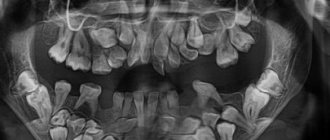
232 teeth, both embryonic and fully grown, were removed from the mouth of an Indian teenager in a clinic in Mumbai, India. Hyperdontia is the diagnosis the doctors gave him after all the clarifying procedures and exclusion of a malignant neoplasm. And all the supernumerary teeth were extracted during a 6-hour operation. The guy recovered and then returned home, taking his former hyper set of teeth with him as a souvenir.
Hyperdontia may also be called in different sources:
- Polyodontia.
- Supradentia.
- Hyperdentia.
Causes of hyperdontia
Experts do not have a unified theory for the occurrence of this abnormal dental condition. There are 4 recognized versions of the causes of hyperdontia, each of which has the right to exist:
- Embryonic splitting of the root germ of the tooth. It can only be considered as a version if a single, or at most double, splitting occurred. This means that the failure to duplicate the roots of the teeth occurred in the womb, before childbirth, and was caused by some illness during this period.
- Formation of tooth germs beyond the set provided by nature. The reason is the same as in the theory of embryonic splitting during the prenatal period of development. Only the mother had to suffer a very serious illness with treatment with potent drugs. Or in the area of her residence, a critically unfavorable environmental situation is observed from year to year.
- Heredity factor. If the parents had hyperdontia, the risk of its manifestation in the child increases by 2-3 times.
- Manifestation of atavism. Our distant primitive ancestors had not 4, but 6 incisors in each jaw in their mouths. Proponents of the theory of atavism believe that this is an attempt by nature to return the body to its original version of development. True, the atavistic theory cannot explain the appearance of extra molars.
Judging by the statistics collected on hyperdontia, the theory of environmental pollution has the greatest chances. Which, however, is quite consistent with the 2nd and 3rd hypotheses. This is supported by the fact that now the frequency of such developmental disorders has increased, and on a global scale, cases of hyperdontia account for up to 2% of the total number of inhabitants. A huge number if you think about and remember the total number of inhabitants of the Earth.
Prevention of dental diseases
Some people are not even aware of what dental diseases with inflammatory processes and pathologies are provoked in other vital organs. For those who are not in the know, we inform you: these are gastritis, ulcers, tonsillitis, thrombosis, heart attack and stroke! And the pathogenic bacteria are to blame for everything, which, multiplying in the oral cavity, enter the throat, stomach, blood vessels and even the heart.
To prevent dental diseases, follow simple rules that will help significantly improve your oral health and overall well-being.
- Stop smoking.
A bad habit provokes vasoconstriction and deterioration of blood supply to the mucous membrane, which results in a lack of nutrients necessary for teeth and gums. - Eat a balanced diet.
The abundance of flour and sweet foods in the diet contributes to an excessive increase in microorganisms and inevitably leads to caries and its complications. Take care of strengthening your enamel by taking vitamin complexes. Then the disease when “teeth crumble”, which occurs due to a lack of calcium in the body, will not be scary for you. - Brush your teeth 2 times a day.
Regular hygiene is one of the most effective ways to keep your teeth safe and sound. In addition to the traditional use of brushes and pastes, you should not neglect dental floss. Flosses effectively remove food debris between the teeth, preventing the development of many diseases. - Get preventive examinations once every six months.
It is easier to cure any disease if it is detected at the beginning of its development. Some dental diseases in dentistry have symptoms that cannot be identified on their own. For example, caries at the junction of teeth is visible only on an x-ray.
A person is not able to influence factors that cause various types of dental diseases, such as poor ecology, heredity, and stress. However, with a responsible attitude towards hygiene and prevention, the risk of dental diseases can be significantly reduced or, at least, their treatment can be facilitated.
