A beautiful smile is the key to the health and success of a modern person. If people smile widely and openly, then those around them are more inclined to like them. Any deficiencies and health problems immediately affect the quality of life, so the problem of cosmetic dental restoration worries many today.
With the help of dental treatment and restoration, you can put in order and restore teeth damaged by caries and other dental diseases. Correctly selected material, shape and color will help to hide any imperfections of the teeth as much as possible and restore them to their original appearance.
Restored teeth after such restoration cannot be distinguished from healthy neighboring teeth. It is prescribed in case of irregularly shaped teeth, chips, cracks and spaces between teeth, as well as after dental trauma. The restoration easily changes the length or width and aligns the dentition. Pigment spots or stains from coffee and smoking can also be removed with cosmetic restoration.
Types of modern prostheses
By level of amputation:
- cosmetic finger prostheses;
- prosthetic part of the hand;
- full hand prosthesis;
- forearm prosthesis (up to the elbow);
- shoulder prosthesis;
- prosthesis after disarticulation of the shoulder joint.
According to the method of attachment to the limb stump:
- using a silicone case and lock;
- using the anatomical shape of the receiving sleeve;
- using belts (bandage).
According to their intended purpose, there are two groups of prostheses:
- cosmetic - imitate a natural hand, hiding the defect;
- functional - make it possible to use the injured limb.
According to the mechanism of action, functional prostheses are:
- bionic (myoelectric or bioelectric);
- workers (passive);
- traction (active mechanical).
Cosmetic enamel restorations: natural biomimetic layering technique
There is no doubt that the human face is one of the components of the overall profile of external attractiveness. If we group the elements of the face by importance, the mouth, of course, occupies one of the first places: it forms both the overall facial expression and helps to display feelings of friendliness, agreement or gratitude. A smile, in turn, expresses a feeling of happiness and pleasure, but even with other emotions it has an extremely important facial meaning. In turn, a smile consists of the profile of the face, the profile of the gums, teeth and the emotion that it expresses. Therefore, to correct a smile, it is necessary to achieve harmony of these four components, also taking into account the specifics of their individuality. Lips are a kind of frame for a smile, and teeth and gums represent a picture placed in this frame. A healthy and harmonious smile has a positive impact on the development of feelings of trust and confidence in a person. Even minor defects in one of the components of a smile, such as a violation of the contour or color of the front teeth, compromise the overall aesthetic condition of a person’s face.
This article will discuss the role of hard tissue, especially enamel, in shaping the aesthetic appearance of the smile, and will present a new minimally invasive technique for creating a more youthful smile profile in compromised clinical situations with minimal biological loss.
The role of tooth enamel
Enamel is one of the most important structures of the tooth, both from a functional and aesthetic point of view. Essentially, enamel is a uniquely organized nanostructured material that forms the outer covering of teeth. It consists of crystalline calcium phosphate, which makes up 96% of the structure, with the remaining 4% being organic components and water. The organic component of enamel is a breakdown product of the main protein - amelogenin. Mature enamel does not contain cells and does not regenerate, unlike other biomineralized tissues such as bone and dentin.
Loss of enamel surface leads to deterioration of the aesthetic parameters of the smile
Enamel, covering the outer coronal surface of the tooth, must withstand a significant number of acting factors in conditions of constant demineralization and remineralization processes. In such a situation, the loss of a certain layer of the tooth surface is simply inevitable. However, this process is normal during the aging of the body, in addition to which it can also be pathological. The latter differs from the physiological one in that it is accelerated by the action of endogenous and exogenous factors.
Depending on the cause, there are four different types of tooth wear: attrition, abrasion, erosion and abfraction. Each of these processes, in addition to dysfunction and aesthetic parameters of the smile, also affects the general state of health.
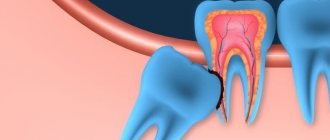
Attrition (Figure 1) is the loss of dental tissue resulting from mechanical action between the surfaces of opposing teeth during mastication and parafunctional activity. This process is most often noticeable on the occlusal surfaces of the posterior teeth and the cutting edges of the anterior teeth.
