cuts out a part of the desired shape from the blank. Then the dentist paints the restoration, giving it individual features and fixes it in the oral cavity.
68. Since the main advantage of such production is speed, often all the work is done within one day. After taking impressions, the patient awaits the results right in the clinic (or walks nearby). But you can, of course, come for final cementing the next day.
69. Partially removable dentures are used when at least one (or several) teeth are present on the jaw. Plastic plate, clasp, locking, nylon (flexible) dentures - their production time does not depend on the material.
70. Taking impressions, determining the bite, fitting the frame (for clasp and locking dentures), trying on the teeth and, finally, handing over the finished prosthesis - these are the main stages of making removable dentures, each of which requires a separate visit. True, if there are a few missing teeth, some of them are reduced.
71. A complete removable denture is made when there is not a single tooth left on the jaw.
72. These figures do not take into account the visits required to adjust a prosthesis that has already been delivered. Immediately after starting use, the prosthesis almost always chafes here and there. Therefore, you need to come back one to three times to eliminate areas that injure the mucous membrane.
73. It is not always possible to repair a removable denture. If the doctor considers it possible, he takes an impression of the prosthesis and sends it to the laboratory. Sometimes you don’t even need to take an impression (for example, if only a crack has appeared on the prosthesis).
74. Repair of a fixed structure (crown, bridge) is rarely feasible. The only thing that can be done is to cover a small chip in the ceramic with a composite filling material. And even then: the service life of such a “patch” is short-lived.
75. Crowns never fall out without a reason. Patients almost always resort to low-quality cement in the hope that a new “stronger” one will be able to hold a seemingly good restoration for a long time. In fact, in 99% of cases, it is not cement that causes the loss, but poor-quality manufacturing of the crown itself. Therefore, in the vast majority of situations, it cannot be cemented again - you need to make a new one.
76. Sometimes patients confuse a mobile tooth (whose root is mobile) and a broken wall. The swinging wall of a fracture can be easily removed in a minute, but the root itself will most likely be far from easy to remove. There is also confusion with baby teeth - it is easy to remove such a tooth during the period of physiological change, when its roots have practically resolved. But if a baby tooth has to be removed several years earlier, then the removal may be similar in complexity to tooth extraction in adults.
77. The removal time is influenced by many factors, so it can vary quite a lot. Speed is not the main thing - it is much more important to carry out the operation as less traumatic as possible, so that healing takes place without complications. And subsequent implantation can be carried out without additional augmentations.
78. Removal of the upper wisdom teeth usually takes place faster than the removal of the lower ones. But in any case, it is recommended to take an x-ray before the operation in order to understand the degree of complexity in advance.
79. Before removing such a tooth, you still need to get to it. An incision is made in the gum, the bone tissue above the tooth is excised, and the tooth itself can be sawn into several parts. After the tooth is extracted, the gums are sutured. The further the wisdom tooth is from the surface, the more difficult and longer it will take to remove it. A preliminary x-ray is required (or even better - a computed tomography).
80. After 7-14 days, you still need to come back once to remove the stitches, but here it is indicated how many visits the operation itself will take.
81. Closed curettage is the main method of treating mild forms of periodontitis. Periodontal pockets are cleaned using Gracie curettes or ultrasound.
82. Open curettage is indicated for moderate periodontitis. In this case, an incision is made in the gum, a flap is peeled off, the root surface is processed under direct visual control, and sutures are applied at the end.
83. The “gold standard” for closing gum recession is the transplantation of one’s own connective tissue (gingival) graft into the area of the exposed root neck. There are also alternative methods when a second surgical field is not used - they are performed somewhat faster.
84. Here we mean an operation with a deep periodontal pocket, when, after curettage of its contents, bone tissue (or its substitute) is introduced and a membrane is installed.
85. Of course, we are talking about root-shaped screw implants here. Basal, lamellar and other marginal types of implantation are not considered.