Spreading
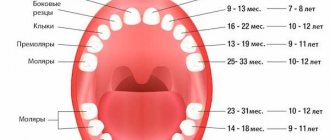
Normally, a person should have 20 baby teeth in childhood, which are replaced by 32 teeth, starting in adolescence. But for the reasons stated above, hypersets with two, four or more redundant teeth can be formed. 2% of people susceptible to this pathology is the total number. But among them it is possible to identify groups in which supernumerary teeth erupt in numbers of no more than two.
The location of such extra teeth (mainly incisors) is the upper jaw, with a shift of the supernumerary units towards the palate. Such people, of the total number of people susceptible to hyperdontia, are about 48%.
The second group is characterized by the growth of canines or premolars, also on the upper jaw. Incomplete teeth appear in them in the amount of one or two.
More than four, six, eight, etc. extra teeth grow only in a rare minority, with hypersets located in the lingual part of the oral cavity.
The remaining cases occur due to the unsystematic appearance of teeth in the lower jaw, on the side of the tongue, lips and cheek.
Supernumerary molar: review of a rare case
Supernumerary teeth or hyperdontia is a dental anomaly that is defined as the presence of a tooth or any dental tissue in excess of the set of 20 primary teeth and 32 permanent teeth. Supernumerary teeth can occur singly, in groups, unilaterally, bilaterally, they can erupt or be impacted on one or both jaws, both in the primary and permanent dentition. The frequency of occurrence in primary dentition varies from 0.1% to 3.8% and from 0.3% to 0.6%. In permanent dentition, the anomaly is more common in men than in women in a ratio of 2:1. However, this gender disproportion is not observed in the primary dentition. There is also evidence that the Asian population is more susceptible to the anomaly. Single supernumerary teeth occur in 76-86% of cases, double teeth in 12-23% and multiple teeth in less than 1%. Multiple hyperodontia rarely occurs in people without any other concomitant diseases and syndromes. Typically, this anomaly is part of systemic disorders such as cleft lip and palate, cleidocranial syndrome, Gardner syndrome, Fabry-Anderson syndrome, chondroectodermal dysplasia, Euler-Danlos syndrome, and tricho-rhinophalangeal syndrome.
Supernumerary teeth can be found in almost any area of the dental arch. Localization on the upper jaw is much more common than on the lower jaw, especially in the anterior region (80%). Somewhat less frequently, supernumerary teeth can be located in the distomolar zone, lower and upper premolars, in the area of the upper canines and lower incisors.
The crowns of abnormal teeth have a normal appearance or an atypical shape, and the roots are also fully or partially formed.
The position in the dental arch varies: mesiodens, paramolar, distomolar and parapremolar. Mesiodens is the most typical localization between the central incisors on the upper jaw, paramolar position is an additional molar, usually rudimentary, small in size and located on the buccal or palatal side in relation to one of the molars on the upper jaw. Most often found in the interdental space of the second and third molars on the buccal side; distomolar position is the fourth permanent molar; parapremolar localization is mainly found in the interdental space on the buccal side between the first and second premolars in the upper jaw. Variations in the morphological shape include different conical type, number of tubercles, and odontome. Supernumerary teeth may be small, conical with a normal root; teeth with multiple cusps are usually short, with a barrel-shaped crown and an invaginated rudimentary root. Another variant of a supernumerary tooth - an additional one - resembles one of the existing ones and is located behind it. Most supernumerary teeth in primary dentition are of the accessory type.
Odontomas are any tumors that develop from tooth tissue. Many authors are inclined to believe that odontomas are a hamartoma or malformation rather than a neoplasm. Compound and compound odontomas are two different types described. Complex odontomas are characterized by diffuse dentin tissue that is completely disorganized, while compound odontomas are malformations that have superficial anatomical similarities to a normal tooth.
According to their shape, supernumerary teeth are classified into additional (eumorphic) and vestigial (dysmorphic). If supernumerary teeth have normal morphology, they are classified as “additional”; if the morphology is abnormal, the teeth are classified as vestigial. The position of the supernumerary teeth can be between the central incisors, overlapping, and the orientation is described as vertical, inverted, or transversal.