Photo 1: Attricia.
Abrasion (photo 2) refers to mechanical abrasion of teeth, provoked by reasons different from those during the interaction of antagonist teeth. Most often, this process develops when certain exogenous agents are present between the teeth, such as an overly abrasive toothbrush or paste, or during a certain method of brushing teeth.
Photo 2: Abrasia.
Erosion (photo 3a and b) is the pathological wear of teeth caused by the action of chemicals, most often acids of internal or external origin. The rate of erosion progression is also influenced by the quality of saliva (rate of salivation, pH and saliva components).
Photo 3a,b: Erosion.
Abfraction (photo 4) is a pathological process of loss of a layer of the surface of the teeth, which occurs when teeth are repeatedly compressed and bent under the influence of occlusal loads, resulting in the destruction of enamel rods. This process is most noticeable in the area of the tooth neck.
Photo 4: Abfraction.
In addition to these four reasons, the loss of hard tooth tissue can be provoked by developmental anomalies (photo 5a-c), especially amelogenesis imperfecta and dentinogenesis, which are predisposing factors for progressive pathological abrasion.
Photo 5a-c: Teeth with developmental defects: enamel hypoplasia (a), amelogenesis imperfecta (b), dental fluorosis (c).
The relationship between the processes is quite logical: with inadequate enamelogenesis, the tissue is very thin and soft, therefore, it wears out more easily, while with imperfect dentinogenesis, the strength of the bond between dentin and enamel is impaired, which leads to easy separation of these tissues at the interface. The loss of hard dental tissues changes their morphological shape, leads to the development of various types of sensitivity, pulpal complications, discoloration of teeth, loss of vertical parameters of occlusion and associated occlusal disorders. The latter, accordingly, provoke changes in neuromuscular function, chewing efficiency and smile aesthetics due to an imbalance in the horizontal component of the occlusal plane. Loss of the canine route of insertion increases the load on the posterior group of teeth, which consequently causes progressive wear of the molars and an increased risk of chipping of restorations in this area. An unstable state of occlusion, among other things, also provokes biting of the cheeks and tongue during chewing.
Optical characteristics of anterior teeth
As mentioned earlier, teeth undergo changes over the years that directly affect their appearance and color. Due to an increase in the thickness of dentin and a decrease in the thickness of enamel, the parameters of transparency and opacity of teeth also change, which can be explained by the difference in interaction with light when the composition and level of mineralization of hard tissues are disrupted. Enamel transmits up to 70.1% of the light flux, while no more than 52.6% passes through dentin. Thus, it is clear why dentin is the main light former, and enamel is only a modifier.
Optical properties of natural enamel
When working with enamel, you need to understand the specific orientation of enamel prisms in the thickness of the fabric. As a rule, they are located at an angle of 90 degrees relative to the dentin surface. In the cervical region, the prisms depart from their usual horizontal orientation and tilt apically. In the area of the cutting edge, the prisms have an oblique direction, and in the area of the edges they are almost in a vertical position. Due to this change in the orientation of the prisms, the transparency of the enamel also decreases. Enamel also changes the chromatic parameters of teeth due to processes such as reflection, transmission and refraction of light, as well as based on the characteristics of thickness and surface texture. In addition, enamel has the ability to weaken the colors of the lower range, which also affects the chromatic parameters of the tooth. The light reflectance or transmission properties of enamel depend on its texture, the orientation of the enamel prisms and the ability to refract light depending on histological characteristics. Enamel translucency may also be associated with variations in calcification levels, as more porous and less mineralized enamel has higher levels of light dispersion.
