- Author:
Naumovich Yulia Yakovlevna - Specialty:
Dentist-orthodontist - Category:
Doctor of the highest qualification category
Learn more about the doctor Get a consultation
Adentia is a complete or partial absence of dentition due to a congenital malformation or acquired/transferred diseases. In turn, complete absence of teeth is very rare. Partial tooth loss is more common, accounting for 45–75% of the total number of dental diseases. Complete edentia is usually associated with age-related changes and occurs in people over 60 years of age. This pathology is unpleasant not only due to a violation of the aesthetics of the smile, but is also primarily dangerous due to serious disturbances in the gastrointestinal tract, deterioration of diction and irreversible changes in the dental system.
Classification of edentia
In dentistry, several types of adentia are differentiated. Based on the time of onset and etiology of the disease, the following are distinguished:
- primary (congenital);
- secondary (acquired);
- edentia of permanent and temporary teeth.
If the patient does not have the rudiments of teeth, he is diagnosed with “congenital adentia.” In some cases, adjacent crowns grow together. And in this case, “false adentia” is diagnosed. Partial edentia means the absence of no more than 10 teeth. Otherwise, a multiple form is observed.
There is also a Kennedy classification of the disease. According to it, the following defects are distinguished:
- double end;
- one-sided end;
- included defect in the lateral areas of the dentition;
- included defect in the anterior part of the dentition.
Partial secondary adentia: what is it?
Partial secondary adentia is a very serious stage of the disease. The patient is diagnosed with the absence of 5 to 17 teeth in one jaw. This disease is observed in 50-75% of people over 60 years of age. Secondary partial adentia is not only an aesthetic defect, but also a serious disruption of the functioning of the dental system. In addition, a person’s diction and articulation, the functioning of the gastrointestinal tract are impaired, psychological disadaptation occurs, and a person’s social behavior changes.
Secondary partial edentia can provoke atrophy of the facial muscles if the disease is neglected and you do not contact specialists. If two or more teeth are missing in the upper or lower jaw, the adjacent teeth will begin to shift. All this will negatively affect chewing food. With secondary partial adentia, the bone tissue of the tooth will quickly deplete, because the remaining teeth will be subject to a very strong load.
If partial secondary edentia begins to progress and tooth loss continues, the process takes on a multiple form. If treatment is not started in time and the causes are not eliminated, then the pathology can lead to the loss of all remaining teeth.
The edentulous disease itself can be divided into several types:
- Primary complete edentia. A serious pathology, but it can be found very rarely. It appears in milk and permanent teeth. The patient does not have a single tooth germ.
- Primary partial edentia. It appears quite often. One or more teeth are missing. The place where the tooth should be remains empty. Underdevelopment of the jaw occurs due to lack of teeth.
- Secondary complete edentia. If all the teeth below and above are lost. They may fall out or be removed during treatment. This includes both permanent and baby teeth.
- Secondary partial edentia. Frequent illness. Some teeth are missing.
Classification of secondary partial edentia
In turn, partial secondary adentia has its own classification:
- First grade. The presence of a bilateral end defect;
- Second class. Unilateral end defect;
- Third class. There is a one-sided included defect;
- Fourth grade. Secondary partial adentia is characterized by the absence of front teeth.
Partial secondary adentia: localization
According to the location of the pathology, they are divided into:
– secondary partial edentia of the upper jaw;
– secondary partial edentulism of the lower jaw.
Prevention of edentia
By following simple preventative measures, you can avoid serious health complications that can be associated with edentulism. Thus, the risk of developing primary adentia in the fetus can be minimized by strictly following the rules even at the stage of pregnancy planning and immediately at the time of bearing the child. It is necessary to monitor calcium levels and eat enough foods rich in this element for the normal development of the baby. If your child has not been teething for a long time, it is necessary to make an appointment with a pediatric dentist.
To prevent acquired adentia, doctors recommend regularly visiting the dental office for examinations, as well as thoroughly cleaning the oral cavity twice a day and professional sanitation at least once every six months. If for some reason several teeth have already been lost, then you should not hesitate with prosthetics or implantation. It is necessary to find out the cause of tooth loss and eliminate it, restoring the integrity of the dentition.
