Diseases of the gastrointestinal tract have a complex effect on the health of the entire digestive system, which includes the oral cavity. First of all, this effect is due to a lack of vitamins and minerals, which leads to inflammatory processes, and in addition, aggravates existing oral diseases.
Of course, in such cases, treatment of the problem should be comprehensive - you should also contact a dentist
, who will eliminate the manifestations of diseases in the mouth, and to an endocrinologist, who will directly eliminate the root of the disease.
Let's look at the main examples of gastrointestinal diseases that directly affect the condition of the oral cavity and teeth.
Stomach ulcer, its types and stages
Gastric ulcer (hereinafter referred to as PUD) is a disease in which a mucosal defect occurs and the submucosal layer may be affected. This is a chronic disease that occurs in waves, with periods of exacerbation and remission.
An ulcer can be localized in different parts of the stomach:
- subcardial and cardiac - in the upper part;
- antrum - in the lower section;
- in the body - in the middle part;
- in the pyloric canal - at the transition to the duodenum.
The size of the ulcer is:
- small - up to 5 mm in diameter;
- medium - in diameter 6-19 mm;
- large - 20-30 mm in diameter;
- gigantic - more than 30 mm in diameter.
There are also ulcers associated with the bacterium Helicobacter pylori (hereinafter referred to as HP) and those not associated with it.
The disease occurs in several stages:
- exacerbations - the occurrence of a defect in the mucous membrane;
- scarring - the formation of connective tissue at the site of the ulcer;
- remission - healing of the defect.
The stage of cicatricial and ulcerative deformation of the organ is distinguished separately.
Changes in the oral mucosa in diseases of the gastrointestinal tract
- Changing the language
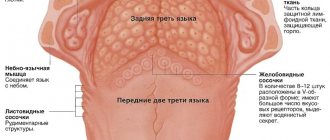
In diseases of the gastrointestinal tract, the condition of the tongue is best studied.
The appearance of the tongue, as many authors believe, can have important diagnostic value and indicate existing pathology of the digestive tract. Changes in the tongue in diseases of the gastrointestinal tract are of a nonspecific nature, manifested by the formation of plaque, swelling, desquamation, atrophy of the papillae, paresthesia, impaired taste sensitivity, and are also quite labile; they can disappear during the period of remission of the underlying disease or during its treatment. Coated tongue is most often detected. Plaque consists mainly of keratinized epithelial cells, bacteria, fungi, and food debris. The severity of plaque depends on various reasons. The amount of plaque on the tongue increases with a decrease in its self-cleaning, mainly during chewing. When assessing the degree of tongue coating, it is important to take into account the composition and consistency of the food consumed, as well as the regularity of individual hygiene measures and other factors. The amount of plaque on the tongue varies throughout the day: there is more in the morning than in the afternoon and evening, since the amount of plaque decreases after eating. Disruption of the process of normal (physiological) keratinization and desquamation of the epithelium also determines the amount and density of plaque. Thus, with atrophy of the filiform papillae of the tongue, there is little or no plaque. With hypertrophy of these papillae, a hard-to-remove thick layer of plaque is formed on the surface of the tongue, consisting mainly of stuck together keratinized filiform papillae.
The condition of the tongue may indicate disorders of the digestive system. Coated tongue is one of the characteristic symptoms of diseases of the gastrointestinal tract. Thus, with exacerbation of gastritis, peptic ulcer, enterocolitis and colitis, the amount of plaque increases, it covers the entire back of the tongue, localizing mainly in its posterior sections. Plaque formation, as a rule, is not accompanied by subjective sensations. Only with a thick, dense layer of plaque on the tongue can a feeling of discomfort and a slight decrease in taste sensitivity occur. Usually the coating on the tongue is grayish-white in color, but it can take on various shades (yellow, brown). The color of plaque is mainly due to dyes in food products, medications or exacerbations of gastrointestinal diseases: peptic ulcer, chronic hepatitis, cholecystitis (yellow, brown).
