Directions for use and doses
Inside. Take one dose 2-3 times a day in between feedings for 3 days.
The method for opening the package and taking the drug is presented in the figures.
Figure 1. Open the sachet.
Figure 2. Separate one PE container.
Figure 3. Open the PE container by turning the head.
Figure 4. Sitting the child. Lightly press the container to squeeze its contents into the child's mouth.
Place the remaining containers in a sachet and close it by folding over the open side.
Can the physiological process of teething in infants be pathological?
I.N.ZAKHAROVA, Doctor of Medical Sciences, Professor, I.N. KHOLODOVA, Doctor of Medical Sciences, Professor, Yu.L. DMITRIEVA, Ph.D., N.V. MOROZOVA, MD, M.V. MOZZHUKHIN, D.I. KOLODOV
Russian Medical Academy of Postgraduate Education, Moscow
The article discusses the problem of teething in infants, listing the mechanisms and factors influencing this process. Scientific studies are presented that show the significance of various clinical symptoms during teething in children, the dependence of this process on the type of constitution of the child, and also the issues of modern therapy for pathological teething are considered.
Key words: infants, constitutional type of children, teething, pathological symptoms, homeopathic medicines.
Teething is one of the stages in the development of a baby's teeth. This period is determined by the growth and development of the baby and is considered as a physiological process that is in close connection not only with the general state of health, but also with its constitution. In most children, teething does not cause any serious complications or complaints [1]. However, in a number of infants, teething affects his well-being, causing certain pathological symptoms.
The eruption of primary teeth is influenced by various factors. A number of researchers believe that the main significance in the process of teething is the human genotype and his constitution, although the role of various external environmental factors cannot be ruled out. Some dentists believe that children of elderly parents erupt teeth somewhat earlier than children of young parents. First-born children begin to erupt teeth earlier than second and third children, and girls begin to erupt a little earlier than boys [2]. Many experts note that there is a direct relationship between the degree of prematurity of the child and the timing of the eruption of baby teeth. Thus, in healthy premature children, the timing of the eruption of baby teeth generally corresponds to those in healthy full-term children. In premature infants with a history of complicated neonatal period (intracranial birth injury, infectious and inflammatory diseases), this process begins at a later date (at 11-12 months and after a year) and depends on the severity of the pathology suffered. Features of the mother's pregnancy also influence the physiology of teething. There is evidence that in children whose mothers suffered from toxicosis during pregnancy, the eruption of baby teeth is delayed. Some authors believe that the eruption of primary teeth occurs at a later date in children born to mothers with congenital heart defects. Diseases suffered during the first year of life are of great importance in the formation of a child’s dental system. Many researchers note that with rickets, the appearance of baby teeth occurs late and in violation of the correct order [3].
There are several theories explaining the process of teething, among which the most convincing are the following [4]:
- Hunter's theory, according to which the growing roots of the tooth abut the hard bony bottom of the bony alveolus and the tooth is pushed out of the bony alveolus;
- Yasvoin's theory, according to which the cause of teething is the differentiation processes occurring in the tissue of the dental papilla, as a result of which a large amount of basic substance accumulates there. The increase in pulp volume creates pressure inside the tooth germ, which forces it to move towards the free edge of the gum;
- Katz's theory, which believes that the growing tooth puts pressure on the lateral walls of the alveoli, which leads to superficial bone resorption. At the same time, new bone is deposited on the outer surface of the alveolar processes and on its upper edge. Bone tissue accumulates in the area of the bottom of the alveolus, which leads to an increase in tissue pressure there, pushing the tooth to the surface.
It should be noted that none of these theories can fully explain the complex mechanism of teething. By the time the tooth erupts, the area of bone covering the crown of the tooth is reabsorbed. The same processes are observed in the gums. During the growth of the tooth root, bone restructuring and gradual deepening of the dental alveoli also occur. At the same time, morphological changes occur in the tissues surrounding the tooth: increased blood flow, changes in vascular permeability, increased production of the main substance of the pulp and periodontium [5].