Causes of edentia
The causes of gaps in the dentition can be explained by congenital developmental disorders. In this case, primary adentia is observed due to an anomaly in the embryogenesis of dental tissue. In this case, the rudiments of teeth simply do not form. There is also a hereditary factor for the disease, in which there are problems with the eruption and formation of impacted teeth.
However, the most common cause of secondary adentia is caries and periodontal pathology. Common reasons for tooth extraction are:
- therapeutic treatment errors;
- the presence of chronic inflammation;
- destruction of the crown by more than 50%;
- cyst formation;
- necrosis of hard tooth tissues;
- neoplasms in the jaw.
We know how to cure adentia
In the near future, a medical coordinator will contact you and advise you on the conditions and cost of treatment, select a doctor and make an appointment for you.
| Make an appointment | Or call us +375 29 699-03-03 +375 33 319-03-03 |
Tooth root resorption - symptoms and treatment
Treatment is aimed at eliminating the causes of resorption and its consequences, as well as restoring tooth function.
There is no standard treatment protocol for root resorption. The method will depend on many factors: the type of resorption, the size of the lesion, the condition of the pulp and the availability of adequate access.
Internal resorption. This form of the disease is treated by filling the root canals with gutta-percha using mineral trioxide aggregate (MTA) and composite sealants.
Doctors often use temporary filling materials containing calcium when treating resorption. However, such canal filling for a long period (more than three months) can reduce the elasticity of dentin and lead to the formation of tooth root cracks [32].
In case of internal resorption with perforation, which communicates with the oral cavity, surgical treatment is performed: a mucoperiosteal flap is cut out and peeled off, and the pathologically altered tissue in the area of resorption is removed using a diamond bur. The hole in the tooth root is closed with a special material, then the mucoperiosteal flap is sutured. The period of tissue restoration is individual for each person, but on average it is 2–3 weeks.
External inflammatory resorption. When treating such resorption, it is imperative to eliminate the cause of its occurrence - infection. To do this, it is necessary to carefully mechanically and medicinally treat and seal the root canals. You can place a temporary filling with calcium for three weeks. When there is inflammation in the root canals, a local pH shift occurs to the acidic side, and a temporary filling with calcium creates an alkaline environment and thereby destroys bacteria. The process may be accompanied by a slight aching pain.
Replacement resorption. It is impossible to stop this type of resorption. The rate of tooth replacement with bone tissue depends on age: the younger the patient, the faster resorption will occur. In adults, a tooth may retain its function for many years before it is completely replaced. It is recommended to follow a wait-and-see approach. When the crown of the tooth is supported only by the dentogingival attachment, it will need to be removed, then an implant should be installed [6][27].
To prevent or delay the development of replacement resorption after complete tooth avulsion and replantation, Emdogain can be applied to the root before returning the tooth to its socket [8].
Cervical resorption . The most effective treatment for cervical resorption is removal of the affected tissue. After this, the tooth defect is treated according to the principles of carious cavity preparation and the anatomical shape of the tooth is restored [19].
This type of resorption is treated using the “sandwich technique” using glass ionomer cements and composite materials, as well as using MTA (mineral trioxide aggregate) as a disinfectant and biocompatible material that has a positive effect on the treatment outcome.
Symptoms
Symptoms of primary adentia
Congenital absence of teeth is an extremely rare disease. This pathology is revealed in the deformation of the facial skeleton:
- shortened upper lip;
- disproportionate facial height;
- pronounced supramental fold.
Against this background, there is dryness of the mucous membrane and pallor of the integument, and problems with pronunciation. Children with this diagnosis also have problems with underdeveloped nail plates, they have little hair, no eyebrows, the fontanelle does not heal well and the palate is flat.
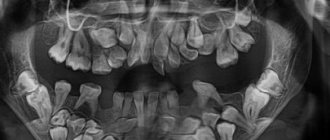
Partial primary adentia can develop due to the absence of some primary teeth. During the examination, the doctor diagnoses that they cannot be felt and are not visible on X-ray images. In this case, the patient has large gaps between the existing teeth, which leads to displacements of the entire row. If a lot of teeth are missing, the doctor may even diagnose underdevelopment of the jaw.
