There is hardly a person who has not suffered from tonsillitis at least once in his life. The causative agents of tonsillitis are staphylococci, streptococci and pneumococci. There are acute tonsillitis and chronic tonsillitis.
Acute tonsillitis (or tonsillitis) is an infectious disease that affects the palatine tonsils, as well as the lingual, laryngeal and nasopharyngeal tonsils.
In acute tonsillitis, the throat hurts, it is difficult to swallow, the body temperature rises, general weakness, chills, aching joints, and headache appear. With proper treatment and compliance with the instructions of the otorhinolaryngologist, the disease is cured in 5-7 days.
1
Diagnosis of chronic tonsillitis in MedicCity
2 Diagnosis of chronic tonsillitis in MedicCity
3 Diagnosis of chronic tonsillitis in MedicCity
Chronic tonsillitis is a common infectious disease in which the focal infection is in the palatine tonsils. The formation of a chronic inflammatory focus in the tonsils occurs due to prolonged exposure of microbes to the lymphoid tissue of the tonsils.
Chronic tonsillitis is characterized by periodic exacerbations - sore throats, but a non-angina form of the disease also occurs.
What is chronic tonsillitis
The human oropharynx has special structures called tonsils; they protect the body from pathogenic microorganisms. In childhood, these structures are subject to enormous stress, because every day the child comes into contact with new microbes that are not yet familiar to him.
When bacteria “settle” on the surface of the tonsils on the back wall of the pharynx, and the immune system cannot cope with them, inflammation develops - tonsillitis. If this inflammation persists for a long time, acute tonsillitis (tonsillitis) turns into a chronic inflammatory process.
Tonsils in chronic tonsillitis do not perform their functions, but on the contrary, they become a source of infection. This leads to infectious and autoimmune complications.
University
Currently, methods for rapid diagnosis of streptococcal antigen in smears from the surface of the tonsils and/or posterior pharyngeal wall (Streptatest, STREP-A-CHECK-1, Binax-Strep A) have become widespread, which allow obtaining results within 15–20 minutes . However, despite their high specificity (95–100%), they are characterized by lower sensitivity (60–80%) than culture tests.
However, neither cultural examination nor rapid tests make it possible to differentiate patients with ATP of streptococcal etiology from asymptomatic carriers of GABHS with intercurrent viral infection.
According to the 2012 ESCMID (European Society for Clinical Microbiology and Infectious Diseases) guidelines, smear culture for GABHS is not recommended routinely in all patients with acute sore throat. If there is a high probability of GABHS based on the assessment on clinical scales, rapid diagnostics should be carried out whenever possible; in the case of a negative result of the rapid test, bacteriological examination is not performed.
The IDSA (Infectious Diseases Society of America) recommends increased use of the rapid test and/or culture of the posterior pharyngeal swab because clinical symptoms are not considered reliable in differentiating ATF caused by viruses from GABHS unless severe symptoms of a viral infection (runny nose, cough, hoarseness and/or ulcerative lesions of the oral mucosa).
In children and adolescents, negative results of the rapid test should be confirmed by culture (in adults, this is not necessary due to the low prevalence of GABHS infection and the extremely low risk of developing rheumatic fever in the future). If the rapid test is positive, culture testing is not advisable. In children under 3 years of age, classic streptococcal ATP practically does not occur, and testing for GABHS in this age group is indicated only if it is diagnosed in a brother or sister.
Laboratory data also do not always allow one to distinguish a bacterial infection from a viral one. Markers of bacterial infection can be considered leukocytosis more than 15 x 109/l, neutrophilia more than 10 x 109/l and/or band forms more than 10% or more than 1.5 x 109/l, CRP more than 70 mg/l. Lower numbers or a significant increase in only one of these indicators are often found with viral infections. Thus, in 1/3 of children with tonsillitis caused by adenoviruses and the Epstein-Barr virus, leukocytosis exceeds 15 x 109/l, and CRP exceeds 60 mg/l. On the other hand, low marker numbers do not necessarily rule out a bacterial infection. Thus, laboratory markers of inflammation do not always help in the diagnosis of streptococcal infection, their diagnostic value is lower than that of catarrhal symptoms, and routine biochemical blood tests are not recommended for ATP.
Serological diagnosis of GABHS infection has become widespread. Most often in general clinical laboratories it is limited to determining the titer of antibodies to streptolysin O (ASL-O). True GABHS infections always cause a specific immune response—an increase in ASL-O titer. The determination of ASL-O in venous blood is a highly sensitive and specific (about 80%) reaction; the determination of ASL-O in capillary blood is much less reliable.
The synthesis of antibodies in general and ASL-O in particular depends on the individual characteristics of the immune response: in some it is pronounced and long-lasting, in others it is slow. Antibody synthesis starts 1–2 weeks after the onset of streptococcal infection, but even 8 weeks after GABHS tonsillopharyngitis, the ASL-O titer may not reach its maximum. ASL-O can remain at very high levels for up to a year.