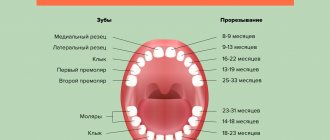
The eruption of baby teeth usually begins at 6-7 months of age. By this time, the development of the crown of the baby tooth ends and the formation of its root begins. The connective tissue of the gums, lying in the path of the erupting tooth, is gradually compressed and atrophies. The reduced enamel epithelium covering the crown of the tooth comes into contact with the gingival epithelium and merges with it. Following this, a breakthrough of the epithelium occurs above the apex of the crown, and it appears in the oral cavity. As the tooth erupts, the epithelium of the gum margin surrounding it turns into a reduced enamel epithelium, covering the not yet erupted part of the tooth crown. This epithelium grows tightly together with the enamel shell and gradually separates from it only during the eruption of the tooth crown. However, even after the end of tooth eruption, this epithelium remains in the area of the lower third or quarter of the tooth crown. Located in the form of a thin border around the neck of the tooth, it forms the so-called. epithelial attachment, or gingival margin. Where the epithelium departs from the surface of the enamel, the bottom of the gingival crevice, or pocket, appears.
Can the physiological process of teething be complicated by any pathological symptoms? In 2002, American researchers published the results of a survey, the purpose of which was to establish the attitude of pediatricians, pediatric dentists and parents to various symptoms most often associated with teething. Most respondents tended to associate teething in babies with symptoms such as fever, restlessness, swollen gums, increased drooling and sleep disturbances. When comparing the answer options between the groups of respondents who took part in the survey, it was noted that the last three symptoms were significantly more often associated by parents and dentists with the dental process. The most significant differences in the attitude of the respondents were obtained regarding changes in stool character as a symptom of teething. The majority of parents (56.7%) and dentists (52.0%) were convinced that the connection was obvious, while only 9.1% of pediatricians supported this point of view [6]. The works of other foreign authors [7, 8, 9] noted that the appearance of drooling, fever, desire to bite, dermatitis on the chin, cheeks, neck associated with irritation with saliva, rhinitis, wet cough and pasty stool against the background of teething is observed in 35-60% of children. In this case, the temperature rise does not exceed 38 ° C and lasts no more than 1-2 days. Fever is caused by the release of biologically active substances in the tooth growth zone and resolves on its own soon after its eruption [8,10]. A change in consistency towards liquefaction or increased frequency of stools is caused by the release of a large amount of saliva, which stimulates intestinal motility [8,10].
In 2012, we, together with employees of the Department of Pediatrics of the State Budget Educational Institution of Higher Professional Education YAGMA of the Ministry of Health of the Russian Federation, conducted a survey of 50 local doctors. To the question: “Do you often encounter children in the first year of life with painful teething syndrome?” — 46% of doctors answered that in approximately 10-30% of cases. Of the symptoms most often accompanying teething, pediatricians ranked increased drooling in first place, followed by the desire to bite, irritability, refusal to eat and increased body temperature. More than 60% of doctors indicated that teething syndrome is often combined with manifestations of acute respiratory infection. Doctors explained this fact by the fact that against the background of teething, the child’s body’s resistance to viruses and bacteria decreases.
Researchers from Cleveland conducted a large prospective study, the purpose of which was to establish the most characteristic symptoms of teething [7]. The work included 125 infants who were monitored from 4 months. up to 1 year. At the same time, parents recorded tympanic temperature daily and noted the possible presence of one or more of the 18 symptoms offered in the child. The authors found that symptoms such as increased salivation, swelling of the gums, anxiety, sleep disturbance, facial flushing, decreased appetite for solid food and a slight increase in body temperature were statistically significantly associated with the dental process. However, significant differences were recorded only for 8 days (4 days before, on the day of teething and 3 days after teething), which allowed the authors to call this period the “eight-day teething window.” The period identified by the authors allows the doctor to navigate in terms of the duration of therapy: 7-8 days. Dilution of stool or an increase in its frequency, decreased appetite for liquid food, cough, the appearance of dermatitis, vomiting and an increase in body temperature above 38.5 °C were not significantly associated with the process of teething, but more often corresponded to the onset of an acute respiratory disease [7].
