Composition and properties of tooth enamel
The composition of tooth enamel consists mainly of inorganic substances (more than 95%). Organic substances are represented by proteins, lipids and carbohydrates. The hardness of the enamel layer is determined by the increased content of inorganic substances in it. About 3% of the composition is water. This is where such high strength is achieved. The chemical composition of enamel is unique. The high content of inorganic substances in it ensures that it performs its main functions - protecting the deeper layers of the tooth. Inorganic substances include hydroxyapatite crystals. It is a mineral that contains various elements, including fluorine, magnesium and others. It is because of these crystals that the enamel is so sensitive to the effects of acids. The integrity and density of the enamel layer depend on calcium ions. Calcium is also part of the enamel of teeth and bones. Enamel, consisting of many elements, has a rich composition, which determines its properties.
Enamel composition
- Minerals (up to 95%);
- organic matter (1.2%);
- water (3.8%).
Depending on the thickness, the enamel changes color - from white to yellow. In the thinnest places where the dentin is visible, the tooth looks yellowed. The degree of mineralization affects the transparency of the tissue. The more minerals in the composition, the more transparent the surface will be. For this reason, baby teeth, which are less saturated with minerals than molars, look whiter.
- Enamel is a tissue that is not capable of regeneration, since it does not contain cells.
- It constantly metabolizes ions coming from saliva, dentin and pulp.
- The tissue is characterized by mutual permeability, with the least permeability characteristic of the external surfaces adjacent to the oral cavity.
What is included in the structure: basic elements
The structure of the tooth is complex, it includes not only the enamel. Dentists divide this layer into three components that are connected to each other:
- Prism. Consists of one ameloblast cell. These elements are a kind of foundation of the enamel, running across its entire thickness perpendicular to the connection of the protective layer with dentin. According to their shape, prisms are divided into oval, arched and polygonal; their thickness ranges from 3 to 5 microns.
- Interprismatic substance. This is a kind of binding component that tightly envelops all enamel prisms. The level of mineralization of this substance is slightly lower than that of prisms, and its thickness cannot exceed one micron. The spindles are located in the interprismatic space. These are a kind of processes of odontoblasts, the bodies of which are enclosed in the nucleus pulposus. The spindles grow from the area where the pulp is located, penetrating the enamel and reaching its surface. The processes are responsible for the ability to recognize toothache.
- The cuticle is the most important component of the composition; it is the surface shell of the enamel, which, after eruption, is erased in the area of their chewing surface and is partially preserved in the lateral areas.
Many studies have been devoted to the characteristics of the chemical composition of tooth enamel. Scientists have studied this component in detail in order to create new, more effective methods of dental treatment. Knowing exactly the composition of enamel, it is possible to develop highly effective means for strengthening and restoring it.
In addition to the main components of the enamel layers, it also contains others:
- Neonatal line - visually looks like a dark stripe, present only on milk units. This strip is located in places where two types of enamel intersect: the layer formed before the birth of the child, and the layer that formed immediately after the baby was born.
- Bundles and plates are specific formations that contain hypomineralized prisms; between them there is an interprismatic substance consisting of the same material as the prisms themselves. Chemical analysis demonstrates that, in terms of molecular structure, this material contains a huge amount of protein compounds. Many dentists unanimously claim that it is through the tufts that various bacteria enter the inner layers of enamel from the oral cavity. Then they make their way further, getting into the layers located inside the tooth, thereby causing caries.
- Gunter-Schräger stripes are stripes that stand out in shades on the enamel surface. The shade can be light or dark. Located in a perpendicular position relative to the surface of the enamel, they are formed as a result of opening the prisms.
- Retzius lines are shaped like slightly offset arches, located symmetrically to each other.
Photos of teeth under a microscope or what plaque actually looks like
While you might think these photos are of rare plants or exotic landscapes, what you're actually seeing is photos of plaque and microorganisms living in your gum area or on your toothbrush, as well as the decay caused by these bacteria. The images were obtained using a microscope that uses a directed flow of electrons for imaging. To make the details more clear, the images were processed using computer graphics.
