Tooth extraction is always accompanied by bleeding, but it usually stops on its own after some time. However, in some cases this does not happen and measures must be taken to forcibly stop the bleeding. There are many methods to stop bleeding - for example, a hemostatic sponge has proven itself well after tooth extraction. Using this product is a simple procedure, but all indications/contraindications must be taken into account.
Hemostatic sponge after tooth extraction
Features of wound healing after tooth extraction
Before moving directly to hemostatic sponges, what they consist of and how to use them, you need to understand how the wound heals after removal and what can go wrong here. More on this later.
Why is there bleeding after removal?
Bleeding is a natural reaction to surgery. After all, when a tooth is removed, the smallest capillaries that penetrate the gums and ligamentous apparatus - the periodontium, which attaches the roots to the bone socket - are torn. And with difficult removal, the bleeding may be even stronger, because... The dentist makes incisions in the gums and drills into the jaw bone - the tissue is more damaged.
Bleeding is a natural reaction to surgery
Read on the topic: How long can a tooth hurt after extraction - normal and pathological.
How long does bleeding last normally?
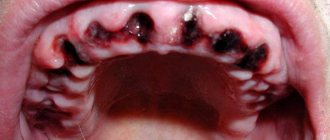
Normally, the blood stops within 15-20 minutes (less often, within 45 minutes) and a blood clot forms in the socket. It seals the hole like a cork, preventing germs from penetrating inside. If the patient has problems that affect blood clotting, then the bleeding time is prolonged, and a clot may not form at all. And this is already fraught with inflammation of the bone socket (the pathology is called “alveolitis”). Therefore, according to indications, the dentist applies a hemostatic drug to the area of the extracted tooth.
On a note! Bleeding may appear again for a short time (and there will be quite a bit of blood) after the anesthetic wears off - if it contained adrenaline. This substance narrows the blood vessels in the intervention area, and as they expand normally, slight bleeding occurs. It goes away quickly.
Why does the bleeding not stop for a long time?
As a rule, after tooth extraction, the dentist says that you should not eat or drink for 2 hours. But few people say that you should not rinse your mouth or suck drinks out of a straw. In the first days, only oral baths are allowed, and it is better to drink in the usual way. Also, do not touch the wound with a brush. It is better to chew food on the healthy “side” of the jaw. Otherwise, there is a risk of moving or “pulling” the clot out of the hole - which will provoke new bleeding or even inflammation, which will result in long-term treatment.
The following groups of patients are also at risk:
- who has not formed a blood clot,
- with blood diseases,
- who takes blood clotting medications,
- having high blood pressure,
- women during menstruation or menopause,
- exposing themselves to physical activity immediately after removal and during the recovery process,
- if there was already inflammation at the extraction site (for example, pericoronitis above a wisdom tooth),
- during complex operations: when several teeth were removed at the same time, or manipulations were performed with increased tissue trauma.
Bleeding may occur during physical exertion after removal.
When you need urgent help
If the bleeding is profuse and does not stop for a long time, if after normalization of the condition the blood begins to ooze heavily again, this is a reason to consult a dentist. In a situation where the patient, in the presence of continuous bleeding, feels weakness, apathy, if the temperature has risen sharply (above 39 degrees Celsius), it is better to call an ambulance or go to the hospital on your own.
What is a hemostatic sponge
Now let's move on to why a hemostatic sponge is placed in the hole left after tooth extraction? Let's first understand the terminology. “Hemo” means “blood” and “stasis” means stopping. Those. a hemostatic sponge is needed to stop bleeding. In simple terms, this is a kind of replacement for a blood clot. The hemostatic sponge in the tooth socket not only seals the open cavity, but also has a hemostatic effect. Firstly, it puts pressure on small vessels, stopping bleeding. Secondly, it absorbs excess blood, increasing several times. The bleeding stops within 2-3 minutes.
On a note! By the way, local hemostatic agents are used not only in dentistry, but also in other areas of medicine - for example, hemostatic bandages successfully replace tourniquets that are applied for bleeding.