This article presents a clinical case of the presence of an additional molar in a somatically healthy patient. A review of the literature regarding the incidence, classification, etiology, complications, diagnosis and treatment strategies of this pathology is also presented.
Description of a clinical case
A 22-year-old man came to the Department of Conservative Dentistry and Endodontics with complaints of pain in the posterior segment of the upper jaw on the left. Hereditary anamnesis and disease history are unremarkable; no signs of systemic diseases or syndromes have been identified.
Intraoral examination revealed Class I occlusion and no pathological tooth alignment. In addition to the full set of permanent teeth, one supernumerary tooth was found, located on the palatal side between the upper first and second molars on the left (Figure 1).
Figure 1: Intraoral photograph showing the paramolar position of the supernumerary tooth between the upper first and second molars on the left.
The supernumerary tooth is defined as a paramolar. The paramolar crown had two cusps and very much resembled the structure of a permanent premolar. The tooth is rotated axially, with the buccal surface distally and the mesial surface buccal. A carious lesion was found on the mesial side of the paramolar (Figure 2). Examination of the soft tissues revealed periodontal inflammation between the first and second molars and paramolars. X-rays were taken: panoramic, sighting and occlusal. Reading the panoramic image was difficult due to the palatal position of the tooth. On sighting and occlusal photographs, it was discovered that the supernumerary tooth was affected by caries and had one root (Photos 3 and 4).
Figure 3: Spot X-ray showing a paramolar with a fully formed tooth (indicated by arrow).
Figure 4: Occlusal radiograph of the maxilla showing the supernumerary tooth (arrow).
The patient was informed of the existing situation. It is recommended to remove the paramolar due to its inconvenient location for hygiene, possible food retention, recurrence of caries and damage to periodontal tissue. The patient was sent to the Department of Maxillofacial Surgery for paramolar removal.
The extracted tooth is cleaned, disinfected and analyzed. The morphology of the tooth is normal. The length of the root corresponds to the size of the crown. The root apex is fully developed. X-ray examination revealed type I canal configuration (Vertucci). Actual tooth dimensions: mesiodistal and bucco-palatal crown width 6 and 10 mm, respectively, crown length 6.5 mm, root length 12 mm. Morphometric measurements showed a high similarity of the supernumerary tooth with the premolar (Photo 2).
Photo 2: Photographs of the extracted tooth: (a) occlusal view, (b) mesial, (c) distal, (d) buccal, (e) palatal.
Discussion
The appearance of paramolars is a fairly rare occurrence. The etiology of this anomaly is not fully understood. Several theories have been proposed: phylogenetic, dichotomous, dental lamina hyperactivity theory, and a combination of genetic and environmental factors.
Phylogenetic theory refers to the process of atavism (evolutionary return). Atavism is a return to an earlier morphology or type. In past centuries, the third molar was almost always present in the permanent dentition; it was comparable in size to the second molar. Moreover, the fourth molar was also quite common. However, as a result of the evolution of phylogeny, the size of the dental arches gradually decreased, which led to a reduction in both the number and size of human teeth. This was one of the stages of preferential development of the cerebral skull over the facial skull. Thus, the appearance of additional paramolars can be considered an example of atavism, the genetic memory of the fourth molar in previous generations. It is worth saying that this theory was rejected by many authors.
The dichotomous theory explains the appearance of supernumerary teeth by splitting the tooth germ. The rudiment splits into two equal or unequal parts, from which morphologically normal independent teeth subsequently develop.
The lamina hyperactivity theory is the most accepted theory. She explains the appearance of paramolars as a result of local, independent, due to special stimulation, increased activity of the dental plate. According to the theory, lingual expansion of the accessory tooth bud leads to the development of a morphologically unchanged tooth, and the vestigial forms arise from the proliferation of epithelial lamina remnants, which is induced by the pressure of permanent teeth. Others are inclined to believe that hyperodontia is associated with multifactorial causes, which are still based on hyperactivity of the dental plate. Remnants of the dental lamina may remain in the jaws in the form of epithelial pearls or islands. When exposed to inducing factors, supernumerary teeth or odontomas can develop from additional rudiments. The best supported hypothesis is that the development of supernumerary teeth is associated with a complex of genetic and environmental factors. This is confirmed by the presence of similar anomalies in close relatives. However, despite the literature data, similar pathology was not found in the relatives of the described patient.
