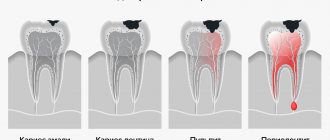
What is tooth luxation
Tooth dislocation is a traumatic injury, which is characterized by displacement of the crown and rupture of the ligamentous apparatus (periodontal). Such damage can occur in childhood and adulthood. Dental services include providing qualified assistance for any dental injuries.
Why do dislocations occur:
- Mechanical injury: if there is a blow or fall from a height.
- Eating too hard foods (fruit seeds, berries).
- Having bad habits: chewing pens, pencils, nut shells.
- Rough removal, resulting in injury to neighbors.
Diagnostics
An experienced doctor can detect a tooth dislocation with a simple examination. At the same time, he pays attention to the location of the dental crown and the characteristics of the damaged gum. However, there are cases when damage and deformation of the teeth may not be noticeable externally and, until subsequent symptoms appear, the dislocation may go unnoticed. This, in turn, will complicate further treatment.
To avoid such situations, it is important to additionally take x-rays of the teeth and jaw during the examination. It will not only confirm or refute the presence of a dislocation, but will also identify possible damage to the jaw or internal tooth tissues. This approach will allow you to choose the most effective treatment and make it possible to save the tooth itself.
Types of tooth dislocations
- Incomplete – there is a displacement of the coronal part, the surrounding gums are swollen, and there is redness.
- Complete dislocation - the tooth is missing in the socket. Bleeding gums and ruptures of the mucous membrane are observed.
- Impacted - the tooth is shorter than the rest or completely “hidden” behind the gum. Swelling and red gums.
The most common luxation of the front tooth occurs. In children, injuries occur much more often. The danger of childhood injuries to the oral cavity is that under the milk there is a rudiment of a permanent one. As a result: the permanent one will erupt in a modified form, or will not erupt at all.
Varieties
This disease is classified into:
- complete;
- incomplete.
In the first case, the disease forms after an absolute rupture of periodontal tissues and the circular ligament of the tooth due to a strong blow to the crown. Often there is damage to the upper jaw of the front teeth.
A complete dislocation clinically looks like this: upon examination, you can see that the tooth is missing from the dentition, and its socket is filled with a fresh blood clot and continues to bleed. Often there are concomitant injuries to the soft tissues of the lips - wounds to the mucous membrane, bruises, and so on. In order for the treatment to be complete and effective, the condition is assessed, namely the presence of carious cavities, the integrity of the root and crown, etc.
Incomplete luxation changes the position of the tooth in the row. The patient complains of mobility, pain, changes in his position and impaired chewing function. An examination of the oral cavity shows the displacement of the crown of the injured tooth in different positions. It can be highly mobile and very painful upon percussion, however, it is in its place in the dentition.
In this case, the gums are hyperemic and swollen, and ruptures may occur. Due to rupture of periodontal tissue, the circular ligament and damage to the walls of the alveoli, pathological dentogingival pockets can form, as well as bleeding from there. In the case of dislocation and oral displacement, its root is usually displaced vestibularly and vice versa. Often the patient has concomitant injuries - wounds, hemorrhages, bruises.
Symptoms of tooth dislocation
Symptoms of incomplete dislocation: pain while eating, red swollen gums, bruising. There is a displacement of the coronal part. Possible enamel chips or cracks.
When full:
- a bleeding hole is visible;
- the patient complains of severe pain, bleeding, swelling;
- with injuries in the frontal area, difficulties in pronouncing certain sounds are observed.
Complaints when injected:
- severe pain, especially when closing and eating;
- slight bleeding from the gums;
- swelling of surrounding tissues;
- the coronal part is shortened or completely hidden under the gum.
An orthopantomogram of the teeth - an x-ray examination of the jaws, where bone tissue and roots are visible - helps to establish a diagnosis and choose the right treatment tactics. It is often prescribed in childhood.
Acute dental trauma. Classification. Terminology. Diagnostics
N.V. Gnali MD, Professor, Head of the Department of Pediatric Dentistry, SSMA, Chief Physician of the MAXIMA Dental Clinic
D. V. Rogatskin , radiologist, ORTOS LLC
The main purpose of clinical classification, in addition to systematizing knowledge, is to help the doctor make a diagnosis, plan treatment, and predict results. Assessing the existing classifications of acute dental trauma (hereinafter referred to as ADT), one can note two trends in their compilation: the first is the desire to describe all types of ADT, the condition of the pulp, periodontium, possible complications, the second is the desire to simplify the classification by including the most common injuries.