Recommendations
The collagen sponge should be removed from the packaging immediately before use. It is important to follow the rules of asepsis to prevent accidental infection in the wound. The hemostatic agent is carefully applied to the bleeding area and held for a couple of minutes. Deep wounds are tightly packed and then bandaged.
After the collagen sponge is saturated with blood, it will slightly increase in size. This will ensure that it adheres tightly to the damaged bleeding area. In cases where it is necessary to close damaged areas of parenchymal organs, a sponge of a suitable size is placed in the existing cavities. To stop bleeding, it is allowed to form several layers from it. After this, it is fixed using a U-shaped seam.
You can now buy a collagen hemostatic tube in pharmacies at an affordable price. It is presented by manufacturers in a wide range. You can also pick up the product in specialized online stores. Now you can use the booking service or order delivery of the product to the specified address.
Before using a collagen-based hemostatic sponge, you should carefully read the manufacturer's instructions. The product should be stored in a dry place where the temperature is maintained in the range of 10°C - 30°C. With high humidity, the sponge quickly becomes unusable. The shelf life of the product, subject to the required conditions, is 5 years.
Appearance and release form
The hemostatic sponge looks like a cube or plate, which looks like a small sponge or a piece of yellow or white foam rubber. Although in fact it consists mainly of natural collagen with various medicinal additives. The plate is quite soft and easy to cut, which allows the dentist to cut the desired size according to the shape of the hole.
The plate is quite soft and easy to cut
Manufacturers produce both small (1x1 centimeter) and large sponges (10x10 cm). The plates are tightly sealed in transparent bags, and the cubes are sealed in dark, opaque bottles. Hemostatic powders and gels are also produced. Absolutely all collagen hemostatics dissolve on their own in the wound over time.
Types of hemostatic sponges
According to the manufacturing method, hemostatic sponges for teeth are of the following types:
- from donor blood plasma - amben,
- from bones/tendons/blood of cattle - collagen and gelatin.
You need to understand that a hemostatic agent not only stops bleeding (due to aminocaproic acid, for example) and stimulates the formation of a blood clot, but also has an antiseptic effect. It can also accelerate regeneration and relieve inflammation. It all depends on the active components that make up the hemostatic sponge. The drug can be impregnated with the following substances:
- antiseptics: chlorhexidine, furatsilin, silver suspension, boric acid, iodoform,
- local anesthetics: for example, lidocaine,
- preparations for bone regeneration: calcium phosphate,
- antibiotics: metronidazole, chloramphenicol, neomycin, gentamicin, etc.,
- natural substances: propolis, eugenol, etc.
Hemostatic sponges for teeth come in different types
Experience in using collagen dressings and Meturacol sponges in surgical practice
The prevalence of trophic ulcers of venous etiology is about 70% of all ulcers of the lower extremities. Trophic ulcers occur in 1–2% of the adult population. Diabetic micro-, macroangiopathy and distal neuropathy cause trophic ulcers in 3% of patients with diabetes mellitus (DM). The number of patients with foot ulcers reaches 15%. Every year, 0.6–0.8% of patients with diabetes undergo lower limb amputation at various levels. Moreover, in 85% of cases, amputations are preceded by ulcers [6, 10]. It is known that the course of the wound process is more complex and varied against the background of diabetes. Diabetic foot syndrome (DFS) is one of the most important problems in modern diabetology. Approximately 40–70% of all non-traumatic amputations are performed in patients with diabetes. During the first 5 years after amputation, up to 80% of patients who have undergone high amputation, i.e. amputation above the knee, die. The risk of developing DDS in patients with diabetes with more than 20 years of disease experience increases to 75%. Gangrenous lesions of the foot in 30–50% of cases result in amputation of the limb. As practice shows, patients with foot ulcers due to DFS are treated in hospital for 6–8 weeks. The average duration of further outpatient treatment for these patients is 4 months, and in 10% of patients it lasts more than 1 year. This is due to the fact that the course of the wound process in patients with diabetes has its own characteristics: a lower rate of epithelization, a tendency to generalize the infectious process, a negative effect on the reparative processes of chronic renal failure [5, 11, 13].