86. With single-stage implantation, after tooth extraction, the implant is immediately installed in the socket.
87. If there is a lack of bone tissue, its volume must be increased before installing the implant. This is achieved by a separate operation, which can be carried out in several ways.
88. Sinus lift is moving the bottom of the maxillary sinus upward. It is performed when there is a lack of bone tissue in height in the area of 4-7 teeth of the upper jaw. A closed sinus lift is indicated for minor bone deficiency. This is a simple procedure and is performed immediately before the implant is installed.
89. Open sinus lift is a separate operation. Used for significant atrophy of bone tissue. Typically, implants are installed after a few months, once the success is confirmed.
90. Here we will indicate the time costs not for a single visit (they are quite simple: 15 minutes, with the exception of the visit when braces are installed), but for the entire treatment. This period is of much more interest to patients.
91. Ligature braces require visits to the orthodontist every 2-3 weeks. Self-ligating (ligature-free) braces - once every 1-3 months.
92. At the first appointment, the orthodontist never fixes braces. And when that day comes, the doctor himself will select the required interval. Installing braces can take up to 2 hours.
93. The duration of treatment with lingual braces is approximately six months longer than with vestibular braces.
94. Aligners are clear, removable aligners. Effective for minor bite pathologies.
95. The patient receives a set of mouth guards, which he changes at home every 1-2 weeks. You need to visit the orthodontist for follow-up examinations once every 1-2 months.
Installing a seal
The dentist selects a suitable filling material, which must meet the following requirements:
- have antimicrobial, hypoallergenic properties and high biocompatibility;
- be plastic and airtight at the same time;
- Do not dye the fabric of the unit being restored.
The filling material is varied:
- hardening;
- non-hardening;
- pins made of silver, titanium, gutta-percha, plastic.
When installing a pin, sealants and fillers are used, which are most often made from epoxy resin. First, the doctor uses an endodontic needle to place material into the prepared canal, then the top of the filling is compacted, excess material is removed, polished and adjusted to the bite.
Dental treatment at Dr. Granov’s dental clinic means high quality services and an individual approach to each patient.
There are several categories of causes of caries in humans.
The answer to the question of how to treat dental caries depends on the cause of such a disease. It is also very important to eliminate potential conditions for the development of tooth decay.
There are several reasons that can stimulate the appearance of damage to enamel and soft tissues:
- Severe bacterial plaque. It occurs when a person does not properly care for his teeth. It is very important to maintain regular oral hygiene, brush your teeth properly, and use floss.
- Tartar. It can also form if the patient does not comply with the rules of oral hygiene. If the stone is not removed in a timely manner, the lesion will constantly progress and spread.
- Poor nutrition. Risk factors include consuming large amounts of sweet and sour foods. Also on the list of dangerous foods are foods high in carbohydrates and starch. When consuming a large amount of low-quality and unhealthy food, tooth enamel gradually begins to become thinner. Because of this, under the influence of bacteria, the risk of caries becomes increasingly noticeable.
- Decreased saliva production. Under normal conditions, a person produces up to two liters of saliva per day. It is necessary so that food debris can be washed off the surface of the tooth. When the salivary glands do not function properly, these residues remain and the risk of bacterial growth increases.
- Lack of minerals in food. The human body either does not produce many useful substances that are needed to strengthen bones and tooth enamel, or receives them in small quantities. The list of main substances that must be obtained from foods includes fluorine, calcium, and phosphorus. At the same time, genetics also leads to problems for some people. Some people are simply genetically predisposed to accumulate a minimum of nutrients.
- Pregnancy. At different stages, there is a possibility that the fetus takes a lot of useful substances from the mother. She begins to experience a severe lack of minerals.
- Diseases of the body. Patients with systemic pathologies that directly affect metabolic processes are also at risk. Particularly dangerous are variants of diseases such as lesions of the thyroid gland, peptic ulcers, diabetes mellitus, gastritis, and imbalance of hormones in the body.