The format of the article does not allow us to present the mentioned classifications in full; we will limit ourselves to only a few comments. The disadvantage of the classification proposed by the Bulgarian authors Sl. Davydov and Z. Peneva (1964), in our opinion, is the inclusion of a section “Traumatic periodontitis” in it, which does not correspond to the generally accepted classification of periodontitis, which distinguishes acute, chronic periodontitis and chronic periodontitis in the acute stage.
The term “traumatic” indicates only the cause of periodontitis, and not its course. The nosological forms introduced by the authors: “Loosening of teeth without dislocation”, “Rupture of the neurovascular bundle without loosening of teeth” are not types of injury, but its consequences.
In the classification developed by V.F. Vasilevskaya (1970), types of crown fractures in the area of enamel and dentin are distinguished based on the transillumination of the pulp, which seems to us rather arbitrary due to the same treatment for this pathology. In our opinion, it is inappropriate to introduce into the “Combined trauma” section simultaneous, but different in form, injuries to two or three teeth of one patient. In addition, the classification does not take into account all types of combined tooth damage.
It is extremely difficult to use in practice the classifications proposed by G. M. Ivashchenko (1963) and A. M. Konstantinov (1985), due to the unsystematic and incomplete listing of nosological forms of injuries. Thus, G. M. Ivashchenko did not include in the working classification the definition of the type and level of the tooth fracture line, which is necessary to know when planning treatment. A. M. Konstantinov uses not a clinical, but a metric assessment of damage - “Fracture of 1/3 or 2/3 crown.”
This is quite difficult to determine due to the different size, shape and location of the broken part; in addition, this information is not decisive when planning treatment. It is unacceptable, in our opinion, to distinguish between “complicated” and “uncomplicated” root fractures, since this involves combining the injury as such with its consequences.
One of the latest is the classification developed by V.V. Roginsky (1987). In our opinion, there is no reason to complicate the classification by indicating the degree of formation of the root of the injured tooth. You should also not include tooth contusion in the classification as a nosological form, since it is impossible to diagnose it on the basis of the signs proposed by the author.
Pulp necrosis, identified by the author (class I-II, type 3), is a consequence of trauma, and not a nosological form.
In our country, the best known classification is N.M. Chuprynina, published in the latest edition in 1993 (Chuprynina N.M., Volozhin A.I., Ginali N.V. Dental trauma, 1993). In this classification, in particular, dislocations with displacement of a tooth towards the adjacent one and rotation of the tooth along the axis are considered separately.
In our opinion, a tooth physically cannot rotate along its axis, much less move towards the adjacent one, without preliminary extrusion, which in this classification is also considered as an independent form of dislocation. In addition, there is the author’s interpretation of the concepts of “combined” and “combined” trauma, which contradicts general medical concepts in this area. And finally, the category “trauma of the germ” is highlighted.
Since the germ is not a full-fledged tooth and cannot be directly injured, consideration of this nosology in the classification of acute dental trauma is unjustified.
The WHO classification is known, which identifies 8 classes of HTA:
- Class 1: Tooth contusion with minor structural damage.
- Class 2. Uncomplicated fracture of the tooth crown.
- Class 3. Complicated fracture of the tooth crown.
- Class 4. Complete fracture of the tooth crown.
- Class 5. Coronal-root longitudinal fracture.
- Class 6. Tooth root fracture.
- Class 7. Tooth dislocation (incomplete).
- Class 8. Complete tooth dislocation.
The classification created by Jacobsen (1981) is simple and accessible to practitioners. However, the classification of Andreason et all (Andreason JO, Andreason F., Andreason L., Textbook and Color Atlas of the Traumatic Injuries to the Teeth, 2007) is most widespread abroad:
- Crown fracture.
- Fracture within the enamel.
- Fracture within enamel and dentin.
- A simple crown-root fracture within the dentine enamel and cementum.
- Fracture within the enamel, dentin and pulp (Fig. 1).
- Complete coronocoronal fracture within the enamel, dentin, pulp and cementum (Fig. 2).
Rice. 1. CT, visualization of tooth 11, MPR; fracture within the enamel, dentin and pulp.