A similar prospective study was conducted by Brazilian authors [11]. 47 children aged 5 to 15 months were taken under observation. During the study period, children underwent daily measurement of tympanic and axillary temperature, examination of the oral cavity and registration of possible symptoms of dentition. Based on the results of the analysis of the data obtained, it was found that the process of teething was significantly associated with an increase in tympanic temperature on the day of tooth emergence, as well as the presence of symptoms such as irritability (p < 0.001), increased salivation (p < 0.001), rhinorrhea (p < 0.001 ) and decreased appetite (p < 0.001) [11].
Our own observations of children showed that in children of different types of constitution this process proceeds differently (Table 2). Thus, in children with a lymphatic-hypoplastic type of constitution, which are characterized by lymphadenopathy, excess body weight, a tendency to atopic dermatitis and rickets, as a rule, the eruption of primary teeth occurs late and in the wrong order. They usually experience severe anxiety, crying, abnormal bowel habits, swelling and soreness of the gums, and excessive salivation. A significant delay in teething may be a consequence of pathology of the endocrine system, in particular congenital or transient hypothyroidism [12].
In a number of children who can be classified as having a neuro-arthritic type of constitution, the first teeth, as a rule, appear on time, but their eruption is often accompanied by severe pain, excitability, episodes of crying for several hours, and sleep disturbances. Refusal to eat, regurgitation and vomiting may occur. It is these children who, when teething, may have a rise in temperature up to febrile levels. Children of this type of constitution usually have good growth, underweight, they are hyperactive, excitable, they are characterized by imbalance, causeless rises in temperature, regurgitation, vomiting, and acetone states (Table 1).
In children with an allergic type of constitution, the process of teething is often accompanied by the appearance or exacerbation of allergic dermatitis, stool upset, tearfulness, and loss of appetite. In these children, during teething, acute respiratory infections are often associated, which is probably due to their characteristic features: lability of water-salt metabolism, anaerobic type of metabolism, excessive histamine synthesis, decreased phagocytosis activity, increased permeability of the vascular wall.
Thus, the information available in the literature allows us to conclude that in a number of children the process of teething may be accompanied by pathological symptoms and impairment. Unfortunately, in not a single scientific study have we been able to identify symptoms that could reliably indicate teething and would allow us to make a differential diagnosis between this process and an incipient acute respiratory infection. Knowing the type of constitution allows you to predict how teething will proceed in each individual child, and plan preventive measures aimed at reducing pathological symptoms in this situation.
To make teething easier for your baby, you need to:
- give him more attention from his parents;
- more frequent breastfeeding, which has a sedative effect and increases resistance to infections;
- Invite the child to pick up a teether, which should be clean, preferably cool. because such material, when in contact with the gums, slightly soothes pain and reduces inflammation;
- massage the gums, for which you need to wrap your index finger with a gauze swab dipped in cold water and gently massage the child’s gums;
- provide gentle care for the skin around the mouth;
- use medications if necessary.
There are many drugs that facilitate teething, most of them exist in the form of gels (Table 2).
The disadvantages of using these products include the short-term effect of the gel due to its rapid rinsing with saliva, as well as the possibility of developing allergic reactions to its components [10]. In addition, to improve the general condition and reduce the temperature, drugs such as paracetamol and gels with a local anesthetic effect are used. Frequent use of these drugs may contribute to the development of unwanted side reactions and toxic effects.
When teething, you can use natural remedies (homeopathic medicines). The works of a number of authors have shown their high efficiency and safety, including in pathological teething [13,14,15,16, 17,18,19]. Complex homeopathic preparations are non-toxic and are effective and safe. The prescription of complex homeopathic medicines makes it possible to make a differential diagnosis between teething and an incipient acute respiratory infection. If pathological symptoms are associated with teething, they usually stop or decrease by the second day from the start of treatment with homeopathic medicines [17,19]. If the baby does not feel better after 1-2 days of therapy, it is necessary to reconsider your treatment tactics towards the treatment of an acute respiratory infection.
One of the homeopathic medicines is Dentokind tablets. Dentokind contains the following components: belladonna - belladonna. This drug has been used in France since 1994 in children in the form of an oral solution. Dantinorm Baby contains components that can affect teething symptoms: chamomile (Chamomilla vulgaris), which is traditionally used to relieve pain, has an anti-inflammatory and soothing effect; "Indian ivy" (Phytolacca decandra), used to reduce soreness and inflammation of the gums; Rhubarb (Rheum officinale), used for digestive disorders, affects intestinal motility and helps eliminate diarrhea. The drug is used in one dose 2-3 times a day in between feedings for 3 days.