Dental plaque under a microscope (400x magnification, photograph on 10-centimeter film). It is an accumulation of bacteria in the form of a film trying to colonize the surface of the tooth.
The same plaque at 10 thousand times magnification.
Photo of a baby tooth (incisor). Most of the tooth consists of dentin, a substance that envelops the cavity in which soft connective tissue, blood vessels and nerves are located. The crown of the tooth is covered with enamel (in the photo - the white area above the dentin). This is a stronger, mineralized substance that protects dentin from the effects of acids in the oral cavity. The root of a healthy tooth does not come into contact with acids in the mouth; in this part, dentin is protected by a cementitious substance (pink in the photo). It serves to adhere the periodontal ligaments to the surface of the tooth, reliably fixing its position.
The photo shows a section of a tooth. Blue indicates the enamel-forming layer of the cell, yellow indicates the surface of the tooth, and red indicates dentin. Depletion of the enamel or cementum exposes dentin (a porous substance with microscopic channels called dentinal tubules connecting the pulp), causing tooth sensitivity.
Yellow indicates the layer of bacteria that forms plaque on the surface of the tooth. During the digestive process, bacteria release acid, which causes demineralization of the tooth. As a result, caries develops, requiring treatment and installation of a filling, otherwise the carious lesion can lead to tooth extraction.
An incisor with a carious cavity or demineralization of the tooth caused by bacterial activity. In this case, caries formed on the lateral surface (between two teeth). Also visible in the photo is cervical caries (between the crown and the root of the tooth - indicated in yellow), which appeared due to improper or insufficient use of dental floss.
Yellow indicates the accumulation of bacteria on the gums.
Tooth surface (yellow) with a colony of spherical bacteria (blue) and red blood cells (red).
Toothbrush bristles.
The bristles of a used toothbrush are covered with plaque. After cleaning, rinse the brush thoroughly and remove any remaining toothpaste or plaque particles from it, then dry it in an upright position.
Plaque on the bristles of a used toothbrush at 750x magnification.
Special interdental brushes with a small head covered with bristles, designed to clean teeth in hard-to-reach areas.
Detailed image of a used interdental brush covered in plaque.
Crown of a baby tooth. The root of the tooth has become exfoliated as a result of temporary tooth resorption caused by the pressure of the growing molar.
A colony of bacteria forming plaque at 1000x magnification.
Plaque.
Plaque at 8 thousand times magnification.
A drill attachment designed to remove soft tissue and bacteria from a carious cavity.
Drill tip.
Calcium phosphate crystals contained in dental solutions for remineralizing teeth.
Pin (used to strengthen the filling in case of extensive carious lesions or the absence of part of the tooth).
Specifics of enamel of baby teeth
The main feature of the enamel of the first dental units is that this layer is not as strong as that of permanent teeth. This can be justified by the fact that much fewer mineral compounds are concentrated in baby teeth. If you study the composition of children's enamel in detail and examine it under a microscope, you can draw the following conclusions:
- The Retzius lines, which we mentioned above, are not as pronounced as on constant units.
- The prisms are placed in a horizontal direction.
- There are many microscopic cracks in the enamel of a baby tooth, hence the porosity of its structure.
Given this information, pediatric dentists claim that children's enamel is more susceptible to wear and destruction. For this reason, caries progresses at an intensive rate in children.
Damage to enamel: what to do
One of the most common phenomena is damage to the enamel. There are several types of lesions. It is worth considering that all types of lesions can be classified into two groups: those that formed before the eruption of baby teeth, and those that arose after. The first category includes the following pathologies:
- Dysplasia – there are a lot of symptoms of the disease: the formation of spots, thinning of the enamel layer. Most often, this pathology is associated with genetics and is often accompanied by problems with bone development. Teeth affected by dysplasia erupt with an initially irregular shape.
- Hypoplasia. Tooth tissues atrophy or are absent altogether. The formation of spots, changes in shade, thinning of the enamel are the main signs of the disease. To treat this problem, medications are prescribed that help restore mineral balance.
- Hyperplasia is excess tissue growth. It can also be caused by a mineral imbalance. Various blood diseases and hormonal imbalances can lead to the development of hyperplasia of the tooth buds. Enamel “drops” appear on the tooth surface. In rare, particularly difficult cases, hypertrophied areas can be filled with dentin or pulp.