The value of ASL-O in the acute period does not give any indication of the risk of developing immune complications and does not depend on the severity of the disease. On the other hand, if the patient has an increased ASL-O already in the first three days from the onset of tonsillopharyngitis, this excludes an acute streptococcal infection and indicates that the patient suffered from it within a period of 2 weeks to 6-12 months before the examination or suffers from chronic tonsillitis . Immune complications (glomerulonephritis, ARF) develop 3–8 weeks after GABHS infection; if they did not arise within these periods, then it is hardly possible to assume their development in the future (even despite the increased level of ASL-O).
It is necessary to clearly understand that ASL-O are antibodies of antigen recognition, and not of its elimination, and not treat the patient with antibiotics in order to normalize this indicator. The immune process has a certain stage, which develops despite the death of the pathogen. It is the infection that needs to be treated, not the elevated ASL-O level! Determination of the ASL-O titer is recommended only in cardiorheumatology and nephrology to prove the streptococcal etiology of heart and kidney damage.
To diagnose the streptococcal etiology of ATF, determination of the level of antibodies is not used; the diagnosis is verified by cultural methods. This test can be used to differentiate active infection from a carrier state. (The meaning of the definition of ASL-O was described in sufficient detail by Alexander Lavrinovich in “MV” dated January 5, 2022).
There are early and late (immune) complications of GABHS infection.
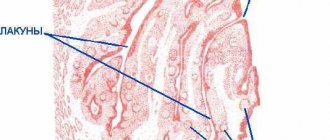
Early complications are represented by cervical lymphadenitis, paratonsillitis, parapharyngitis, retropharyngeal and peritonsillar abscesses. The etiology of these complications is associated with a combined flora (GABHS and anaerobes) penetrating into the peritonsillar tissue and lymph nodes from the depths of the lacunae in severe tonsillitis or as a result of injury, for example, during processing or shading of the tonsils. In this case, the patient, despite the treatment, continues to have fever, pain when swallowing, turning the head, and opening the mouth. Upon examination, asymmetry of the pharynx and bulging of the pharyngeal wall are revealed.
Immune complications of GABHS infection, which include post-streptococcal acute glomerulonephritis and acute rheumatic fever, are well known to clinicians. The latter disease develops in 0.3% of patients with untreated GABHS tonsillitis, of which 40% develop chronic rheumatic heart disease. Adequate ABT reduces the risk of developing acute rheumatic fever (ARF) by 80% and peritonsillar abscess by 85%.
The so-called rheumatogenous GABHS strains have a number of specific properties. Of particular importance is M-protein, a type-specific antigen located in the outer layer of the cell wall. Antibodies to M-protein cross-react with various tissues of the host body according to the principle of molecular mimicry as the main pathogenetic mechanism for the development of immune complications of GABHS infection. In addition, protein M has the properties of a superantigen, causing polyclonal activation of lymphocytes and the formation of low-affinity antibodies, which can lead to impaired tolerance to self-tissue antigens and the development of autoaggression, especially in genetically predisposed patients. These properties were noted in serotypes M-3, M-5 and M-18.
Immunopathological complications of GABHS infection develop in the convalescence stage. Acute glomerulonephritis manifests itself on the 7th–10th day of illness, and adequate therapy for angina does not reduce the risk of its development. The clinical manifestations of ARF appear 2–3 weeks after the symptoms of ARF are relieved, and fever occurs in no more than 30% of patients. However, even in the acute period of ATF, disorders of the internal organs are detected. Changes in the cardiovascular system are characterized by tachycardia, muffled or weakened heart sounds.
When body temperature normalizes, tachycardia gives way to bradycardia, and the dullness of heart sounds becomes even more pronounced. In 1/3 of patients in the acute stage of the disease, microhematuria is detected, which disappears when the intoxication syndrome is relieved. These pathological changes are associated with the direct effect of streptococcal toxins (exotoxins, streptokinase, hyaluronidase, etc.) on organs, are not related to immunopathological reactions and do not require any anti-inflammatory or immunosuppressive therapy.
Symptoms of chronic tonsillitis
Tonsillitis is accompanied by local symptoms directly in the throat, and general symptoms from other organs and systems.
Chronic tonsillitis is characterized by repeated recurrence of tonsillitis.
Main symptoms:
- pain and discomfort in the throat, it hurts the child to swallow solid food;
- enlargement and tenderness of the cervical lymph nodes;
- increase in body temperature to 37-38 degrees;
- bad breath;
- signs of intoxication - fever, headache, weakness;
- abdominal pain, nausea and vomiting;
- upon examination, redness of the pharynx, tonsils are visible, possibly with a white coating (normally, the tonsils do not protrude from the palatine arches, they are not visible).