A swollen tongue is an important sign of gastrointestinal diseases. As a rule, swelling of the tongue is detected by a doctor during examination, since it does not cause pain, except in cases of significant swelling when biting the tongue when eating or talking. The edematous condition is determined upon examination by pronounced tooth marks on its lateral surfaces, as well as an increase in its size. An objective research method to determine the presence of edema is the McClure-Aldrich blister test. Using a blister test, you can determine the state of latent edema, which will allow you to diagnose early (preclinical) changes. V.A. Epishev (1970) described a violation of hydrophilia of the oral mucosa in chronic gastritis. With anacid gastritis, a decrease was found, and with hyperacid gastritis, an increase in the time of resorption of the blister test was established. It should be taken into account that in which a violation of water metabolism is detected.
Changes in the papillae of the tongue are often recorded in pathologies of the digestive tract. The pathogenesis of these changes is mainly due to trophic disorders, as well as a violation of the vitamin balance due to insufficient absorption and synthesis of vitamins B1, B2, B6, B12 by the intestinal microflora.
Depending on the severity and color of the tongue papillae, hyperplastic glossitis can be differentiated from atrophic one.
Hyperplastic glossitis is observed more often in patients with gastritis with high acidity, with exacerbation of peptic ulcer disease. Glossitis is characterized by hypertrophy of the papillae of the tongue, a dense coating, and an increase in the size of the tongue due to severe swelling.
- Atrophic glossitis is found in gastritis with secretory deficiency, hepatitis, gastroenteritis, colitis. With this form of glossitis, atrophy and smoothness of the papillae of the tongue and the absence of plaque are observed. Sometimes the atrophy of the papillae is pronounced, the tongue is smooth and shiny. It may be hyperemic (erythematous) or pale pink. In some cases, the tongue has a “varnished” appearance with bright red spots and stripes, reminiscent of Meller's glossitis. Atrophy of the papillae of the tongue can cause a burning sensation, soreness, and tingling when eating hot and spicy foods.
Desquamation of the epithelium of the tongue is quite often found in diseases of the gastrointestinal tract and can be of varying degrees of severity. Desquamation occurs more often in patients with chronic gastritis with secretory insufficiency, chronic colitis, and liver diseases. It is characterized by the appearance on the back of the tongue of foci of desquamation of the epithelium of filiform papillae. With secretory insufficiency and infectious lesions of the liver, desquamative glossitis is often combined with atrophy and smoothness of the papillae of the tongue. These changes, as a rule, do not cause painful sensations and patients often do not suspect their existence, only sometimes complaining of burning and pain when eating irritating foods. The appearance of foci of desquamation during an exacerbation of a chronic disease of the gastrointestinal tract and their disappearance during remission are characteristic.
Paresthesia of the tongue often accompanies diseases of the digestive system. There is a burning, tingling, tingling sensation on the tongue. These sensations often accompany desquamative glossitis, but can occur without visible changes in the tongue.
Impaired taste sensitivity is determined by the method of functional mobility of its receptors. It is known that the number of functioning receptors depends on the age and condition of the digestive tract. Normally, maximum activity of taste buds is detected on an empty stomach. After eating, their level of mobility decreases. The reaction of the taste buds of the tongue appears in response to incoming excitation impulses from the receptors of the gastric mucosa in a centrifugal manner. In case of peptic ulcer, stomach tumors, due to a disorder of its secretory and motor functions, the reflex connection between the receptors of the tongue and the stomach is disrupted. This is manifested by various changes in the functional mobility of taste receptors (increased activity and lack of demobilization after eating, etc.). Disturbances in taste sensitivity can also occur with changes in the papillary apparatus of the tongue (heavily coated tongue, atrophy or desquamation).
- Lesions of the oral mucosa
Erosive and ulcerative lesions of the oral mucosa, developing in diseases of the gastrointestinal tract, are predominantly a consequence of trophic disorders. There are a large number of reports on the presence of erosions and ulcers on the oral mucosa due to gastric ulcers, liver diseases, colitis, enterocolitis, etc. There is a known connection between recurrent aphthous stomatitis and gastrointestinal pathology. Approximately 50% of patients with diseases of the gastrointestinal tract (chronic gastritis, gastric and duodenal ulcers) suffer from recurrent aphthous stomatitis of varying severity.