The pathophysiology of chronic wounds is complex and varied, but they all share common features: long-term inflammation that causes extensive tissue damage and impedes healing, and excessive scar tissue formation due to fibroproliferative disorders. The criterion for determining a chronic wound is the period of its existence, which, without signs of active healing, according to various sources, varies from 4 to 8 weeks. [1, 3, 17, 22]. As a result of unrecognized persistent infection or inadequate surgical debridement, acute wounds can develop into chronic wounds at any time. However, in the vast majority of cases, chronic wounds represent the last stage of advanced tissue destruction caused by vascular diseases of a venous, arterial or metabolic nature, or radiation injuries [20, 23].
At the end of the last century, 10 thousand methods of treating trophic ulcers were known [9]. Along with general treatment methods, there are chemical, physical, biological agents and methods of treatment. But, as a rule, these methods do not give the expected effect; many of them require long-term hospital treatment, and some require subsequent surgery to close the ulcer. Although even after the healing of a trophic ulcer has been achieved, the frequency of relapses is often, according to various sources, ranging from 7.3 to 56.2% [24]. Also N.I. Pirogov identified 3 stages of the wound process. Today, the staged approach to wound healing proposed by M.I. is most often used. Kuzin. Traditionally, the main element of local wound treatment is a dressing, which isolates the wound surface from harmful environmental influences and maintains an optimal condition for healing in the wound.
The discovery of antibiotics marked the beginning of a new era in the treatment of purulent diseases. These drugs have cured millions of people. However, in modern conditions, in many cases antibiotics are ineffective due to the increasing resistance of microorganisms to them [12]. In 1962, G. Winter published an article with observations about the preservation of a moist environment in a wound in animals, which, in his opinion, accelerated the epithelization of acute ulcers that did not penetrate the entire depth of the skin by 1.5 times [28]. Subsequently, the theory of wet wound healing was supported by a number of experiments, including on humans. At the end of the twentieth century. The theory of the “ideal dressing” arose, which did not take into account the peculiarities of the course of the wound process. In addition to the principle of moist healing, the management of chronic ulcers must comply with the conditions of thermal insulation, prevent the accumulation of excess exudate, and provide for regular debridement (surgical treatment).
Currently, staged treatment of venous trophic ulcers is generally accepted. In accordance with this concept, it is initially necessary to achieve closure or reduction in the area of the ulcerative defect, improve the condition of the surrounding tissues, and reduce pain and swelling syndromes. The use in practical medicine of scientific data concerning the pathogenesis of wound healing of chronic wounds obtained in recent years allows us to hope for improved treatment outcomes for patients with long-term non-healing wounds.
Modern dressings should keep the wound in a moderately moist state and protect it from trauma, but it must be remembered that excessive moisture causes the death of epithelial cells; when the wound dries, a crust forms, slowing down epithelization; the use of fat-based dressings can lead to the so-called greenhouse effect, when purulent discharge accumulates under the bandage, increasing the absorption of toxic products and the severity of intoxication. The goal of local exposure should be to restore the physiological mechanisms of the wound process, ensuring the delimitation of necrosis, cleansing of the wound surface, and activation of repair processes in the wound. In this case, local treatment does not determine the outcome of the ulcer, but can influence the duration of healing.
Currently, dressings are being developed and improved, not only new drugs, but also entire groups of them are appearing, which allows us to expand our capabilities for treating wounds. At this stage, medicine knows more than 2.5 thousand types of dressings, despite the fact that most of them repeat each other to one degree or another.
In recent years, the so-called method of active therapy for chronic wounds has been formulated, which included the topical application of growth factors and biosynthetic skin analogues. The use of fast-growing epidermal cell grafts can save the lives of many burn patients by providing early and permanent closure of the excised wound. There is also a revision of many ideas about methods of treatment and care of wounds and previously used classifications of local treatments for wounds of various etiologies. Effective and at the same time gentle wound care, maintaining the natural wound healing process, together with a caring attitude towards the patient, are recognized as the basic principles of wound treatment.