A careful analysis of the literature revealed very little information about the appearance of paramolars. Paramolars are somewhat less common in the upper jaw, very rarely bilaterally and almost never in the primary dentition. They are usually vestigial and located buccally between the second and third molars, although in some cases they can be located between the first and second molars. Fusion of paramolars with normal teeth is also incredibly rare. The literature describes the only case of endodontic treatment of a fused second left molar in the lower jaw and a paramolar with a split crown.
Diagnosis also requires differentiation of other structures that may appear in the molar area, such as an additional cusp or a fused supernumerary tooth. Bolk in 1916 first described an additional cusp on the buccal surface of the upper and lower permanent molars, which he called the paramolar cusp. Dahlberg in 1945 proposed the term paramolar cusp to refer to any abnormal cusp, supernumerary inclusion, or elevation on the buccal surface of both maxillary and mandibular premolars and molars. He presented a paleontological nomenclature in which he classified these structures as “protostylid” if they are on the lower jaw and “parastylid” if on the upper jaw. It is widely accepted today that such formations originate from the cervical region of the tooth and are variable in appearance. Often these structures appear on the buccal surface of the mesiobuccal tubercle and quite rarely on the distobuccal tubercle. It is believed that the paramolar tubercles may originate from the remains of their own epithelium or be a genetic remnant from mammals and lower primates.
Supernumerary teeth may erupt normally, remain impacted, or appear axially rotated or with other abnormalities. Supernumerary teeth with a normal position in the bone usually erupt. However, only 13-34% of supernumerary teeth in the permanent dentition erupt normally, compared to 73% in the primary dentition. The rest may remain impacted and cause complications.
The development of complications can cause a delay in the eruption of associated permanent teeth, retention, ectopic eruption, disposition, rotation of adjacent teeth, crowding due to insufficient space for eruption, malocclusion due to a decrease in space in the dental arch during the eruption of paramolars, tremors in the molar area, traumatic bite and ulceration of the buccal mucosa with buccal placement of paramolars, difficulties in orthodontic treatment, pathological development of the root of associated permanent teeth, formation of follicular cysts from the follicular sac of a supernumerary tooth, trigeminal neuralgia due to compression, pulp necrosis and root resorption due to excessive pressure of the paramolar , caries due to plaque accumulation, gum inflammation and localized periodontitis. As can be seen from the described case, due to plaque retention, carious lesions of the paramolar and inflammation of the surrounding periodontium occurred.
Most supernumerary teeth are impacted and are usually discovered incidentally during radiographic examination. However, if a patient presents with complications that are often associated with the presence of a supernumerary tooth, the dentist should consider this anomaly in the differential diagnosis and insist on appropriate x-ray examination.
The most valuable radiographic examination is the OPG with additional targeted photographs and photographs of the upper and lower jaw in the occlusal plane. To clearly localize an unerupted tooth, use the vertical or horizontal parallax technique. Parallax is a change in the view of an object against a specific background based on the movement of the viewer. This technique can be carried out by taking images of the same area, but from different angles, with two different devices. When using this method, as a rule, the reference point is the root of the adjacent tooth. In addition, cone beam CT may be used. This technology provides a three-dimensional image of the structures of the specified zone and is incredibly informative for the described anomaly.
Clinical management of patients with paramolars depends on the position of the tooth and its effect on surrounding tissues and important anatomical structures. Treatment offers two options: removal or observation. Observation does not include any manipulations other than clinical and radiological monitoring of the patient. This method is preferable if the presence of a paramolar is asymptomatic and does not cause any inconvenience. If any complications arise, tooth extraction is advisable. In the described case, we resorted to tooth extraction in order to maintain the proper level of hygiene, prevent the carious process and preserve the surrounding periodontium.