Changes in the color of the oral mucosa can occur against the background of gastrointestinal pathology. During the period of exacerbation of peptic ulcer, enterocolitis, colitis, catarrhal gingivitis, glossitis or stomatitis often develop, the severity of which depends on the duration and frequency of exacerbations of the underlying disease. The oral mucosa in the affected area is characterized by hyperemia with symptoms of cyanosis due to the chronic course of the process. In this case, patients complain of a burning sensation in the mouth, changes in the color of the mucous membrane, and sometimes pain when eating irritating foods. The most pronounced phenomena are catarrhal gingivitis and stomatitis during exacerbation of chronic colitis. During the period of remission of gastrointestinal diseases, the symptoms of catarrhal gingivitis or stomatitis become mild or completely disappear.
It should be remembered that such changes in the oral mucosa can be manifestations of other diseases and conditions of the body (infectious, including fungal, allergic, cardiovascular, hypovitaminosis). In this regard, for successful diagnosis and selection of treatment methods, a thorough examination of the patient is necessary.
Salivation disorders can manifest as hyper or hyposalivation. Studies by a number of authors have proven that patients with gastric and duodenal ulcers experience morphological and functional changes in the minor salivary glands. With peptic ulcer disease in the initial stage (for up to a year), as well as its exacerbation, salivation increases with the subsequent development of hyposalivation. Patients begin to complain of dry mouth. Clinically, impaired salivation is often combined with other previously described changes in the oral cavity, characteristic of gastrointestinal pathology.
Main causes
The cause of a defect in the gastric mucosa is considered to be an imbalance between the aggressive secretions of the stomach and the protective qualities of the mucous membrane. To digest food, the stomach secretes pepsin and hydrochloric acid. To prevent them from destroying the stomach, mucus forms on its surface, protecting the organ. If more acid is produced and less mucus is produced, an ulcer may form. The background for such a pathology may be a decrease in gastric motility, a violation of the regenerative - restorative properties of the mucous membrane against the background of certain diseases.
The main etiological cause of ulcer formation is damage to the mucous membrane of the HP. This bacterium successfully survives in an acidic environment and produces an enzyme that causes an inflammatory reaction with subsequent formation of a defect. Helicobacter pylori is detected in 82% of patients suffering from gastric ulcers.
Another reason may be uncontrolled use of anti-inflammatory non-steroidal drugs, such as aspirin.
Provoking factors may be:
- smoking and alcohol abuse;
- constant consumption of spicy food;
- stressful situations;
- hereditary predisposition;
- dry food;
- eating disorder.
Gastric ulcers often develop against the background of certain diseases, such as atrophic gastritis and hormonal pathologies.
Causes of peptic ulcer
One of the main causes of peptic ulcer development is currently considered to be infection caused by the microorganism Helicobacter pylori (H. pylori). However, it should be noted that approximately more than half of the world's population is infected with H. pylori infection, and in many people this infection is asymptomatic; some of those infected develop chronic gastritis, atrophic gastritis, and stomach cancer. The effect of Helicobacter pylori on the gastric mucosa may depend on the state of the host’s immune system; the development of peptic ulcer disease depends on the presence of associated factors.
Factors contributing to the development of peptic ulcer disease (risk factors)
- Neuropsychic factor (stress).
- Smoking (smoking also impairs the healing of ulcers and increases the likelihood of their re-development - relapses; the degree of risk when smoking tobacco depends on the number of cigarettes smoked per day).
- Heredity.
- Violation of the regime and nature of nutrition.
- Alcohol abuse.
For the occurrence of a peptic ulcer, as a rule, it is not the isolated action of one of the listed factors that is necessary, but their combination. From a modern point of view, the development of peptic ulcer disease appears to be the result of an imbalance between the factors of “aggression” and the factors of “protection” of the mucous membrane of the stomach and duodenum. Factors of aggression (acid, gastroduodenal dyskinesia, Helicobacter pylori, etc.) prevail over protective factors (mucoproteins and bicarbonates of mucus, mechanisms for regulating the production of gastric juice, etc.).
Endoscopic stages of peptic ulcer
- open ulcer,
- scarring ulcer,
- stages of red scar, white scar.
Ulcer size
- small (less than 0.5 cm);
- medium (0.5–1 cm);
- large (1.1–3 cm);
- gigantic (more than 3 cm).