Symptoms of secondary adentia
The absence of teeth in the lower and upper jaw is a consequence of their surgical removal due to oncology, periodontitis or advanced forms of caries. In this case, atrophy of the alveolar processes occurs, and the lower jaw moves towards the nose.
Partial tooth loss is the most common phenomenon, as more than 70% of people experience it. In this case, teeth are removed due to periodontitis or advanced caries. Lack of proper therapy leads to dangerous complications:
- formation of a traumatic node;
- tissue destruction;
- formation of pockets near teeth;
- retraction of the upper lip and cheeks;
- dislocation of the temporomandibular joint.
Etiology
Pathological root resorption can be initiated by many factors, acting separately or simultaneously.
Such factors may be chronic inflammatory diseases of the pulp, tooth trauma, chronic periodontal diseases or orthodontic treatment [27]. Resorption can also be caused by pressure from supernumerary teeth, surgical interventions near the root system, incorrect endodontic treatment and aggressive teeth whitening [5, 6, 19, 25, 27, 30, 43, 66].
Cases of resorption occurring against the background of somatic diseases such as scleroderma [23, 60], pathologies of the endocrine system [13, 42, 54] and viral diseases [7] have been described.
Cases of multiple idiopathic tooth root resorption have also been reported [10, 40, 41, 73].
Diagnosis of edentia
Making a diagnosis does not require serious research or additional tests. A careful visual examination by a specialist and an x-ray of the jaw are sufficient.
Additional examinations may be needed to identify factors that interfere with prosthetics:
- inflammatory process;
- tumor;
- damage to the oral mucosa;
- exostosis.
During the examination, the doctor pays special attention to clarifying the nature of the origin of adentia - primary or secondary. For this purpose, radiography is usually prescribed.
Treatment of adentia
Restoration of the dentition in case of edentia is carried out by installing dentures. For this purpose, the patient is offered removable plate, bridge or clasp dentures.
Bridge-like fixed prostheses
Orthodontic structures that are attached to the supporting teeth in the jaw and replace missing units, performing their chewing function. Treatment of edentulism with the help of these prostheses allows you to restore a person’s nutritious diet, eliminate problems with diction and restore the aesthetics of a smile.
Removable plate dentures
Plate dentures are installed on existing teeth, evenly distributing the chewing load and pressure on the jaw. The method demonstrates an effectiveness of 60–80%, since wearing a prosthesis requires developing a habit within 2 months, as well as some restrictions in eating your favorite foods. This treatment option is recommended to eliminate phonetic defects in pronunciation and restore the attractiveness of a smile.
Clasp dentures
The support for these dentures is the mucous membrane and natural teeth. The special design promotes uniform distribution of chewing pressure and is characterized by biocompatibility and hygiene. Clasp dentures help eliminate all defects in the dentition.
Bite deformation with partial absence of teeth
The condition of the dental system with partial absence of teeth is a topic for a separate discussion. Even the loss of one tooth leads to displacement of the entire dentition. In this way, the body tries to restore the correct load distribution. This process begins in the immediate vicinity of the lost tooth, but over time, the deformation of the dentition with partial absence of teeth becomes more and more pronounced, especially when a significant number of them are lost. The most accurate classification of changes in the position of teeth during edentia was proposed by Dr. E. I. Gavrilov.
Classification of partial absence of teeth according to Gavrilov
- Vertical movement (lengthening of teeth). Often occurs when antagonist teeth are lost.
- Mesial and distal movement.
- Oral and vestibular movement of teeth.
- Combined movement of teeth (rotation with tilting, fan-shaped divergence, etc.).
Correction of dental deformations occurs using orthodontic, orthopedic and surgical techniques. In case of serious disorders, the installation of a prosthesis or implants may be postponed. Determination of occlusion in case of partial absence of teeth includes the calculation of occlusal height, prosthetic plane, height of the lower part of the face and the central relationship of the jaws.