- Fluorosis. The disease is characterized by the appearance of spots and furrows. Small pits or streaks may appear. Pathology is caused by excess fluoride content in the body. Often the disease affects baby teeth.
Below we will consider pathologies that are not associated with genetics and congenital anomalies:
- Erosion refers to non-carious lesions of the enamel layer and dentin. Erosion can be triggered by gastrointestinal diseases, excessive consumption of too acidic foods, and taking certain types of medications. Drug treatment is prescribed.
- Hypersensitivity. When a person reacts painfully to too cold or hot, this indicates the development of tooth sensitivity, which is often accompanied by thinning of the enamel. In this case, the task is to strengthen the layer. Minerals and vitamins are prescribed.
- Wedge-shaped defect. The pathology is that the neck of the tooth is gradually exposed, and the base is destroyed. The disease can be triggered by thyroid disease, gastrointestinal problems, and gum disease.
- Caries. If the carious lesion of the enamel layer is not eliminated in a timely manner, the disease will spread to the dentin and soon reach the pulp. The disease is treated by cleaning the cavity and installing a filling there.
- Impacts of a mechanical nature. Chips and cracks often form on the enamel. Modern dentists, using advanced equipment, can restore the damaged area.
Mineralization of teeth and why is it needed?
Not only adults, but also children are currently faced with dental problems. In children, dental problems can arise from a lack of minerals and vitamins during fetal development, when the fetus is developing teeth. When teeth erupt, the period of primary mineralization of enamel begins. At this stage, the tooth enamel is still immature. As the tooth functions, minerals are transferred from saliva to the enamel. After 2-4 years, the optimal content of mineral substances is observed in it and its layer is compacted. The general mineralization of the tooth is constantly maintained due to the mineral composition of the oral fluid, that is, saliva. The most important function of which is mineralizing. Thanks to this function, the “enamel maturation” of erupted teeth occurs.
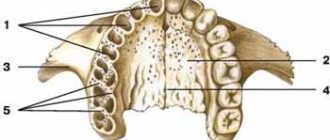
Enamel is the hardest and most mineralized component. It covers the outside of the tooth crown. Its thickness varies depending on the location on the crown and the shape of the tooth. It reaches its greatest thickness on the cutting edge of the anterior (frontal) and on the tubercles of chewing teeth (molars and premolars). In the area of fissures (recesses), the lateral surfaces of the tooth crown and in the area of the necks of teeth, the thickness of the enamel is much less.
Here we can see the connection between the thickness of the enamel and the areas of its demineralization. The hardness of enamel is due to its high content of mineral salts. The mineralization process is significantly influenced by the nature of nutrition, disorders of phosphorus-calcium metabolism (rickets), fluoride content in drinking water, and the general condition of the body.
The condition of permanent teeth can be influenced by diseases of the endocrine system, impaired digestion of food (with celiac disease, dysbacteriosis), diseases of the gastrointestinal tract, excessive consumption of sugars, insufficient oral care, lack or, conversely, excess of certain minerals, changes in the composition of saliva (its mineralizing capacity).
Saliva plays a vital role in maintaining the balance of the processes of mineralization and demineralization of tooth enamel. If the mineral composition of the enamel is disturbed, the resistance (stability) decreases and the risk of demineralization of the enamel increases.
One of the methods for correcting disorders is enamel remineralization. This procedure is carried out both for the purpose of prevention and for teeth that already have significant damage to the enamel. All means for remineralizing enamel can be divided into two groups. The first group includes products based on fluorine compounds. The second group includes products without fluoride, but containing hydroxyapatite particles or calcium compounds.
The remineralization procedure can be carried out both at home and after professional oral hygiene. Before carrying out remineralization therapy, it is important that the teeth are cleaned of any type of plaque. A qualified specialist must assess the condition of the dental tissues and decide which methods are indicated in each specific case. After professional oral hygiene, a specialist can use a highly effective polishing paste based on a high concentration of nanohydroxyapatite, and also prescribe it for home use, applied to the teeth after daily brushing, or used in mouth guards. For isolated areas of enamel demineralization, teeth are coated with varnish.