Symptoms of the disease
Peptic ulcer usually manifests itself more often in spring and autumn, during the period of exacerbation of the disease. The first sign of the disease is pain that occurs immediately after eating. This is due to the fact that pepsin and hydrochloric acid released during meals aggressively affect the defect unprotected by mucus. Moreover, the manifestations of pain symptoms increase within an hour after eating. The pain is localized in the epigastric region, in the region of the heart, and can radiate - radiate under the scapula, as in a heart attack. At the height of the pain syndrome, nausea often occurs, which can result in vomiting, which brings relief.
Other dyspeptic manifestations and signs of illness: heartburn, loss of appetite, constipation. A coated tongue may indicate stomach problems. Against this background, the patient quickly loses weight.
Clinical picture of peptic ulcer
The most consistent and important symptom of peptic ulcer disease is pain. Pain in peptic ulcer disease has a clearly defined rhythm (time of occurrence and connection with food intake), and seasonality of exacerbations.
Based on the time of occurrence and their connection with food intake, pain is distinguished between early and late, night and “hungry”. Early pain occurs 0.5–1 hour after eating, lasts 1.5–2 hours and decreases as gastric contents are evacuated. Such pain is more typical for gastric ulcer in the upper part.
Late pain appears 1.5–2 hours after eating, night pain occurs at night, and “hungry pain” occurs several hours after eating and stops after eating. Late, night and “hungry” pains are more typical for the localization of an ulcer in the antrum of the stomach or duodenal ulcer.
The nature and intensity of pain may vary (dull, aching, burning, cutting, cramping). The localization of pain in peptic ulcer disease is different and depends on the location of the ulcer: with an ulcer on the lesser curvature of the stomach, pain often occurs in the epigastric region, with duodenal ulcers - in the epigastric region to the right of the midline. With ulcers of the cardial part of the stomach, pain can be behind the sternum or in the heart area; in this case, it is important to differentiate peptic ulcer disease from angina pectoris or myocardial infarction. Pain often occurs after taking antacids, milk, food, and even after vomiting.
In addition to pain, the typical clinical picture of peptic ulcer disease includes various dyspeptic symptoms.
Heartburn is one of the early and frequent symptoms characteristic of peptic ulcer disease. Heartburn can occur at the same time after eating as pain. It often precedes the onset of pain, and subsequently is often combined with pain. These two symptoms are closely related, and some patients have difficulty distinguishing between them. In later stages of the disease, heartburn may disappear. But sometimes it can be the only subjective manifestation of a peptic ulcer.
Belching is a fairly common, but not specific symptom of peptic ulcer disease. The most typical belching is sour. The appearance of belching is associated with impaired evacuation of gastric contents due to prolonged spasm and severe inflammatory edema of the pylorus or duodenal bulb. It should also be remembered that belching is characteristic of a diaphragmatic hernia.
Nausea and vomiting are dyspeptic symptoms characteristic of exacerbation of peptic ulcer disease. Nausea is often accompanied by vomiting, although vomiting can occur without preceding nausea.
Vomiting in patients with peptic ulcer disease often has some specific features: firstly, it occurs at the height of pain, being, as it were, the culmination of pain; secondly, it brings significant relief. Vomit, as a rule, has an acidic reaction with an admixture of recently eaten food. Vomiting can also occur on an empty stomach.
Appetite in case of peptic ulcer is usually preserved or even increased (the so-called painful feeling of hunger). Decreased appetite is possible with severe pain syndrome; fear of eating may occur due to the possibility of pain occurring or increasing. Decreased appetite and fear of food can lead to significant weight loss for the patient.
Constipation is observed in half of patients with peptic ulcer disease, especially during exacerbation. Constipation in peptic ulcer disease is caused by a number of reasons: spastic contraction of the colon, a gentle diet, poor coarse fiber and the resulting lack of intestinal stimulation, limitation of physical activity, and the use of antacids (Almagel, etc.).