Another factor in the development of caries is the poor environmental situation in a person’s place of residence. It can stimulate the development of caries, rapid damage to both hard and soft tissues.
For this reason, a high incidence of caries is observed in regions where there are a lot of acids, heavy metal salts, and alkali vapors scattered in the air.
In order to develop a treatment method in a certain situation, it is necessary to understand what reason for the development of the disease is relevant in the case of a particular patient.
The fact is that often it is chronic diseases, improper oral hygiene, and lack of nutrients that can trigger the recurrence of the disease. In any situation, it is very important to eliminate the cause itself.
Methods for preventing caries
Doctors note that many cases of caries can be avoided if a person pays close attention to his health. There are several basic tips that will help you protect your body:
- Try to balance your diet. You need to reduce the amount of foods high in carbohydrates, sugar and starch in your diet. Sugar also negatively affects the condition of teeth.
- Pay attention to the quality of oral hygiene. Be sure to brush your teeth regularly and at the same time observe the duration and method of brush movement. It is also recommended to pay attention to what kind of toothpaste you use, use irrigators, rinses, and dental floss.
- Visit your dentist regularly. Regular medical examinations are very important. In this case, it will be possible, if not completely protected, to get rid of most oral problems at an early stage.
Our doctors will conduct a thorough examination of the oral cavity and give additional recommendations on hygiene and caries prevention.
Is it painful to treat root canals?
Thanks to the use of modern anesthetics, root canal treatment has become a painless procedure. The patient may feel mild discomfort only during the injection of the anesthetic.
Therefore, there is no need to be afraid of root canal treatment; moreover, you must remember that you should never postpone the procedure due to fear of the dentist! Inflammation in a tooth that has progressed to a certain stage of development cannot be cured, which means that the diseased tooth will have to be removed and a prosthesis put in its place. In addition, more serious complications may occur.
What happens if the implant does not take root?
Implant failure is difficult to prevent. The causes of the pathology may be peri-implantitis, smoking, non-compliance with medical recommendations in the early and late postoperative period. If acute rejection occurs, removal of the titanium rod is indicated. Re-implantation is possible only after complete healing of the wound. Rejection can develop several years after the permanent crown is installed. A number of external and internal factors can provoke a pathological process and destabilization of the implant.
Braces: wearing time depending on pathologies
How long to wear braces depends directly on your bite. Orthodontists use a special classification according to Engel, where anomalies of the dentofacial rows are divided into three groups.
The first class includes minor defects. Wearing braces can restore the correct bite in 6-12 months for pathologies:
- medium-sized diastema - a gap between the front teeth;
- crowding of the front incisors - there is not enough space for the permanent teeth due to the insufficient size of the dental arch;
- trema – interdental spaces remaining after a complete change of bite;
- transposition, dystopia - tooth eruption in the wrong place.
Rodikova Tatyana
Serious bite corrections require not only correction of the position of individual teeth, but also the formation of jaw arches. That is why the process is lengthy and requires the use of rigid orthodontic arches, elastics, and numerous techniques.
Correction of a bite with the listed anomalies is quick, especially at a young age and with the correct selection of a brace system. If we compare how long a 13-year-old child needs to wear braces and an almost adult 18-year-old patient, then the speed of treatment in the first case will be higher.
Long-term wearing of braces will require pathologies belonging to the second and third classes. Among them are the types of bite:
- distal – the lower jaw is underdeveloped, and the upper jaw is too large;
- mesial – there is underdevelopment of the upper jaw with a lack of size of the lower jaw;
- open - some of the teeth do not close, which increases the load on the rest;
- deep – the lower teeth are hidden under the upper ones, completely covered by them;
- cross - the incisors cross when the upper and lower jaws meet.
Correcting the listed problems is more difficult, so wearing braces requires two to three years, followed by consolidation of the result for another 4-5 years.