Rice. 2. CT, visualization of tooth 22, sagittal reformat and volumetric rendering; Complete coronal-coronal fracture within the enamel, dentin, pulp and cementum.
- Root fracture.
- Root fracture within cementum, dentin and pulp (Fig. 3).
Rice. 3. CT, visualization of tooth 21, MPR; root fracture within the cementum, dentin and pulp.
- Damage to periodontal tissue.
- Injury.
- Subluxation (subluxation).
- Dislocation with displacement (lateral luxation, Fig. 4, 5).
- Intrusion (impacted dislocation).
- Extrusion (dislocation with extension from the socket, Fig. 6).
- Complete dislocation (avulsion, Fig. 4).
Rice. 4. CT, visualization of tooth 21, MPR; dislocation with displacement (lateral luxation) of tooth 21, complete dislocation (avulsion) of tooth 22.
Rice. 5. CT, visualization of tooth 21, MPR; dislocation with displacement (lateral luxation) of a fragment of tooth 21 (sagittal reformat) and tooth 11 (coronal reformat), fracture of the alveolar process in the area of the alveolar part of the palatal cortical plate (axial reformat).
Rice. 6. CT, visualization of tooth 42, MPR; dislocation with displacement, extrusion (dislocation with extension from the socket).
- Damage to pulp and periodontal tissue.
- Long-term result: a tooth with non-vital pulp, but without destruction of bone tissue in the periapical area (Fig. 7).
Rice. 7. CT, visualization of tooth 23, MPR; trauma three years ago, obliteration of the middle and apical third of the root.
In recent years, dentistry as a science and applied branch of medicine has been actively developing, new technologies are being introduced into everyday practice, and world experience is being adopted. In this regard, it seems possible for us to recommend the Andreason classification and international terminology for use in our country. Below is a list and transcription of terms used in foreign literature when describing conditions associated with dental trauma.
- Fracture (fractura) - fracture.
- Subluxation - mobility without displacement, subluxation.
- Luxation is a dislocation of a tooth or displacement of a tooth fragment.
- Lateral luxation is a lateral displacement with fracture of the socket wall.
- Extrusion - extension from the hole.
- Intrusion - impacting, impacted dislocation (Fig. 8).
- Avulsion - “full luxation”, complete dislocation with tooth extraction.
- Contusion is a bruise of soft tissues.
- Abrasion - abrasion.
- Laceration (laceration) - rupture, dissection.
- Incision - incision, cut.
- Penetration - injury by a small object with its fixation in the tissues.
- Malformation is a developmental defect characterized by a change in shape and structure; violation of morphogenesis.
- Dilaceration - curvature of the root at a large angle or curvature of the crown relative to the root (Fig. 9).
- Inflamation - literally “fire”, inflammation, acute inflammation.
- Exacerbation - literally “outrage”, exacerbation of a chronic process.
Rice. 8. CT visualization of the coronal part of tooth 11 in a state of intrusion, an adult patient with a history of trauma to the primary incisor in childhood.
Rice. 9. CT visualization of rudiment 11, condition after trauma of primary incisors; after avulsion of the incisors, the tooth germ 11 develops in a state of dilaceration; the injury provoked the development of a follicular cyst from germ 11.
A dental therapist examines a patient with dental trauma. He also treats the patient, if necessary, involving a surgeon, orthodontist, or orthopedist. The examination consists of clarifying the victim’s complaints, medical history (questioning), determining the general condition of the patient and the condition of the periodontium in the area of the injured tooth, analyzing the data obtained, establishing a diagnosis and developing a treatment plan.
Until recently, radiodiagnosis (x-ray diagnostics) in dentistry was considered an additional research method, however, when examining injured teeth, this type of research has always been necessary and relevant. Therefore, with regard to dental trauma, we can say that radiodiagnostic testing is mandatory in all cases of trauma.
The maximum information about the condition and position of the injured tooth, as well as the degree of damage to the surrounding bone tissue, is provided by computed tomography (CT), performed on a specialized maxillofacial tomograph with cone beam collimation.
Research using spiral and sequential computed tomographs is extremely rarely used in dentistry, especially in pediatric practice, due to the high radiation exposure and low resolution of image receivers. However, cone beam CT scans with a single planar sensor are designed specifically for examining the maxillofacial region.
Devices of this class provide high image quality, and the radiation dose is only 30-60 microsieverts (0.03-0.06 mSv, which is 2-3 times less than, for example, with conventional radiography of the paranasal sinuses), therefore this method has no direct contraindications for use in pediatric dentistry.
