Caries is a local lesion of dental tissues, implying a long process of demineralization, during which a carious cavity is formed. In dentistry, there is a clear classification of dental caries.
The basic principle of caries classification is determined taking into account the depth of damage to dental tissues. The causes of tooth decay are bacteria that need to be removed by brushing your teeth daily.
Caries: its types and classification
Uncomplicated caries:
This is the name of the initial stage of damage to tooth tissue. Caries manifests itself as a small focus of demineralization on the surface of the tooth enamel in the form of a small, light or dark spot. The primary stage of the second degree is characterized by the formation of a carious cavity that does not reach the border between enamel and dentin. Deep tissue damage is manifested by the fact that caries penetrates deeper into the tooth, but without yet affecting the pulp, which is protected by a thin layer of dentin.
Complicated caries:
When caries becomes more severe, it manifests itself as:
- pulpitis – acute inflammation of the neurovascular bundle of the tooth;
- periodontitis is an inflammation of the oral tissues between the alveolar process and the tooth.
Histological classification consists of several points:
- primary damage to tooth enamel;
- damage to the enamel and thin layer of dentin;
- damage to cement:
- dental caries in remission.
According to the depth of tissue damage
The WHO classification (ICD-10) played a significant role in the systematization of carious diseases. It helped regulate the intensity of damage to dental tissues. This system identifies the following stages of the disease:
- Enamel damage. This is the initial and superficial stage, which may appear as stains and roughness on the teeth.
- Damage to dentin. At this stage, the destructive process goes beyond the enamel.
- Caries of dental cement. The destruction is localized in an area of tissue that covers the root and neck of the tooth with a thin layer.
- Suspended caries.
- Odontoclasia (demineralization of enamel areas).
- Another specified type of disease.
- Unspecified caries.
In the practice of dentists, when making a diagnosis, only the first three codes from the specified list are used. One of the significant disadvantages of diagnosing caries according to WHO is the absence in the classification of initial forms of enamel damage that can be cured by non-invasive methods. With this in mind, the International Carious Disease Assessment System (ICDAS) was introduced in 2004.
Free consultation
30-40 minutes
inspection and diagnostics
treatment plan and cost
Make an appointment
Classification of caries according to Black
This classification of caries intensity was proposed in 1896 by Dr. Black. The essence of the classification is to standardize the methods of filling and removing affected dental tissues. Each class of cavity should be treated using its appropriate filling technique. Levels of carious lesions:
- lesions in the area of natural fissures and in the pits of all teeth in the mouth;
- damage to all surfaces of premolars and molars;
- lesions in the area of the incisors and, rarely, the canines, which do not violate the integrity of the cutting edge;
- damage to all canines and incisors with deformation of the cutting edge;
- damage to all teeth located on the vestibular surface.
- extensive carious lesion.
K02.2 Cement
Compared to damage to enamel (initial stage) and dentine, cementum (root) caries is diagnosed much less frequently, but is considered aggressive and harmful to the tooth.
The root is characterized by relatively thin walls, which means that the disease does not take much time to completely destroy the tissue. All this can develop into pulpitis or periodontitis, which sometimes leads to tooth extraction.
Clinical symptoms depend on the location of the disease focus. For example, when the cause is located in the periodontal area, when the swollen gum protects the root from other influences, we can talk about a closed form.
With this outcome, no obvious symptoms are observed. Usually, with a closed location of cement caries, there is no pain or it is not expressed.
Photo of an extracted tooth with cement caries
In an open form, in addition to the root, the cervical area can also be destroyed. The patient may be accompanied by:
- External disorders (especially pronounced in the front);
- Inconvenience while eating;
- Painful sensations from irritants (sweets, temperature, when food gets under the gum).
Modern medicine makes it possible to get rid of caries in several, and sometimes even in one, dentist appointment. Everything will depend on the form of the disease. If the gum covers the lesion, bleeds, or greatly interferes with the filling, then gum correction is performed first.
After getting rid of the soft tissue, the affected area (with or without exposure) is temporarily filled with cement and oil dentin. After the tissue has healed, the patient comes back for a second filling.
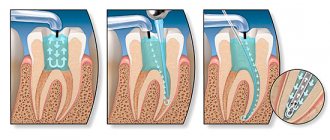
How to treat caries?
It is worth noting that in order to prevent the development of caries, it is recommended to visit the dentist once every six months. When the first stage of caries is detected, a high-quality filling is installed, and the carious area is removed with a drill. If caries is not treated, it progresses to more complex stages, with a large affected area, and then surgical intervention cannot be avoided. If you notice dark spots on your tooth enamel, contact your dentist immediately.
Medium caries is treated in one visit to the doctor, deep caries in 2 visits, and caries in particularly complex forms requires 3 or more visits to the clinic.