The infectious process is not limited to the throat; symptoms of tonsillitis are followed by a runny nose, hoarseness, and cough. Possible development of conjunctivitis, otitis, meningitis.
Causes of chronic tonsillitis
Tonsillitis
- infection. Among the pathogens that can cause tonsillitis are:
- bacteria (streptococci, staphylococci, diphtheria bacillus, etc.);
- ARVI (influenza viruses, parainfluenza, adenoviruses);
- herpes viruses (cytomegalovirus, Epstein-Barr virus);
- measles virus;
- yeast fungi (candida).
Provoking factors include hypothermia, consumption of cold foods, contact with sick people, stress, and poor nutrition. Candidal tonsillitis may indicate immunodeficiency.
Complications due to improper self-medication and lack of treatment for tonsillitis
There are a simple form of tonsillitis - accompanied only by local symptoms, and a toxic-allergic (complicated) - manifestations of intoxication and dysfunction of all organs and systems come to the fore.
Toxic-allergic manifestations are characteristic of chronic tonsillitis of streptococcal origin. With this form, antibodies to streptococci are formed in the blood, which are also capable of attacking the body’s own tissues. The most vulnerable to such autoimmune aggression are the kidneys, heart and joints. Therefore, chronic tonsillitis leads to the following complications:
- glomerulonephritis and subsequently renal failure;
- endocarditis, myocarditis, pericarditis;
- rheumatism, rheumatoid arthritis, systemic lupus erythematosus.
Therefore, any tonsillitis should be examined and adequately treated. It is necessary to monitor the child’s condition for 3-4 weeks after recovery. If alarming symptoms appear in the heart (chest pain, rapid heartbeat, high temperature), joints (pain with movement, stiffness), kidneys (swelling, lower back pain), seek medical help.
Recommendations for the prevention of tonsillitis
To prevent the development of chronic tonsillitis, you must adhere to the following recommendations:
- avoid hypothermia of the child;
- protect him from communicating with sick people;
- monitor the child’s nutritional status;
- promptly show the child to a pediatrician or pediatric ENT doctor when the first symptoms of a sore throat appear;
- Visit the dentist with him in a timely manner to remove carious teeth, which are a source of bacterial growth in the mouth.
Prevention of sore throat
In order to reduce the likelihood of tonsillitis (acute tonsillitis) to a minimum, parents need to take a competent approach to strengthening the child’s immune system. To do this, the following preventive measures should be observed:
- Lead an active lifestyle - take frequent walks in the fresh air, involve your child in sports activities (running, swimming, football, cycling, etc.).
- Provide the child with a balanced diet - introduce a large amount of fresh vegetables and fruits, herbs, low-fat protein foods into the children's diet, and also limit the consumption of fatty, fried foods, fast food, and fast carbohydrates.
- Monitor the child’s personal hygiene, develop in young children the habit of brushing their teeth and washing their face daily (dental caries can cause infection in the tonsils).
- Ensure comfortable conditions in the children's room - maintain optimal humidity and air temperature (no more than 23C at a humidity of 50-60%), carry out daily wet cleaning and ventilation of the rooms.
- If any symptoms of diseases of the ENT organs occur, bring your child for medical examinations in a timely manner, trust only qualified specialists!
We employ experienced doctors of various specialties who will establish an objective diagnosis and select the correct treatment so that the baby can return to his normal lifestyle as soon as possible!
Diagnosis and treatment of tonsillitis
Diagnosis of chronic tonsillitis is made based on symptoms and examination data. To assess the general condition of the child, additional examination methods may be prescribed:
- general blood analysis;
- general urine analysis;
- chest x-ray;
- electrocardiography.
With chronic tonsillitis, a child may show signs of damage to other organs. Therefore, if necessary, a pediatric otolaryngologist can refer him for examination to specialized specialists (nephrologist, cardiologist, ophthalmologist, etc.).
Chronic tonsillitis involves drug treatment: gargling, antibacterial, anti-inflammatory drugs and physiotherapy.
If conservative treatment is ineffective, the child is indicated for a tonsillectomy (surgical removal of the tonsils).
Chronic tonsillitis is a focal infection that must be removed from the body as quickly as possible to preserve the child’s health.
Marshall syndrome in children
Imagine the condition of parents whose child suffers from a sore throat every month. We are talking about Marshall syndrome, which many treated like a regular sore throat. And the baby received a monthly dose of antibiotics. In fact, antiviral and antibacterial drugs are absolutely ineffective for this pathology. The only effective method of treating the disease in this case is the use of glucocorticosteroid drugs such as Prednisolone or Dexamethasone. But this does not guarantee that in a month the child will not again develop symptoms of Marshall syndrome. The radical treatment method in this case is removal of the tonsils.