If it is not possible to make a computed tomogram, it is necessary to perform polypositional intraoral radiography. Depending on the sector the tooth belongs to, intraoral photographs are taken in direct (orthoradial) and oblique (eccentric) projections.
It should not be forgotten that, firstly, the study is carried out in cases of severe pain, changes in the configuration of the tissues surrounding the tooth and, in many cases, contamination of the surrounding mucous membrane with blood.
Secondly, to avoid projection distortion when photographing single-rooted teeth, it is necessary to position the image receiver parallel to the vertical axis of the tooth being examined. In this regard, we recommend carrying out the most non-contact and apodactyl positioning with a parallel position of the tooth axis relative to the plane of the sensor or film (orthogonal projection).
When working with a radiovisiograph, this is easily done using a standard positioner. If film is used during the study, it must be fixed in a film-fixer or held by the edge of the cover with a mosquito-type clamp.
In case of combined trauma, panoramic tomography of the dentition (orthopantomography) is performed, however, in case of isolated damage to one or more teeth in the frontal region, this research method should be considered uninformative.
Initially, it is necessary to determine the quality of the radiograph: contrast, sharpness, projection distortions (lengthening, shortening of teeth). The image should be decrypted taking into account these data or a new image should be taken, avoiding previous mistakes.
An analysis of the shadow of the tooth should be carried out, paying attention to the outlines of the crown and root of the tooth, the presence of a cavity in the crown, a filling, and its defects (overhanging edges, loose fit to the walls of the cavity). When studying the image, the size, shape, location of the tooth cavity, the presence of a denticle or intracanal granuloma in it, the location and size of the canal mouths are revealed.
The condition of the root is determined from the radiograph: length, shape, contours, canal width, size of the apical foramen, which characterize the degree of root formation and reveal physiological or pathological root resorption. It is necessary to pay attention to the state of the space of the periodontal ligament and the closing hard plate of the alveolus (lamina dura), monitor its integrity, configuration and compliance with the anatomical shape.
It is necessary to evaluate the condition of the bone tissue surrounding the tooth, the outlines of the apexes of the interdental septa, their relationship with the enamel-cement border, integrity, extent, evaluate the configuration of the bone pattern, identify the presence of pathological changes and determine their nature. Radiation diagnostics are carried out immediately at the time of treatment, several months later, and also, in some cases, a day after the injury.
Repeated identical radiographs of the injured tooth, taken at various intervals, are necessary not only for dynamic monitoring of reparative processes, but also to clarify the diagnosis. This is due to the fact that immediately after the injury (several hours), if there is no significant mobility or change in the position of the coronal part of the tooth, the fracture line may not be visualized. Over time, the fragment shifts, associated with increased swelling of the surrounding tissues and mechanical impact on the crown during chewing, the gap between the fragments widens and becomes clearly visible on the image (Fig. 10).
Rice. 10. Intraoral photographs of tooth 21: a - an hour after the injury, b - a day later.
Despite the rapid development of technology and improvement of treatment methods, acute dental trauma still remains a pressing problem in dentistry. It is almost impossible to foresee or take any measures to prevent situations that provoke dental injury. In this regard, the prognosis in the treatment of OTD largely depends on a timely and correct diagnosis, on the basis of which the optimal treatment method will be selected.
What to do if a tooth is dislocated
If you have any injury, you should immediately make an appointment with a doctor. If a tooth falls out, you should save it and bring it to the clinic. Apply a clean gauze pad to the wound site for 10 minutes. This will help stop the bleeding.
If the pain is severe, you will need to take a painkiller. You should not take more than 2-3 tablets, as this will negatively affect the administration of anesthesia in the doctor's office. In case of an overdose of painkillers, local anesthesia (injection into the gum) may have a worse effect.
It is also recommended to avoid eating hard foods, as well as too cold, hot, or spicy foods. The rest of the recommendations will be given by the dentist after examination and diagnosis.
Treatment of dislocated teeth
Traumatic tooth dislocation must be treated in a dental clinic. The doctor conducts an examination, clarifies complaints, and prescribes diagnostics. After this, treatment is prescribed.
Incomplete tooth dislocation requires fixation with wire splints. Such structures can remain in the mouth for several months. An orthopedic dentist installs a splint. Painkillers and anti-inflammatory drugs are prescribed. A gentle diet is required. Often, nerve removal and subsequent root canal filling are required. Splinting teeth in case of dislocation helps to avoid removal and other complications.