These requirements are met by a biosynthesized material – collagen. For more than half a century, this protein has been the subject of close attention of scientists in various specialties (biochemists, morphologists, physiologists and clinicians), which is explained by its important role in ensuring vital processes and pathology of connective tissue. In addition, purified collagen from cattle skin is used as an adjunct to hemostasis during vascular, abdominal and dental surgeries. Collagen fiber consists of groups of fibrils, which in turn consist of even thinner microfibrils, twisted into a triple helix. Such fibers have high tensile strength. Over time, collagen undergoes the aging process in the body, which is due to the formation of cross-links between its fibers. Cross-links are stable, prevent the natural breakdown of collagen fibers, reduce their flexibility, firmness and elasticity.
The technological aspect of studying collagen is of great practical importance. With the help of synthetic materials, it was not possible to solve the complex problems of reconstructive surgery: even relatively inert polymers, remaining a permanent foreign body in the body, maintained a chronic inflammatory reaction and changed their physical properties. Long-term functioning of synthetic prostheses was often impossible.
The most promising material for the manufacture of prostheses, which, acting as a temporary guiding frame for regeneration, would gradually be replaced by the body’s own tissues, is the biopolymer collagen, which has the positive qualities of synthetic polymers and tissue grafts, but is devoid of a number of their disadvantages [8, 16].
The main advantages of collagen as a new plastic material are the absence of toxic and carcinogenic properties, weak antigenicity, high mechanical strength and resistance to tissue enzymes, adjustable rate of lysis in the body, the ability to form complexes with biologically active substances (heparin, chondroitin sulfate, antibiotics, etc.) , stimulation of the regeneration of the body’s own tissues. Collagen belongs to a class of proteins called scleroproteins. A feature of proteins of this class is their phylogenetic relationship in different animal species and humans. The share of collagen in the total mass of body proteins is about 30% (6% of body weight), and it makes up the bulk of the dermis (up to 70% in terms of dry weight).
The term "collagen" is a collective term. It refers to both specific monomeric protein molecules and aggregates of these molecules that form fibrillar structures in the extracellular matrix of connective tissue. Most often, collagen is used in the production of films, sponges, and fibrous materials [19].
Collagen coatings create optimal conditions for wound healing, due to which the inflammation process occurs within physiologically acceptable limits, wound healing time is reduced, which is confirmed by the successful use of collagen for the treatment of burns and wounds. Collagen is able to reduce the activity of proteolytic enzymes (in particular, matrix metalloproteinases) in the wound, thereby stimulating the formation of granulation tissue. Modern collagen coatings are used in the form of sponges for the treatment of chronic wounds at the stage of exudation, granulation and epithelization in patients with purulent-necrotic lesions of the lower extremities, including in patients with DFS. Collagen dressings allow you to treat wounds of varying depths and degrees of complexity, as well as long-term non-healing wounds.
Collagen, thanks to the preserved fiber structure, not only stimulates the body’s natural healing process, but also promotes the rapid and effective growth of new full-fledged tissue at the site of the defect, acts as a matrix for the growth of new tissue: fibroblasts, blood and lymph vessels, nerve fibers from surrounding healthy tissue , introducing themselves into the collagen matrix, they spread strictly along it.
There are no contraindications to the use of these dressings. It should be noted that one more positive property is that collagen bandages do not stain linen, which creates certain convenience for patients and staff.