Symptoms depend on the location of the ulcer and the age of the patient . In some cases there may be no pain (painless ulcers). In these cases, ulcers are discovered when complications develop (ulcer bleeding, ulcer perforation - breakthrough of the ulcer wall into the abdominal cavity, penetration of the ulcer). Only about half of people with duodenal ulcers (duodenal ulcers) have typical symptoms. In children, the elderly, and patients taking certain medications, symptoms may be atypical or absent altogether.
Treatment of the disease
Gastric ulcers are well treated with conservative methods, which include pharmacotherapy and physiotherapeutic procedures. In emergency and some other cases, surgical intervention is indicated.
Drug treatment
The treatment of gastric ulcers uses complex pharmacotherapy, including medications aimed at the root cause of the pathology, relieving irritation of the mucous membrane and creating a protective barrier for gastric juice and relieving pain. The main group of drugs includes:
- Proton pump inhibitors are long-acting drugs that reduce gastric secretory activity.
- Antacids - envelop the mucous membrane, protecting it from the aggressive effects of gastric juice, and reduce its acidity.
- Antibacterial drugs are aimed at eradication (destruction) of Helicobacter pylori. The best effect is achieved when antibiotics are combined. For peptic ulcers, macrolides, antiprotozoal drugs, penicillin and tetracycline antibiotics are prescribed.
- Bismuth preparations relieve inflammation and form an insoluble colloid that creates a protective film when combined with protein.
- Vitamin B5 (Pantothenate) - normalizes the production of hydrochloric acid, stimulates the regeneration of the mucous membrane.
- Methylmethionine sulfonium chloride, also called vitamin U, acts as a cytoprotector that helps reduce gastric secretion and heal gastric ulcers.
Treatment can be supplemented with other drugs aimed at eliminating the causes of ulcerative pathology.
Physiotherapy
Physiotherapy helps ulcer healing and can be used in complex therapy. The mechanisms of self-regulation and adaptation are beneficially affected by:
- laser puncture - exposure of bioactive points with a laser beam;
- EHF therapy - the influence of electromagnetic waves in the millimeter range;
- magnetotherapy - exposure to low-frequency magnetic fields.
Ultrasound therapy is used to improve gastric motility in case of gastric atony. This procedure also improves blood supply to the organ, reduces the number of bacteria and relieves inflammation.
Surgery
Emergency surgery is performed in case of massive bleeding and perforated gastric ulcer. Surgical intervention is also indicated for complicated forms of ulcers in the case of a non-healing ulcer, as well as for malignancy, when the pathology becomes malignant. In some cases, gentle methods are used: laparoscopy or endoscopy.
specialist
Our doctors will answer any questions you may have
Tumasova Anna Valerievna Gastroenterologist
Diet and bad habits for stomach ulcers
Diet for gastrointestinal ulcers is an essential part of treatment. During the acute period, nutrition should be as gentle as possible, gentle on the mucous membrane and not stimulating the secretory activity of the stomach. In the first two days, preference is given to slimy soups with rice water without vegetables and meat, jelly or warm tea with sugar and crackers. In the next 6 days, table No. 1 is used in therapeutic nutrition.
Authorized Products
General nutrition rules:
- include easily digestible foods in the diet;
- food should be warm
- Do not eat cold or hot foods;
- you need to eat slowly, in small portions
- products need to be crushed and ground;
- Baking, boiling, stewing is allowed;
- fried foods and spices are excluded;
- the break in eating should not be more than 3 hours;
- food must be chewed thoroughly.
The following foods and dishes are allowed for stomach ulcers:
- Slimy soups: with the addition of rice, semolina, oatmeal, you can add cream or butter;
- Slimy porridges: with water or milk from the same cereal, you can add cream;
- Fish and meat: lean beef, veal, turkey, rabbit, chicken. To prepare the meat, you need to boil it, pass it through a meat grinder, add butter, bake it into a soufflé puree, you can cook steamed cutlets, meatballs, meatballs;
- Eggs: soft-boiled, or steam omelet;
- Berries and fruits: baked unsweetened fruits, dried fruit compotes;
- Dairy products: milk, steamed pureed cottage cheese soufflé, cream.
- Drinks: weak tea with added cream or milk, rosehip decoction, milk or fruit jelly.
You can add refined vegetable oil or unsalted butter to dishes.