Optical properties of dentin
Dentin can be considered as dental tissue that largely determines the overall shade of the tooth. From an optical point of view, dentin is a structure with low transparency and varying parameters of intensity and color saturation. Dentin is relatively opaque because the arrangement of the dentinal tubules allows dentin to exhibit selective diffraction of light, causing some rays to be reflected while others are absorbed. During the development of the organism, primary dentin is replaced by secondary and tertiary dentin, which are characterized by a different structure and composition, and, consequently, other optical characteristics. In elderly patients, a decrease in the diameter of the dentinal tubules causes progressive dentin sclerosis and high color saturation of this structure.
Basic characteristics of teeth
The visual characteristics of teeth change with age and can be categorized into four age groups: childhood, adolescence, middle age and old age.
In childhood (photo 6a-c)
Photo 6a-c: View of teeth in childhood.
Around the age of 10 years, the enamel is characterized by an almost milky white hue, the surface layers are at their most opaque and often look as if they have been frostbitten. In this case, the enamel, as a rule, demonstrates a clear opalescent effect, and its surface with micro- and macrostructure has a very low surface gloss; The cutting edges of the teeth are completely covered with enamel.
In adolescence (photo 7a-c)
Photo 7a-c: View of teeth in adolescence.
Around the age of 20, the enamel becomes less white, and its transparency increases due to the abrasion of the upper layers of the young, opaque enamel. The enamel surface is still microstructured and has a low gloss level. The dentinal areas, although still covered with enamel, become slightly noticeable with a blue and orange tint.
Middle age period (photo 8a-c)
Photo 8a-c: View of teeth in middle age.
During this period, the micro- and macrostructure of the enamel surface decreases, and its surface gloss increases. The enamel becomes more transparent, and dentin shades become more pronounced.
Elderly period (photo 9a-c)
Photo 9a-c: View of teeth in older age.
The enamel is characterized by increased transparency, the shades become closer to bluish and grayish, the microstructure of the enamel is almost absent, and the macrostructure is significantly reduced. Also, at the same time, the parameters of surface gloss increase, dentin looks darker and even less transparent compared to teeth in middle age.
Restoration strategy
Understanding all the specifics of light changes and optical characteristics of enamel, which vary with age, the doctor can ensure that the most artistic and natural restoration effect is obtained. The restoration strategy includes not only the process of modeling the lost layers of tissue, but also the optimal approach to material selection, processing, texturing and polishing. Cosmetic enamel restorations can be successfully used to correct minor violations of the structure of teeth, their brightness and contour parameters. The loss of the surface layer of enamel provokes disturbances in the visual perception of the front teeth, their brightness parameters, contour and the overall aesthetic profile of the smile. Because the enamel layer is quite thin, its loss is often associated with the loss or at least exposure of a certain amount of dentin tissue. Therefore, restoring the natural appearance of enamel requires a careful analysis of the need for restoration and lost dentin tissue, which also affects the parameters of depth, color and type of restoration.
Selection of restorative materials based on optical properties
Although dentin determines the basic color of the tooth and its shade, this parameter is perceived by the observer as somewhat altered due to its modification by enamel tissues depending on its thickness, texture and level of polishing. Enamel does not actually change the shade (color) of the tooth, but only gives it more or less saturation depending on its thickness. Placing a layer of enamel of the required thickness over the dentin area increases or decreases the brightness parameters of the tooth, determining the so-called “liveness” of the restoration. When simultaneously restoring both enamel and dentin tissues, it is necessary to take into account the difference in color transmission by these structures: therefore, more opaque composites must be used for the dentin portion of the restoration, and more transparent shades must be used for the enamel. Considering that a huge amount of restoration materials with different shades of color and transparency parameters are produced all over the world, a systematization of these materials depending on their optical characteristics was proposed (Table 1).