There are several foreign and domestic collagen dressings on the Russian market, but products from foreign manufacturers are highly expensive, so domestic developments are more accessible. One of the most famous and long-used collagen dressings is the Meturacol sponge. It was developed by scientists from the I.M. MMA. Sechenov in the 1980s. and its properties are not inferior to foreign analogues. Clinical trials of Meturacol were carried out at the Children's City Clinical Hospital No. 9 in Moscow (for the treatment of burn injuries in children injured in the disaster in Bashkiria in 1989), the Moscow Medical Dental Institute. M.A. Semashko (in the practice of treating purulent wounds), clinics of the Medical Center of the Administration of the President of the Russian Federation. This is a combination drug consisting of collagen from bovine split (a product obtained from the skin) of cattle, and methyluracil; It is a finely porous dry plate of white color with a slight specific odor. The drug has a porous structure with capillary activity, which promotes the constant absorption of wound secretions and necrotic cells, bacteria and fibrinous plaque, and accelerated formation of granulation tissue. Methyluracil, along with weakening exudative and alternative manifestations of the inflammatory process, accelerates tissue regeneration, healing of wounds and burns.
At the surgical department of the Doctor 2000 Medical Center, the experience of treating trophic ulcers using the Meturacol collagen sponge was analyzed. The planned tasks were:
- understand whether a constant moist environment is provided in the wound;
- ensure prevention of secondary infection;
- evaluate the possibility of rarely changing dressings (on average once every 3–6 days) and the painlessness of dressings;
- determine the timing of healing and rehabilitation of patients with chronic wounds.
The study included 32 patients of the surgical department of the Doctor 2000 Medical Center with chronic wounds of various etiologies: 17 men (53%) and 15 women (47%). Of these, 17 patients had VDS (53%), 11 had chronic venous insufficiency (CVI) (34%), 2 had erysipelas (7%), 1 patient had Martorell’s ulcer, 1 had a trophic ulcer due to chronic arterial insufficiency (Fig. 1).
The age of 21 patients (65.5%) ranged from 38 to 69 years, 11 patients (34%) were older than 69 years. The duration of existence of ulcers is from 3 months. up to 1.5 years. At the time of inclusion in the study, all patients had wound surfaces of a pale pink color, 8 had fibrin deposits and moderate serous-purulent discharge, 14 had areas of light brown, moist or partially rejected scab. All patients had perifocal inflammation of surrounding healthy tissues. There was no epithelialization.
Clinical assessment of treatment results when using the Meturacol collagen sponge was carried out on the basis of visual control of the course of the wound process, the amount and nature of discharge, and the timing of epithelization. The rate of ulcer closure was determined by calculating its area and depth in millimeters once every 10 days for 7 weeks. The study included wounds with an area of more than 30 mm2. The area of the wound and its changes during treatment were assessed quantitatively using transparent film at the beginning and after 3 weeks. treatment and at the end of the study. Clinical and laboratory studies were carried out before, during and after the course of treatment, which included de-escalation antibacterial therapy (1-2 drugs), taking into account the determination of the sensitivity of the microflora during a microbiological study of culture from the wound.
After treating the skin and cleaning the wound, the Meturacol collagen sponge was cut to the size of the wound and applied to it. It should have covered the entire surface of the wound defect (Fig. 2).
The collagen sponge Meturacol had a prolonged healing effect on the wound; a moist environment was created by the final application of the Krupoderm dressing. The collagen plate turned into a gel, the remnants of which were removed with a sodium chloride solution during subsequent dressings, which was painless for the patient. On wounds with little or no exudation, a Meturacol sponge was applied, after moistening it with a 0.9% sodium chloride solution.
Dressing was done once every 2–3 days, and if the wound was stable, the Meturacol sponge remained on the surface of the wound for up to 7 days. Against the background of antibacterial therapy and the use of Meturacol, in no case was there an increase in wound discharge under the dressing; by the second dressing, the phenomena of perifocal inflammation were stopped, and the amount of discharge decreased. With significantly exuding wounds in 4 patients (12%), dressings were changed daily until the wound discharge decreased; in other cases, due to the lack of discharge, dressings were performed once every 2–7 days. The period of epithelization was 21–57 days after the start of treatment. In 18 patients (56%), the wounds healed under a thin crust of exfoliated epidermis. In 3 cases (patients with CVI) (9.4%), the formation of a dry thin scab was noted under the dried bandage. In the remaining 11 (34%) patients, marginal epithelization was observed, the rejected fibrin layer and areas of thin wet scab were easily and painlessly removed during staged dressings. At subsequent dressings, melting and peeling of the remaining areas of the scab were noted.