Conclusion
The dentist needs to know about the different types of supernumerary teeth for proper diagnosis and timely detection of this anomaly. Each such case requires careful diagnosis and subsequent appropriate treatment that causes minimal complications.
Authors: Gurudutt Nayak, Shashit Shetty, Inderpreet Singh, Deepti Pitalia Department of Conservative Dentistry and Endodontics, Kanti Devi Dental College and Hospital, Mathura, Uttar Pradesh, India
What does it look like
The main symptom or sign is the presence of extra teeth or even a hint of their appearance in the form of a painful swelling in the mouth. In such cases, the first thing they do is targeted radiography, which allows one to clearly diagnose problems in the area of 4-5 teeth.
If this method turns out to be ineffective, an orthopantogram is used, which reflects a more complete picture of the condition of the roots of the teeth and jaw bones. And to obtain a 3D picture of the condition of the roots and crowns, you can make a computer tomogram.
This anomaly can appear at any age. True, in adults and children the clinical picture of the development of the disease can manifest itself differently.
In children
Extra teeth can come out in the first few months of a child’s life, that is, in full accordance with the timing. But their number will be doubled. Although there have been cases of the appearance of such teeth immediately after the birth of the baby, in the first weeks and even days of its existence.
Both the baby and the mother suffer from such a “toothy” because:
- When teeth grab the nipple, wounds and cracks appear on it.
- In a child, the unpleasant sensations from teething intensify many times over.
- Poor milk flow due to improper latching of the breast.
- The child has difficulty sucking milk.
Manifestations of hyperdontia in an infant can be expressed in:
- Poor nasal breathing due to swelling of the nasal mucosa.
- Severe drooling.
- The gum tissue is swollen and painfully red.
- The temperature rises to low-grade levels, that is, up to 38⁰C, for several days.
If the case is advanced, then the symptoms change to the following signs:
- diction is impaired;
- an incorrect bite is formed;
- due to injury to the mucous membrane of the tongue and the inner surface of the cheek, wounds regularly form on them;
- there is no complete closure of the main dentition.
All this will be especially pronounced if extra teeth begin to grow in the area of the upper palate. Hyperdontia especially hinders children who have begun to develop speech. The first consequence of the appearance of extra teeth will be a lisp due to the fundamental impossibility of pronouncing sounds correctly. After all, teeth that have grown outside the dentition will not allow the tongue to take the correct position when trying to pronounce hissing, voiceless, and voiced consonants. No speech therapist can help solve this problem.
And the presence of extra teeth at primary school age (especially if they immediately catch the eye during a conversation) can serve as a subject of ridicule and even bullying from peers. Which is also fraught with deep psychological problems.
In adults
Abnormal dental development in adults may have the same symptoms as in children. But because the tissues of the oral cavity have already been formed and have essentially stopped in their growth and development, additional symptoms may include:
Dystopian teeth
That is, additional teeth whose growth has stopped and the bite has already been formed. And there is no longer room for the growth of other teeth.
- The growth of extra teeth occurs in the roof of the mouth or in the lingual (tongue-facing) part of the gum. Moreover, in the upper jaw - in the lower jaw, cases of germination of extra teeth are recorded much less frequently.
- The teeth have an incorrect turn, an atypical angle of inclination, and are curved.
- The teeth adjacent to the abnormal swelling become loose.
- In the area of tooth growth, protrusion of the jaw bone is observed.
- The gums often become inflamed, and X-ray examination at the initial stages of the anomaly reveals deformations of the jaw bones - even before the roots of extra teeth form.
In adults, dystopic teeth become a source of psychological problems. Such people are often withdrawn and unsociable. And psychological problems then turn into chronic forms of diseases of the digestive, nervous and endocrine systems.
Impacted teeth
This term refers to teeth that are unable to erupt and remain in the bone tissue of the jaw. A person often does not even suspect their presence until they make themselves felt with all sorts of complications. Namely:
- Loosening of normal, healthy-looking teeth.