Table 1: Material category.
| Material category | Target | Example |
| Opaque group | To mask discolorations | Beautyfil Opaquer |
| Dentin group | ||
| Opaque dentin | To replace deep dentin layers | Beautifil II A20 (Opaque dentin) |
| Normal dentin | To replace the outer layers of dentin | Beautifil II A2 (universal dentin) |
| Enamel group | ||
| Transparent | For enamel replacement | Beautifil II Enamel HVT |
| Effect group (dyes) | To create specific effects | Beautyfil II Gum shade |
Smile style and surface texture design
The technique of natural-mimetic restorations is consistent with the general psychology of the patient’s perception, as described in the Smile Wheel concept. The design of the smile and the texture of the surface of the teeth should be chosen in accordance with the specific perception of the patient, his individual wishes and vision of treatment results. However, this approach requires a deep understanding of the patient’s personality in order to adequately interpret his subjective aspects. To analyze human personality, the author of the article uses the “DISC” principle, developed by William Moulton Marston, and presented by him in his publication “The Emotions of Normal People” in 1928. Marston proposed that people are motivated by four internal drives that drive his personality images. To describe the processes, he used four behavioral tendencies, which he defined by four letters of the alphabet: D-domination (dominance), I-influence (influence), S-steadiness (stability) and C-compliance (compliance).
D-Smile Style
I-Smile Style
S-Smile Style
C-Smile Style
Based on DISC personality traits, the author classifies smiles into four categories according to Tables 2 and 3.
Table 2: DISCover smile design - dental characteristics.
| Smile design | Central incisors | Tops of fangs | Lateral incisors | IAL (esthetic cutting edge line) | Angle IAL | Tooth axis |
| Smile Design D | Lack of dominance with a square shape | Flat type | Flat and can touch the esthetic incisal line (IAL) | Direct or R = reverse | 90° and more | Straight or slightly deviated |
| Smile Design I | Dominant type with rectangular shape | Rounded flat | Rounded and flat cutting edges that do not touch the aesthetic cutting edge line (IAL) | Descending to direct type | 85-90° | Straight |
| Smile Design | Dominant type with oval shape | Rounded | Delicate, rounded mesial and distal incisal edges that do not touch the esthetic incisal line (IAL) | Descending type | 75-85° | Slightly convertible |
| Smile Design C | Dominant type with triangular shape | Spot | Rounded distal and flat mesial cutting edges that touch the IAL | Descending type | 70-80 ° | Convertible |
Table 3: DISCover smile design: personality characteristics.
| Smile design | Personality characteristics | Suitable for |
| Smile Design D | Goal-oriented, competitive, direct, extroverted, driven by desire, ambitious, strong willed: “Just do it.” | Entrepreneurs, salespeople, legal or judicial professions, managers and related professions |
| Smile Design I | Human and personality oriented, talkative, spontaneous, enthusiastic, persuasive personality type: “Have fun.” | Marketing, public relations, training, tourism, retail and related professions |
| Smile Design | Stable, reliable, conservative, loyal, relaxed, passive, patient type: “Do everything together.” | Training, Education, Finance, Economics, Human Resources, Help Desk, Customer Service, Manufacturing, etc. |
| Smile Design C | Cautious, detail-oriented, logical, organized, diplomatic, "do it right" type. | Accounting, auditing, engineering, medicine, research and development, agriculture, computer programming, etc. |
To achieve optimal restoration parameters, the doctor should always take into account age-related variations in the enamel surface. With age, patients experience a thinning of the covering structure of the tooth, but its modeling should still be carried out taking into account the individual wishes of the patient.
The surface texture of a tooth is determined by three factors:
- Surface texture or degree of surface smoothness/roughness. This parameter can be divided into two categories.
- Macrotexture (vertical and/or horizontal projections and depressions, ridges and grooves visible on the surface of the tooth) and microtexture (small surface irregularities associated with the approximation and calcification of the enamel matrix during tooth formation, depressions, vertical lines and perikymata).
- The gloss or degree of shine of a tooth, also known as simply shine (photos 10 and 11). Luster determines the amount of light reflected on the surface of the crown. This parameter is no less important than the color and contour of the future restoration. It should be noted that shine is not related to age and is genetically or congenitally determined.
Photo 10: Macrotexture with low gloss value.
Photo 11: Microtexture with high gloss value.