In case of complete dislocation, tooth reposition is sometimes used - its return to the socket. Regular monitoring of the patient's well-being is required. In other cases, implantation or production of prostheses (bridge or removable denture, depending on the clinical situation) is used.
Therapy for impacted nerves: removal of the nerve, splinting, diet. This form of injury is considered the most unfavorable.
An x-ray control is required: a repeat image after a few months to exclude inflammatory periodontal diseases.
Additional treatments
Drug therapy
- When carrying out manipulations to reposition a tooth after dislocation, local anesthesia is used, for this purpose Ultracaine D-S, Ultracaine D-S Forte, Cytokartin, Septanest, Bupivacaine are used. But the effect of the anesthetic stops after some time, so painkillers from the NSAID group are prescribed: ibuprofen, nimesulide, ketorolac, dexketoprofen. Children are prescribed ibuprofen and paracetamol.
- To improve the condition of the gums after injury, use: Dentol Gel - has a local anesthetic effect.
- Gel Metrogyl Denta - contains two antibacterial components, eliminates inflammation.
- Kamistad gel is a combined drug: lidocaine has a local anesthetic effect, chamomile flower tincture produces antiseptic and anti-inflammatory effects, thymol has an antiseptic effect.
- Solcoseryl dental paste - stimulates regeneration processes in tissues, thereby shortening the healing period of wounds of the mucous membrane. The composition also includes polidocanol, a local anesthetic.
Physiotherapy
After acute phenomena have subsided, the following are used to stimulate healing processes and eliminate tissue swelling:
- UHF therapy is the effect on the body of an alternating electric field with ultra-high frequency.
- Microwave therapy – uses alternating electromagnetic oscillations of ultra-high frequencies of various ranges (centimeter, decimeter and millimeter).
- Magnetotherapy is the effect of a low-frequency magnetic field on the injured area.
- Magneto-laser therapy is a complex effect of magnetic and laser radiation.
Questions and answers
If a tooth falls out due to injury, can you put it back in place yourself at home?
This procedure should not be performed at home. Such attempts will not give the desired result, but will lead to infection. You should contact your dentist immediately. Replantation is possible only in exceptional cases. In other cases, the patient will be offered prosthetics (bridge construction) or implant installation.
What diagnostics are needed for dislocations?
The dentist prescribes a computed tomography scan of the jaws - a three-dimensional image that will show whether there is damage to the alveolar process, roots, or whether there are changes in the periodontium. Computed tomography will help determine an accurate diagnosis and choose the right treatment tactics.
What are the complications of a dislocation?
If you do not consult a dentist in time, serious consequences of this injury will occur. Among the complications are inflammatory ones: pulpitis, periodontitis, periostitis, abscess. Children often experience a stop in the development of the permanent tooth germ. To avoid these complications, you should immediately contact your dentist.
How to protect yourself from dislocations when playing sports?
For this purpose, sports protective mouth guards are manufactured. You should contact an orthopedic dentist. Mouthguards are made individually for each patient based on casts of the jaws. Therefore, they are conveniently fixed on the jaws, do not create discomfort and reliably perform their protective function.
Prevention
Prevention of tooth dislocation includes:
- Explanatory work with employees of industries associated with increased injuries. Each employee is required to comply with safety regulations, which provide for an algorithm for performing certain actions and the use of protective devices.
- Explaining to parents and children the rules for arranging playgrounds and behavior on them, familiarizing themselves with possible types of injuries and methods of providing first aid if they occur. Parents should supervise young children during play.
- Educational work among the population about the need to comply with traffic rules by drivers and pedestrians, as this is necessary not only to reduce the level of injuries, but also to save lives.
- Compliance by medical personnel with the rules for performing dental procedures.
- Avoiding bad habits: you need to use special tools to open bottles and crack nuts.
- Avoiding situations that could lead to a fight; if it does occur, during it you need to tense your masticatory muscles and keep your teeth closed: this will help avoid not only dislocation of teeth, but also a fracture of the jaw.
- Providing a high level of protection for athletes involved in traumatic sports (hockey, boxing). For this purpose, helmets with full face protection and mouth guards are used (molded, which have a ready-made shape, and molded - after heating in hot water, they take the individual shape of the teeth).