- When an impacted tooth is located close to the edge of the jaw, a subcutaneous or axillary protrusion appears on the face.
- At any time of the day, aching pains can appear and just as suddenly disappear.
The most difficult moment is the appearance of supernumerary teeth in place of impacted third molars, or “wisdom teeth.” Which cannot germinate due to the presence of supernumeraries. Because third molars have a large area of chewing surfaces, such attempts to erupt lead to overstraining of the gum tissue and even entangling of the roots of other teeth during the growth process. The consequences of this can manifest themselves in the form of inflammation of the roots of all molars up to and including the premolar.
Consequences
Untimely or improper treatment of hyperdontia can cause serious consequences, the correction of which may take a long time:
- severe malocclusion;
- speech defects that cannot be corrected;
- constant injury to soft tissues leads to chronic inflammation with a high risk of developing benign and malignant neoplasms in the oral cavity;
- Impacted teeth are a common cause of chronic osteomyelitis of the jaw.
The lack of correction of hyperdontia in children is especially dangerous, since it often causes disturbances in the correct formation of jaw tissues. Supernumerary teeth can cause the death of the rudiments of permanent teeth or their improper eruption.
Therefore, if there are any signs indicating the appearance of excess dental elements, or if impacted teeth are detected, you must urgently seek advice from a dentist!
Types of hyperdontia
There are several of them. And they differ in the degree of inconvenience for their wearer and in the possible consequences. And even according to the subjective feelings of people who have been diagnosed with this disease.
Typical hyperdontia
This pathology is characterized by the presence of extra teeth that began to grow without leaving the dentition in the mouth. Since two normal-sized teeth would be cramped, such teeth, called twins, are reduced in size. This is expressed in the reduction of their coronal part.
The cause of this anomaly is most often heredity.
Atypical or atypical
This pathology with an increase in the number of teeth is characterized by the growth of extra teeth outside the dentition. Usually on the palate, where they can take up almost all the available space. Or the lateral surfaces of the jaw arches, most often from the side of the tongue. It is a very rare form of pathology.
Real (true)
Supernumerary permanent teeth in this type of hyperdontia appear from the formation of excess root buds or when the roots split in the initial stage of their growth. It does not cause significant inconvenience as long as both teeth in a pair of “twins” are healthy. Problems arise if at least one is affected by caries, the treatment of which can be difficult due to the intertwining of the roots of such teeth. For the same reason, there are difficulties with their removal.
False hyperdontia
Probably the most harmless of all, from the “it will go away on its own” series. Although, of course, medical supervision is mandatory in order to avoid developmental complications. It occurs when a child’s bite changes due to the replacement of milk teeth with permanent ones. It occurs when a permanent tooth erupts, when the milk tooth has not yet fallen out. Corrected after the loss or removal of a baby tooth. The decision to remove is made by the doctor.
The long-term coexistence of missing baby teeth and new, permanent ones is not such a rare phenomenon. This happens due to the inattention or even frivolity of parents who missed such an important stage in the development of the child. Especially if the growth of permanent teeth occurs painlessly.
What does the cost of treatment depend on?
The cost of treatment is determined by various factors, including the complexity of the anomaly and the method of its correction. If the patient does not show signs of deformation of the jaw arch, then simple removal will be required:
- extraction of one supernumerary element costs around 1,500 rubles,
- with its dystopia and retention, complex removal is required, and the cost of the procedure will vary from 3,500 to 15 thousand rubles.
The need for orthodontic correction significantly increases the cost of treatment. Here the price will depend on the specific technique, type of corrective structure, its materials and additional procedures.
Types of teeth with hyperdontia
Supernumerary teeth in hyperdontia can be divided into several types according to their location in the mouth:
- Spiny. May form on the upper jaw. Localization - between the central and lateral incisors, within the immediate limits of the main dental arches. They are called spiky because of the presence of very sharp ends.
- Additional premolars. They grow from the cheek side within the normal molar units of the dentition.
- Extra fangs. These grow on the upper jaw, in 99% of cases - on the side of the cheek and lip.