In the 32 patients in this study and in other patients who received a total of approximately 700 Meturacol collagen sponges, no cases of allergic manifestations or intolerance were recorded. The results of observation of clinical cases during the study suggest the safety of the impact on bacterial contamination of wounds in the 2nd and 3rd phases of the wound process when using the Meturacol collagen sponge.
conclusions
The study showed the possibility of using Meturacol collagen dressings in the 2nd and 3rd phases of the wound process, the absence of allergic reactions.
It can be stated that Meturacol collagen sponges:
- simple and easy to use by both doctors and patients;
- provide a constant moist environment in the wound;
- economically profitable (3 times cheaper than imported analogues, do not require frequent changes);
- the painlessness of changing dressings, the absence of side effects, and the effectiveness of use are noted;
- in some cases, the healing time of ulcerative defects is reduced.
In conclusion, we give an example of treatment of patient B., 76 years old, with Meturacol collagen sponges. Diagnosis: type 2 diabetes, insulin-requiring, DFS, trophic ulcer of the left foot (Fig. 3–5).
Manufacturers of hemostatic sponges
Popular manufacturers of hemostatic agents used by dentists in our country are domestic companies. Let's consider them further:
- Alvostaz compress from Omega-Dent: available in the form of cubes, flagella, powders and solutions. The compresses are numbered - “1” with iodoform, “2” with metronidazole and chlorhexidine, “3” with neomycin and chloramphenicol,
- "Gemasept" with gentamicin from the Russian Research Institute of Hematology and Transfusiology of the Federal Medical and Biological Agency",
- “Collagen hemostatic sponge” with silver and boric acid from “Zelenaya Dubrava”,
- “Hemostatic sponge” with furatsilin and boric acid from “Belkozin”.
Biological dressing Digestol
Biological dressing "Digestol" - Self-absorbing collagen wound coverings with a cleansing and antibacterial effect, are highly porous white or cream-colored plates with a specific odor, made from a mixture of natural collagen biopolymer and trypsin-like enzymes digestase and collagenase (from the hepatopancreas of the Kamchatka crab). Ingredients: collagen at least 80%, digestase enzyme (collagenase) at least 1%, purified water Area of application: Complex treatment of purulent wounds, trophic ulcers, treatment of infectious and inflammatory diseases of the oral cavity, complications of diabetic foot syndrome. It has a rapid hemostatic effect by stimulating platelet aggregation and an antimicrobial effect by destroying the walls of bacteria. For the complex treatment of purulent wounds, burns, trophic ulcers, bedsores, gunshot wounds, treatment of infectious and inflammatory diseases of the oral cavity, complications of the “diabetic foot” syndrome in surgery, tamponing of sockets in dentistry. Has a cleansing and antibacterial effect. It has a rapid hemostatic effect by stimulating platelet aggregation and an antimicrobial effect by destroying the walls of bacteria. Dimensions 100x100x5 No. 1, 50x50x5 No. 1, 10x10x5 No. 10. pH of the aqueous extract: 5.0-7.5 Sterile, single use Sterilization: radiation Guaranteed shelf life of the plates from the date of sterilization: 3 years. Manufacturer: ZAO “Zelenaya Dubrava” , Russia Price: on request
Indications for use
A hemostatic sponge can be useful after tooth extraction, especially wisdom teeth. Because the “eights” often do not erupt completely, and the dentist has to perform a mini-operation to get to them and remove them along with the roots. When a tooth is removed, a hemostatic agent is placed 3-4 months before implantation to completely eliminate the possibility of complications and problems with the formation of new bone in the socket.