Naturo-mimetic layering technique (restoration) (NLT)
Given the complex structure of natural teeth, it is quite difficult to replicate it by simulating the parameters of enamel and dentin. When implementing an NLT protocol, it is important to conduct a detailed analysis of the color, opacity, translucency, texture, surface gloss and special characteristics of teeth to be restored in the future. During NLT restoration, the desired result is achieved by applying the correct thickness of transparent or translucent enamel group materials over a saturated and opaque dentin replacement composite. There are various clinical situations in which it is necessary to achieve the effect of enamel rejuvenation, treatment for which is carried out differently depending on the type of tooth defect and the patient’s wishes regarding restoration. Depending on the clinical situation, the clinician should choose one of the above NLT methods. The natural mimetic layering technique is based on a new classification of shade layers and is divided into the following clinical algorithms.
NLT monolayer
With this technique, the defect is restored with one layer of composite. Typically, opaque shades or materials designed to simulate optical effects are not used in such situations. However, in any case, it is necessary to take into account the parameters of the required restoration layer. The higher color of the area and its opacity justifies the use of a thicker layer. On the other hand, using an enamel shade that is too transparent can cause a gray effect in the restoration, which can again be corrected by the thickness of the layer of material used. At the same time, by increasing the thickness of the dentin material layer, we simultaneously influence the parameters of shade and color intensity, and, therefore, we need to look for a suitable compromise for maximum imitation of natural tooth tissue (photo 13).
Photo 12: NLT monolayer technique.
Photo 13: NLT two-layer technique.
NLT three-layer technique
This technique is used for teeth that require significant color modification, such as when restoring non-vital teeth. The method involves the application of opaque materials, which do not need to be covered with composites intended to form optical effects. As a rule, the opaque group of materials with a three-layer technique is covered with dentin and enamel shades, imitating natural tooth tissue (photo 14).
Photo 14: NLT three-layer technique.
NLT-comprehensive layering technique
Any restoration that requires the use of a group of materials designed to create optical effects is complex. And it doesn’t matter whether it is made only with such materials, or in combination with opaque analogues, or enamel-dentin-substituting composites. Therefore, the technique can be called mono-complex, two-complex or tri-complex. The use of a composite to create a specific effect (to create opalescence, orange or yellow tints, stains, enamel cracks, white spots, etc.) must be justified by the results of careful color analysis and mapping of the tooth surface. This type of restoration is mainly used in the incisal area of the tooth, where the range of translucency and opalescence increases significantly (photo 15-17).
Photo 15: NLT monocomplex technique.
Photo 16: NLT-two-complex technique.
Photo 17: NLT - three-complex technique.
The level of polishing (smoothness) of the surface changes the indicators of chromatic perception, and this parameter is inversely proportional to the lightness of the restoration. The more a surface is polished, the greater its light transmission becomes and, consequently, the brightness decreases. In turn, the absence of polishing (matte finish or the presence of a more pronounced microstructure) leads to a more reflective surface and a brighter restoration.
Photo 18: Naturo-mimetic layering technique (NLT): step-by-step algorithm.
Conclusion
Cosmetic dentistry is one of the fastest-growing branches of dentistry, advancing in tandem with greater awareness and improved patient well-being. After all, everyone wants to have a beautiful, stylish and healthy smile. An aesthetic smile today is the main criterion for patients, indicating that their treatment was successful and in accordance with their own wishes.
Author: Dr Sushil Koirala, Nepal
Bionic prostheses
The most advanced prostheses, as close as possible to the action of the human hand. To operate, they use an external energy source (rechargeable batteries), are equipped with electric motors and are controlled by electrical signals from the patient’s body. Myoelectric prostheses respond to muscle contraction. Changes in the electrical potential are detected by EMG sensors in the prosthetic socket. They transmit a signal to the microprocessor of the artificial hand, and the prosthesis performs a certain action.
Note!
- Conventional bioelectric prostheses make grip a breeze. This is the basic movement, but it is not always enough.
- Highly functional prosthetics can accommodate a variety of grips. For this, two myodensors are used that sense the activity of the two largest muscles of the arm. To select the desired gesture, the patient sends the prosthesis several sequentially repeated commands - they serve to switch modes by brute force. After training, the prosthesis becomes a real extension of the hand; the person uses it instinctively, performing different types of grips without thinking.