- Additional premolars. The localization area of these additional teeth is the lower jaw, on the cheek side.
Additional and primary teeth may fuse. There are 4 types of such merger:
- Bedding. The enamel of both teeth, twin neighbors, grows in the form of tubercles over the entire tooth surface.
- Root merge. The crown parts are located separately, but the roots are fused together.
- Coronal fusion. The root system of each tooth is separate, but the crown part is fused and has one common enamel “shirt”.
- Complete fusion of twin teeth. The crowns, which have a common enamel coating, and the roots are fused together.
Features of polyodontia in adults and adolescents
In adults, after complete replacement of complete teeth, the presence of additional units can lead to additional pathologies:
- chronic rhinitis, sinusitis when the wall of the maxillary sinuses is perforated by the roots of supernumerary impacted structures;
- interdental caries - due to teeth fitting too closely to each other.
Retention and dystopia
Adults are characterized by 2 main types of supernumerary teeth:
- Dystopic teeth are the name given to teeth with deviations in the direction of growth. The peculiarities of the formation of supernumerary units very often lead to dystopia. This is due to the fact that the space on the dental arch line is limited, and the roots of normal teeth simply push the “intruder” towards the cheek or palate.
- Impacted teeth – impaction occurs when a tooth loses its growth impulse and remains embedded in the jawbone. Impacted teeth can cause the adjacent normal teeth to become loose and cause them to shift and change the bite. Often cause pain.
On a note! According to statistics, hyperdontia accounts for up to 2% of cases of dental problems. Of these, 70% are associated with the appearance of single supernumerary teeth, 25% with a couple of such formations, and only in 5% complex multiple complexes of 3–4 or more teeth can be found.
Treatment of hyperdontia
It happens that there is no need to treat such an anomaly at all: if the teeth do not extend beyond the dentition, do not disturb their shape and do not injure the mucous membrane. In other cases, the presence of supernumerary teeth in the mouth requires serious intervention. Usually a dental surgeon.
It can not only remove unnecessary teeth that clearly interfere with normal life, but also help the necessary teeth to emerge. And the orthodontist will help correct the bite.
Extra teeth must be removed if:
- Milk teeth do not allow permanent teeth to erupt normally, and a growing person retains a “milk bite.”
- In the dental arch, the teeth are positioned incorrectly, grown with displacement and a strong inclination. This phenomenon is called dystopia.
- The crown is stuck in the gum or bone and cannot erupt. This is called retention.
Such pathological cases in dentistry can be treated without difficulty. If, of course, the patient turned to the appropriate doctor on time. Although there are nuances associated with each specific person.
The question of removing extra teeth is decided by the doctor based on: the stage of formation of the dental system, the inclination of the supernumerary tooth, what consequences and defects are predicted from a particular situation.
Sometimes, if supernumerary teeth:
- interfere with normal eruption;
- contribute to the formation of three – abnormal gaps between the teeth, causing caries in the gum pockets, and diastema – an extra-wide interdental space;
- impacted ones are not capable of eruption due to the fact that they are incorrectly formed and strongly inclined;
- may cause bite defects.
What to do?
The presence of supernumerary teeth is an abnormal phenomenon, so the issue of eliminating this problem must be resolved. How, this is another question, to give an unambiguous answer to which is impossible. As a rule, there can be several ways to solve a problem. The choice of treatment method depends on where the extra tooth is located, what shape it is, and what stage of eruption it is at.
Facilitating teething in baby
Drug treatment allows you to relieve unpleasant and painful symptoms during the eruption of excess buds. This option is the only one for children with baby teeth if the tooth is only at the eruption stage. When it finally germinates, it will be necessary to use more radical methods. The dentist prescribes medications that will help relieve pain, reduce fever and stop the inflammatory process in the soft tissues of the gums.