Also, hemostatic sponges or powders are used during operations on the gums1 - plastic surgery, curettage of gum pockets (removal of deep “deposits” of tartar), and when cutting off dead areas of the jaw bone due to osteomyelitis. In the latter case, bone blocks and materials for regeneration of bone substance are additionally planted. In general, the doctor always assesses the patient’s condition in advance - asks about diseases and other conditions, and about the medications taken. If there is a risk of bleeding or poor regeneration, then rest assured, a hemostatic sponge will definitely be placed in the hole.
These sponges are used for bone augmentation
It is important to know! A few days after tooth extraction, it may be necessary to apply a hemostatic sponge if the dentist sees a tendency to worsen. For example, a clot has fallen out or the gums/bone have become inflamed.
How to use the drug correctly
How to use the sponge? The hemostatic sponge is placed into the socket of the extracted tooth only by the dentist. Home use is not recommended due to the risk of infection deep into the tissues. The application procedure is given step by step below:
- tooth extraction or treatment of the hole a few days after removal: in the latter case, purulent masses are removed, irrigation is carried out with an antiseptic,
- a piece of the hemostatic plate is cut off with sterile scissors or a hemostatic cube is taken with tweezers,
- the drug is placed in the hole and pressed with a flat instrument: if the hemostatic agent is pre-saturated with thrombin, the hemostatic effect is enhanced,
- if necessary, an additional piece of hemostatic is applied,
- if necessary, a small tampon is placed on top of the hole (it will be removed the next day),
- suturing the gums - a seam in the shape of the letter “P”: also, if necessary, in most cases you can do without stitches.
A piece of the hemostatic plate is cut with sterile scissors.
Analogs
Some patients believe that a hemostatic sponge is not able to stop bleeding and alleviate the patient’s plight. In reality, the effect of this medication is selective, and it is also important to consider the risk of side effects. In such clinical pictures, the attending physician introduces a replacement and suggests using an analogue of the specified pharmacological group. Here is a replacement worthy of modern pharmacology, which can also be purchased over the counter, but after consulting with your doctor first:
- Kaprofer;
- Alginatol;
- Natalsid;
- Eavisel;
- Polyhemostat;
- Tissucol Keith;
- Posterisan;
- Feracryl;
- Tachocomb;
- Styptic pencil;
- Tissucol.
Is it necessary to remove the hemostatic agent?
Patients often wonder what to do with a hemostatic sponge after it has been placed in the socket of an extracted tooth? How long should I keep it on, and will it dissolve on its own? The rules of conduct are as follows: carefully but thoroughly observe oral hygiene, and also take medications prescribed by the dentist. There is no need to specially remove the hemostatic agent - after all, it consists of components that will completely dissolve during wound healing. And instead of a hemostatic agent, its own tissues form in the hole.
“When my wisdom tooth was removed, they stuffed it into the wound like a piece of foam rubber. I then saw the houses through the seams. I was also surprised - what is it? And at the next appointment, my dentist told me that this is a special sponge that absorbs blood and protects against infection. And when it resolved, I didn’t even notice)) It probably completely disappeared in a couple of weeks.”
Ekaterina R., review from irecommend.com
Contraindications and side effects
The only contraindication to the use of a hemostatic sponge after tooth extraction is an individual allergy to any of the components of the drug. In particular, for antibiotics that are used to impregnate the hemostatic agent. Therefore, be sure to tell your dentist if you are allergic and to what medications. Hemostatic agents should also be used with extreme caution in children.
There are no side effects, because There are no toxic substances or components that affect perception in hemostatics. But if itching, inflammation, or swelling appears, feel free to contact your dentist. These manifestations can be caused either by a newly manifested allergy or by incipient complications - if, for example, the treatment was carried out poorly or the patient did not follow the doctor’s instructions.
1Skulean A. Periodontal regeneration, 2012.
Precautionary measures
Absorbable GG is not used for heavy bleeding resulting from damage to large vessels. A contraindication to the use of a sponge is the patient’s individual intolerance to certain components of the product (for example, Furacilin). When used independently, it is not allowed to place (remove) GG into the inner layers of the socket; only surface application is permissible. When the hemostatic effect is achieved, the sponge is carefully removed from the postoperative wound.