Today, caries can be treated without pain, effectively and comfortably for patients. So there is no need to delay going to the doctor. In addition to the drill, caries treatment methods include the microinvasive method, ozone therapy, air abrasive treatment and laser treatment.
General information
Doctors have repeatedly made attempts to create a single, universal system of classifications of human diseases.
As a result, in the 20th century the “International Classification - ICD” was developed. Since the creation of the unified system (in 1948), it has been constantly revised and supplemented with new information.
The final, 10th revision was carried out in 1989 (hence the name ICD-10). Already in 1994, the International Classification began to be used in countries that are members of the World Health Organization.
In the system, all diseases are divided into sections and marked with a special code. Diseases of the oral cavity, salivary glands and jaws K00-K14 belong to the section of diseases of the digestive system K00-K93. It describes all dental pathologies, not just caries.
K00-K14 includes the following list of pathologies related to dental lesions:
- Item K00. Problems with development and teething. Adentia, the presence of extra teeth, abnormalities in the appearance of teeth, mottling (fluorosis and other darkening of the enamel), disturbances in the formation of teeth, hereditary underdevelopment of teeth, problems with teething.
- Item K01. Impacted (sunk) teeth, i.e. changed position during eruption, in the presence or absence of an obstacle.
- Item K02. All types of caries. Enamel, dentin, cement. Suspended caries. Pulp exposure. Odontoclasia. Other types.
- Item K03. Various lesions of hard dental tissues. Abrasion, enamel grinding, erosion, granuloma, cement hyperplasia.
- Item K04. Damage to the pulp and periapical tissues. Pulpitis, pulp degeneration and gangrene, secondary dentin, periodontitis (acute and chronic apical), periapical abscess with and without cavity, various cysts.
- Item K06. Pathologies of the gums and the edge of the alveolar ridge. Recession and hypertrophy, trauma to the alveolar margin and gums, epulis, atrophic ridge, various granulomas.
- Item K07. Changes in bite and various jaw anomalies. Hyperplasia and hypopalsia, macrognathia and micrognathia of the upper and lower jaws, asymmetry, prognathia, retrognathia, all types of malocclusion, torsion, diastema, trema, displacement and rotation of teeth, transposition.
Incorrect jaw closure and acquired malocclusions. Diseases of the temporomandibular joint: looseness, clicking when opening the mouth, painful dysfunction of the TMJ.
- Item K08. Functional problems with the supporting apparatus and changes in the number of teeth due to exposure to external factors. Loss of teeth due to injury, extraction or disease. Atrophy of the alveolar ridge due to long-term absence of a tooth. Pathologies of the alveolar ridge.
Let's take a closer look at section K02 Dental caries. If a patient wants to find out what entry the dentist made in the chart after treating a tooth, he needs to find the code among the subsections and study the description.
Prevention
The condition of dental tissue is greatly influenced by a person’s diet. To prevent caries, you need to follow some recommendations:
- eat less sweets and starchy foods;
- balance the diet;
- monitor vitamins;
- chew food well;
- rinse your mouth after eating;
- brush your teeth regularly and correctly;
- avoid eating cold and hot food at the same time;
- periodically inspect and sanitize the oral cavity.
The video provides additional information on the topic of the article.
Timely treatment will help you quickly and painlessly get rid of caries. Preventive measures prevent damage to the enamel. It is always better to prevent illness than to treat it.
If you find an error, please select a piece of text and press Ctrl+Enter.
Tags diagnostics caries treatment
Did you like the article? stay tuned
Previous article
A radiant smile and fresh breath from the portable irrigator B Well WI – 911
Next article
An innovative element in the composition of Biorepair toothpaste for adults and children
DIFFERENCE OF SECONDARY CARIES FROM RECURRENCE
A carious lesion under a filling (in dental practice - secondary caries ICD K02.8) is the re-formation of a lesion under a previously placed composite material. The root cause of this process is bacteriological microorganisms, filling cracks and hard tissue structures of the tooth. The diagnosis of secondary caries includes the involvement of intact enamel near the material
Recurrent caries process is the resumption of pathology in the treated area. Such relapses of the disease can be caused by a violation by a dental specialist of the protocol for treating the formed cavity: a zone of preventive expansion is not created and drug treatment is not carried out.
The occurrence of recurrent and secondary pathology can occur at the same time, and choosing a specific cause for the formation of pathology is very difficult.
SIGNS OF PATHOLOGY
Symptoms such as:
- change in shade of the entire filling material or along the edges;
- the seal is not tight (food residue gets stuck);
- enamel chips;
- reaction to changes in temperature or sweet/salty;
- unpleasant odor from the mouth;
- aching pain in a previously treated unit;
- the formation of inflammation in the adjacent gingival and mucous tissues.
If there are visible changes on the crown part of the tooth and the composite material, you must immediately make an appointment for a consultation with a dentist. A reason for concern in case of secondary caries, the reason for recording will be a change in the color shade of the filling or the formation of dark zones on the enamel. An acute painful condition is an indicator of an advanced stage of the pathological process, which means that treating such a unit will be more difficult and longer.