There are also complexes that contain an anhydrous fluorine compound and a highly dispersed calcium compound, which ensures deep penetration of particles with the formation of submicroscopic crystals of calcium fluoride, which provide long-term protection for 1 year.
During enamel treatment, deep penetration of substance ions into micropores occurs, due to which remineralization occurs. The procedure of deep mineralization is relevant if the active development of caries begins, as well as for the mineralization of “immature enamel”.
It is important to strengthen a child’s enamel from the beginning of the eruption of baby teeth until the end of the formation of a permanent bite, until about 11-12 years of age. Remineralization is indicated after professional oral hygiene, after a whitening procedure, for demineralization of enamel (white spot), during and after orthodontic treatment, and increased sensitivity of enamel.
Preserving the integrity of enamel in childhood is the key to healthy teeth in the future.
Methods of strengthening
To eliminate pathologies associated with tooth enamel, dentists use various techniques, both therapeutic and orthopedic. For severe lesions, crowns or veneers are used. But the best option for every person is to try to preserve their own healthy teeth. What options for strengthening enamel are suitable for an adult:
- Take vitamins and minerals regularly.
- Use preventive and therapeutic agents – gels and pastes containing calcium and fluoride.
- Regularly visit the dental office for preventive examinations and professional cleanings. This will not only protect the enamel, but also prevent the development of caries.
- If the enamel is damaged and visual appeal is lost, you can undergo a whitening procedure, but only after prior consultation with your doctor.
For children, dentists recommend fluoridation, fissure sealing and other procedures aimed at comprehensively strengthening teeth. Parents should pay attention to their child's diet. It should not contain sweet soda or excessive amounts of sweets. Since tooth enamel contains a large number of microelements, it is worth taking vitamins periodically, after consulting with a pediatrician and pediatric dentist.
Types of damage to tooth enamel before teething
Dysplasia
A number of disorders, which is characterized by a number of signs: gray spots, thinning of the enamel or the absence of fragments of the enamel layer. In the vast majority of cases, dysplasia is associated with genetic abnormalities, metabolic disorders and bone diseases. When teething, teeth may be irregular in shape (triangular, pear-shaped, etc.).
To treat erosion of tooth enamel, multivitamins, sodium fluoride, and electrophoresis are prescribed. In case of extensive lesions, artistic restoration and prosthetics are used to restore aesthetics. To avoid complications, dental enamel dysplasia in children requires immediate treatment.
Hypoplasia
With hypoplasia, atrophy of tooth tissue or its complete absence is observed at the intrauterine level. Usually the disease is associated with a mineral imbalance. Hypoplasia is expressed by a change in color (to gray or brown), the appearance of spots, thinning of the enamel and even its complete absence (aplasia).
When treating thinning enamel, medications are prescribed to restore mineral balance (calcium gluconate solution, etc.), as well as a complex of vitamins. In case of aesthetic problems, whitening can be performed, and in severe cases, the tooth is covered with a crown or veneer.
Hyperplasia
Excess dental tissue, the appearance of which is also caused by an imbalance of mineral balance (usually due to hormonal imbalances in parents or blood diseases). On the surface of the tooth, so-called enamel drops are formed - islands of brown or reddish color. For more complex anomalies, hypertrophied areas can be filled with dentin or pulp.
Treatment of hyperplasia includes polishing teeth with a drill, applications and rinsing with fluoride and calcium solutions in combination with taking medications that normalize the mineral composition and eliminate the root cause of the deviation.
Fluorosis
When dental fluorosis occurs, spots, grooves, pits, or streaks form on the surface of the enamel. The disease is caused by an excess of fluoride in the body and often occurs in children.
Remineralization of enamel, grinding of teeth, and normalization of the amount of fluoride in the body are indicated. In difficult cases - orthopedic treatment and artistic restoration.
Changes in the structure and violation of the integrity of the enamel can be caused by a number of genetic abnormalities and hereditary diseases. That is why it is important to establish the root cause so that the best treatment can be prescribed if tooth enamel is damaged or atrophied.