Bionic hand prostheses improve the quality of life of patients. People become able to perform complex activities such as drawing, working with a keyboard, tying shoelaces, cooking and many others. The latest generation of bionic prostheses are capable of performing finger movements. For example, the Touch Bionic hand from Ossur performs functionality close to the actions of a real hand, since each finger is equipped with a separate electric motor. The patient can choose from twelve hand grip options. Your prosthetic technician can help you determine your individual reaction speed and grip strength. This allows you to comfortably work even with very fragile objects, for example, taking a chicken egg.
Pros:
innovative technological appearance, use for all main types of household activities.
Minuses:
high cost, unnatural appearance.
Dangers of toothless life
Which of us is unfamiliar with the expression “eats so much that it’s cracking behind the ears”? But a person with partial or complete loss of teeth can hardly boast of “crackling sounds behind the ears” while eating. He has to exclude hard food from his diet, or swallow it after barely chewing it. And as you know, food, when crushed, begins to be digested in the mouth, but with large pieces the stomach will have to cope with triple strength. The already mentioned “crackling behind the ears” is due to the fact that the salivary glands are located in the parotid region. It is they who produce the production of a very important hormone that is involved in the regulation of calcium metabolism; in addition, it affects the blood coagulation and anticoagulation systems, the metabolic processes of the liver, stomach and other vital organs. With partial or complete absence of teeth, chewing movements of the lower jaw are limited, which invariably leads to dysfunction of the salivary glands. This is where changes in the composition of the blood and sudden gastric and liver dysfunctions appear. And a violation of calcium metabolism in the body, among other things, will undoubtedly have a negative “echo” on the remaining teeth. In addition, a person who is missing one or more teeth suffers from the inability to smile broadly, laugh, or conduct a normal conversation, which can negatively affect his communication with others and lead to stress. If this happens, the conclusion is clear - dental prosthetics is simply necessary for a person to continue a normal life.
Working dentures
A working prosthesis is not at all like a regular hand. It is equipped with an adapter for installing various attachments, which allows you to actively use the upper limb for work. Attachments for writing, cutlery, drawing, printing, and sewing can be attached to the prosthesis. There are grips for hammers, keys, scissors and other tools.
Pros:
inexpensive design, great functionality.
Minuses:
unnatural appearance, the need to purchase attachments for each type of activity and change them during work.
Teeth on a plate
Complete removable plate dentures
Modern plate prostheses have not changed much structurally, but have stepped far forward in aesthetics.
The base plate is now not just pink, but with introduced capillary vessels, which creates a very natural appearance of the mucous membrane, and artificial teeth, made using modern technologies, have an excellent appearance and high wear resistance. All this contributes to achieving an individual aesthetic effect and reliability of the prosthesis design. A complete plate denture is the only option to replace all lost teeth (if you do not take into account dental implantation). It is held in the mouth by the suction effect and the anatomical features of the jaws. There is one nuance here - the difference between holding the denture on the upper and lower jaw. The large support area, hard palate and structure of the upper jaw contribute to good fixation of the prosthesis. The same cannot be said about the lower jaw. A small support area, a large number of movable and elastic frenulums and folds do not allow the prosthesis to adhere normally. And the very “glib” language makes this task even more difficult to accomplish. For the toothless lower jaw, the patient can be offered a so-called “floating” removable denture, which will float and not sit tightly in place. It takes a long time to get used to it, but to speed up the process, special fixing creams are used. “Pleasure” is, of course, not very pleasant, so you shouldn’t bring it closer. In the lower jaw, you have to fight for every tooth. Fixation of the prosthesis is always better when there is support. A partial plate denture
is used when one or more teeth are missing. It is made entirely of plastic, with the exception of metal clasps (hooks). The prosthesis is light and cheap, it does not take up much space in the mouth, and rests entirely on the gum. It can be simply irreplaceable for temporary prosthetics.