TREATMENT OF SECONDARY CARIES
The method of treating pathology is determined by the doctor after the necessary diagnostic measures have been carried out and takes into account the stage of the process. Currently, the following treatment methods are available in dental practice:
- Re-filling. The old filling and damaged tissue are removed. The dental cavity is treated antiseptically and an insulating lining is installed. Afterwards, a new filling material is placed.
- Microprosthetics. The technique is high-tech and consists of installing specialized ceramic overlays. They correspond in parameters and shade to the crown part of the tooth.
- Prosthetics with a crown. The decision to use crowns is made taking into account the solid tooth root and the absence of the possibility of using other techniques. To install a crown, pulp removal may be necessary.
- Unit extraction. If the carious process under the filling is severely advanced and affects the subgingival part of the unit, including the root, then the doctor may decide to remove the tooth. Surgery to extract a unit is performed only as a last resort, if it is impossible to save the tooth.
Complications
Untimely or improper treatment of caries leads to complications in the form of diseases such as pulpitis and/or periodontitis, which in turn can lead to the development of purulent-inflammatory processes in the maxillofacial system and complete loss of teeth.
In addition, the lack of treatment, as well as the removal of teeth completely affected by caries, cause secondary deformation of the dentition and pathology of the temporomandibular joint. Indicators of the development of complications of dental caries are very significant: in the age group of 35-44 years, the need for fillings and prosthetics is 48%, for tooth extraction - 24%.3
At the same time, it is worth paying attention to the so-called iatrogenic complications, the occurrence or absence of which depends entirely on the doctor. Since the treatment of dental caries is accompanied by a very large number of medical procedures, the effectiveness and quality of the treatment depends on the level of qualifications, medical skill, quality of the instruments used, materials and other factors. Despite the rapid development of dentistry, today it is often still possible to detect errors and complications that were made during the preparation and filling of a carious cavity during the treatment the patient received earlier. These include: insufficient treatment (preparation) of the carious cavity; overheating and burns of dentin, overheating of the pulp and, as a result, its necrosis; secondary caries; inflammation of the interdental gingival papilla; apical periodontitis – acute and chronic; perforation of the bottom and stenoccarious cavity; damage to adjacent teeth and gingival margins by a dental drill; displacement, fractures or loss of fillings; overbite during filling and/or lack of contact point; applying a single filling to several carious cavities, overhanging edges of the filling; discrepancy between the color of the filling and the color of the tooth/enamel; incorrect choice of filling material and instruments. Most of the listed complications can be eliminated, but, of course, it is better to prevent this by making the right choice of dentist.
DIAGNOSTICS
At a consultation, when applying, the dentist conducts a visual and instrumental examination of the teeth and oral cavity. Also, for a more accurate assessment of the condition of all structures and differential diagnosis of pathologies, an RG image may be needed.
At the branches of the West Dental clinic in Vsevolozhsk and Yanino, you can perform targeted X-rays, orthopantomograms and CBCT scans. The radiation dose when taking pictures is very small, which makes the procedure completely harmless to the health of adults and children. X-ray examination allows you to quickly diagnose secondary caries.
Symptoms of caries on the contact surface
Symptoms of superficial damage to the contact (approximal) surface are quite scarce. They can be divided into objective (i.e. those that both the doctor and the patient see) and subjective (that only the patient feels).
Objective
The dentist will see a surface defect on which the probe will cling. The color of the enamel in the affected area can vary from cream to light or dark brown and even black. The x-ray will show a surface defect that does not extend beyond the enamel layer. In this case, a defect can also form on the adjacent tooth (“kissing” surfaces). Transillumination of the tooth with a narrow beam of light (transillumination) and targeted X-ray diagnostics help identify this form of the disease.
Subjective complaints
In addition to the aesthetic defect - a small dark spot, there may be complaints of mild, quickly passing soreness (soreness) upon contact with cold or hot (much less often), sour, sweet, and sometimes salty. The patient may indicate that food is stuck between the teeth. In some cases there are no complaints.
K02.9 Unspecified
Unspecified caries is a disease that develops not on living, but on pulpless teeth (those from which the nerve has been removed). The reasons for the formation of this form do not differ from standard factors. Typically, unspecified caries occurs at the junction of a filling and an infected tooth. Its appearance in other places of the oral cavity is observed much less frequently.
The fact that a tooth is dead does not protect it from developing caries. Teeth depend on the presence of sugar that enters the oral cavity along with food and bacteria. After the bacteria are saturated with glucose, acid begins to form, leading to the formation of plaque.
Caries of a pulpless tooth is treated according to the standard scheme. However, in this case there is no need to use anesthesia. The nerve that is responsible for pain is no longer in the tooth.