Simple tooth extraction
Surgery. This method is the fastest and most effective, since removing an extra tooth easily solves the problem and relieves a person from unpleasant sensations and discomfort. This treatment method is used when there is too little space in the dentition for an extra tooth or there is no space at all. Most often, supernumerary teeth are removed when there is crowding of the teeth. To free up some space in the dentition, the wisdom teeth are removed first, and if this was not enough, the premolars are also removed.
Braces and other orthodontic treatment methods
Orthodontic treatment is a method that involves correcting the bite, straightening the teeth, etc. The result is achieved by installing braces or other orthodontic structures that allow you to straighten crooked teeth and return them to their place, where they should be. The duration of wearing braces depends on many factors:
- the age of the patient (children have their own specifics);
- complexity of the situation;
- locations of supernumerary teeth and others.
At the first and second stages of the disease, the doctor may decide to install special expansion plates or aligners. Can also apply the separation method.
Consequences of poor quality treatment
If the treatment is not well-carried out, impacted teeth will continue to interfere with the normal development of the bite and dentition, which causes a violation of chewing ability, leading to a number of problems with the gastrointestinal tract, and impaired diction, which negatively affects pronunciation and pronunciation. Also, after unsuccessful treatment, healthy teeth that are located next to the additional one may begin to deteriorate.
Preventive measures
The essence of preventing dental anomalies is to eliminate the possible causes of their appearance even at the stage of formation of rudiments, that is, all responsibility for possible dental anomalies depends entirely on the child’s mother.
To prevent this unpleasant phenomenon, you need to eat right, food should be balanced and healthy. It is important to give up bad habits and follow your doctor’s recommendations. When the baby is small, you need to make sure that he does not suck his finger or pacifier for more than a year and regularly take him for examinations to the dentist for timely detection and elimination of dental problems. Moscow metro station Zvezdnaya, Danube Avenue, 23
When to expect supernumerary teeth to appear?
Always. And not just during and immediately after the baby teeth period. This is especially true in cases of hereditary occurrence of such an anomaly. The most common growth zones for supernumerary teeth are the upper incisors, canines, premolars and first molars. It is possible that such teeth will appear not only within the dentition, but also in the area of the upper palate. But the same supernumerary teeth, but within the lower jaw, are found 5-6 times less often.
Sometimes a deep location in the thickness of the jaw can cause extensive trauma if the tooth is “not going” to leave the place of its growth point due to the obstruction of surrounding tissues. Then the surgical intervention is postponed (if not canceled altogether), and orthodontic devices are placed on the dentition.
Diagnostic methods
The main indication for diagnosis is the presence of an “extra” tooth in the patient’s oral cavity or obvious signs of its eruption (painful tubercle or swelling in the gum or palate). All of these signs can be identified through a routine visual examination, during which the dentist evaluates the condition of the oral cavity. To confirm the diagnosis and carry out differential diagnosis, an X-ray examination is performed - an orthopantomogram. If it is necessary to examine the dentition in several planes, computed tomography (CT) is additionally prescribed.
On a note! The patient may not be aware of the presence of impacted supernumerary teeth. In this case, hyperdontia is detected only by the results of an X-ray or CT scan of the maxillofacial region.
Symptoms
Polyodontia in humans is expressed in the form of a supernumber of teeth, which may differ in size and shape, but is usually visually quite easy to detect. In addition, supernumerary teeth can cause:
- speech defects such as lisp, paralalia and dyslalia ;
- pain and difficulty chewing;
- diastemas and trema;
- loose teeth;
- violations of occlusion and bite, for example, towards open or deep;
- injuries to the lips, tongue and other parts of the oral mucosa;
- the development of follicular cysts, which, with a decrease in immunity , can worsen and lead to the formation of fistula tracts and swelling of the surrounding soft tissues;
- inflammatory changes, as well as sinusitis , rhinitis , osteomyelitis , etc.;
- degenerative processes in the oral cavity, for example, resorption and osteolysis of roots;
- lack of space for development and crowding of permanent complete teeth, changing their inclination, location and deforming the dental arch.
Important! Extra teeth can interfere with good oral hygiene, therefore increasing the risk of caries , as well as its complications - pulpitis and periodontitis .