Active mechanical prostheses
Active (or “traction”) - allow the artificial hand to compress, due to traction, to hold various objects. The action occurs using mechanical traction (when the opposite shoulder moves, the cable is tightened or loosened). A simple and reliable mechanism allows you to control the strength and speed of your grip.
With enough practice, a person masters fairly subtle movements: he can write with a pen, use cutlery, type, carry a bag, light matches.
Traction prostheses can be installed in children from 8 years of age. Constant training of the muscles of the shoulder and forearm subsequently helps to form a stump and quickly get used to a more advanced bionic prosthesis.
Pros:
simple mechanism, easy to maintain, precise movements when performing some delicate work.
Minuses:
the use of a traction band (can rub), the need to be careful with the prosthesis shell and periodically replace it.
Your new smile is our concern
For prosthetics, specialists from the CELT Dentistry Department use ultra-thin imported ceramics, which allows for maximum preservation of tooth tissue, as well as removable dentures with invisible micro-locks. In case of complete or partial absence of teeth, frameless ceramic, metal-ceramic and solid-cast crowns are made. Fixed (bridge) and removable (clasp and plate) prostheses are performed. We can prepare for prosthetics, remove the nerve and fill the canal. If necessary, X-rays can be taken in our Center, in the radiology department, which will allow you to significantly save time. All crowns are selected exactly to match the color of real teeth, for which we have a special color shade scale at our disposal. The department also has its own dental laboratory, equipped with the latest equipment (6 highly qualified dental technicians on staff), which allows us to produce crowns or dentures in a fairly short time, thereby saving your time. Come! You will leave us smiling broadly!
Cosmetic dentures
A cosmetic prosthesis is as close as possible to the natural appearance of a real hand, but is completely non-functional. You won’t be able to do anything complicated with it (for example, buttoning a jacket). The prosthesis consists of four parts: a stump, a supporting socket, a hand frame and a shell (glove). The shell is made of PVC or silicone, matching the patient's skin tone. For greater reliability, images of moles, veins, folds, and palm lines can be applied. It is possible to make a prosthesis with acrylic nails that are as close as possible to real ones.
Pros:
relatively low price, imitates a healthy hand, the hand looks natural - does not attract the attention of others.
Minuses:
the inability to perform any actions, the need to take care of the prosthesis shell and periodically replace it.
Don't be afraid to “put your teeth on the shelf”
Removable prosthetics
- Cost: 33,000 rub.
More details
Dental prosthetics makes it possible to restore teeth that have been removed or lost as a result of illness or injury. Modern dentistry and new technologies for dental prosthetics make it possible to quickly and accurately select the required size, shape and color of new teeth to achieve a high cosmetic effect. Nowadays, dental prosthetics is no longer a long and painful process. Modern removable dentures are fundamentally different from the old ones that our grandparents used. The differences between modern prostheses are new, durable, flexible and safe materials, as well as high technologies that allow us to produce the most suitable prosthesis with maximum precision. There are several methods for restoring lost teeth and normalizing chewing function, that is, normal chewing of food. In this article we will talk about one of the types of dental prosthetics - removable dentures. Such dentures are divided into complete removable and partially removable. They can be lamellar or clasp. Despite the prejudices of many people, removable dentures remain the most common type of prosthetics today, since this method is accessible to most and has the fewest contraindications.
Manufacturing of removable dentures
Prosthetics with various types of dentures has been used in clinical practice for decades, so dentistry has a well-functioning production mechanism.
Stages of manufacturing a partial removable denture
- Initial consultation, examination of the oral cavity and selection of orthopedic design.
- Taking impressions and producing a wax model in the laboratory.
- Grinding and correction of the finished structure.
- Finishing the structure in the articulator and trying on the wax structure by the patient.
Although the production of a partial denture takes on average 2 weeks, the adjustment period can last up to a month. At this time, the patient may feel some discomfort, but if the prosthesis causes significant pain and discomfort, it is worth contacting a specialist for correction or replacement of the structure.