Prohibited Products
During an exacerbation, foods that irritate the gastric mucosa and increase the production of gastric juice are excluded: fatty meat, baked goods, preserves, canned and smoked foods, confectionery with cream, dishes with vinegar and spices, garlic.
Do not include vegetables with coarse fiber in the diet, as well as radishes, radishes, daikon, cabbage, tomatoes, turnips, and mushrooms.
It is necessary to avoid foods that cause fermentation processes: legumes, sweet fruits and juices, carbonated drinks.
During the treatment period, you are strictly prohibited from smoking and drinking alcohol.
Foods High in Iron
Our body cannot synthesize iron; it only processes this element, extracting it from worn-out red blood cells. “Fresh” iron comes from food. However, even if you eat foods containing iron, this does not mean that you have enough. The thing is that there are two types of iron.
Iron can be heme (divalent) or non-heme (trivalent). The first is found in products of animal origin and is easily digestible (about 25%), the second is part of plants and is absorbed by only 8–10% maximum[3]. This is why vegans and vegetarians often lack this element, even if they eat foods rich in iron.
And yet, it is the right diet that is considered the main way to prevent iron deficiency. Iron is found in significant doses in the following foods:
Animal products:
- pork liver - 29 mg (hereinafter the figure is given per 100 g of product);
- hard cheese - 19 mg;
- beef liver - 9 mg;
- egg yolk - 6 mg;
- beef tongue - 5 mg;
- turkey - 4 mg;
- beef - 2.8 mg;
- chicken - 2.5 mg;
- mackerel - 2.5 mg;
- pork - 1.6 mg;
- herring - 1 mg;
- cottage cheese - 0.4 mg.
Products of plant origin:
- beans - 72 mg;
- hazelnuts - 51 mg;
- oat flakes - 45 mg;
- fresh forest mushrooms - 35 mg;
- millet - 31 mg;
- peas - 20 mg;
- seaweed - 16 mg;
- prunes - 13 mg;
- dried apricots - 12 mg;
- buckwheat - 8 mg;
- tofu - 5.5 mg;
- peaches - 4.1 mg.
Although the iron content of some plant foods is high, the non-heme form of iron is poorly absorbed. Therefore, it is important for those following a plant-based diet to check their iron levels and, if necessary, take dietary supplements that contain this element.
Our body perceives iron best from meat (on average 20% is absorbed), a little worse from fish and seafood (about 11%), legumes (7%) and nuts (6%). Only 1-3% of iron is absorbed from fruits, vegetables and cereals.
To improve the absorption of iron, it is also important to receive the right amounts of vitamins and minerals, which play the role of catalysts and help this element to be absorbed. These include:
- Vitamin C. Iron is almost not absorbed without ascorbic acid, so the menu must include foods rich in ascorbic acid - berries, oranges and grapefruits, cabbage, red peppers.
- Vitamin A. If a person lacks vitamin A, then iron will not be absorbed and used to “build” new red blood cells. Many orange and yellow fruits and vegetables are rich in vitamin A - it is this substance that gives them their cheerful colors. To replenish vitamin A reserves, you need to eat more dried apricots, carrots and pumpkin. However, it's important to know that fats are needed for this vitamin to be absorbed, so don't ignore sources of retinol like butter, fish oil, and egg yolks.
- Folic acid (vitamin B9). It helps absorb iron and normalizes the digestive tract, and healthy digestion is extremely important for the absorption of this element. Sources of folic acid are eggs, soybeans, yeast, green leafy vegetables, dill, eggplant, tomatoes, chicken liver.
- Copper. Sources of copper are offal, fish and seafood (shrimp, oysters, etc.), cabbage.
Prevention of peptic ulcers
Stomach ulcers can be avoided if you follow some rules. First of all, give up bad habits, since ethyl alcohol and tobacco reduce the protective properties of the mucous membrane and irritate it.
Diet is no less important in prevention: you need to eat at a certain time, the interval between meals should not exceed 4 hours. You cannot eat dry food, as dry rough food injures the walls of the stomach.
For those who work at night, it is recommended to change jobs to work only during the daytime. It is necessary to avoid stress, treat inflammation of the stomach, hormonal diseases, and visit a gastroenterologist at least once every six months.