For ease of use, I have developed special hygienic packaging: dosed polyethylene containers, each of which corresponds to one dose of the drug, which can be easily dropped into the child’s mouth, avoiding contact of the solution with hands. You can give the drug not only at home, but also while walking.
“To date, there have not been any cases of side effects of the drug and/or allergic reactions; it can be combined with the use of other drugs. In a randomized multicenter study [18,19], 597 children aged 3 to 24 months were observed. with symptoms of teething, while 97% of children had local symptoms, and 94% had general ones. Children received several treatment options: 1st treatment option - homeopathic medicine only, or systemic analgesics, or dental gels; The 2nd treatment option is the combined use of these drugs. The drug Dantinorm Baby (French name CamiUia) was received by 71% of children as monotherapy and in combination with other drugs; systemic analgesics - 69%; dental gels - 64% of children. After 7 days of therapy, improvement or complete absence of pathological
symptoms were noted in 94% of children receiving CamiUia (Dantinorm Baby) as part of therapy. Note that 81% of the parents of these children were completely satisfied with the effectiveness of the treatment.
This study showed that the complex homeopathic drug Dantinorm Baby can be successfully prescribed in the treatment of pathological teething. Dantinorm Baby is especially indicated for children with changes in stool character and diarrhea due to teething, when rectal suppositories are difficult to use, and in cases where severe pain in the gums does not allow the use of other dosage forms and the child even refuses to drink. Therefore, the use of the drug from sterile single-dose containers in drops is optimal.
Thus, in modern conditions, it is necessary to conduct further research aimed at identifying the most significant signs of teething, and differential diagnosis with other pathological conditions (acute respiratory infection, functional disorders of the gastrointestinal tract). The use of natural products in children opens up prospects in the treatment of pathological teething in children. This therapy is safe and effective.
LITERATURE
1. Tatochenko V.K. Pediatrician for every day. 2007. 5th ed., revised. and additional M., 2007.272 p.
2. Belousova N.A., Belousova E.G.. Caring for a healthy child: development and eruption of baby teeth. District pediatrician, 2009.1: 7.
3. Persii L.S., Elizarova V.M., Dyakova S.V. Pediatric dentistry. 5th ed., revised. and dollars M.: Medicine, 2003. p.43-45.
4. Pediatric therapeutic dentistry: national guidelines. Ed. VC. Leontyeva, L.P. Kiselnikova. M.: GEOTAR-Media, 2010.896 p.
5. Gaivoronsky I.V., Petrova T.B. Anatomy of human teeth. Tutorial. St. Petersburg: ELBI-SPb, 2005. 56 p.
6. Barlow BS, KaneLlis MJ, SLayton RL Tooth eruption symptoms: a survey of parents and health professionals. ASDCJ Dent Child, 2002 May-Aug, 69(2): 148-50,123-4,
7. Macknin ML, Piedmonte M, Jacobs J, Skibinski C. Symptoms associated with infant teething: a prospective study. Pediatrics, 2000 Apr, 105(4 Pt 1}: 747-52.
8. Perets B, Ram D, Hermida L et at Sistemic manifestation during eruption of primary teeth in Infants./ Dent child., 2003,70:170-173.
9. Cunha RF, Pugliesi LM, Garcia LD et aL Sistemic and local teething disturbances: prevalence in a clinic for infants./ Dent child., 2004,71: 24-26.
10. Tsong AKL.Teething, teething pain and teething remedies, int. DentmAns Ed, 2010,5(4): 14-28.
11. Ramos-Jorge J, Pordeus IA, Ramos-Jorge ML, Paiva SM. Prospective longitudinal study of signs and symptoms associated with primary tooth eruption. Pediatrics, 2011 Sep, 128(3): 471-6.
12. Persii L.S., Elizarova BM, Dyakova SV. Pediatric dentistry. Ed. 5th, revised and additional M.; Medicine, 2003. pp. 43-45.
13. Bedareva T.P. Antihomotoxic therapy as a necessary stage in the rehabilitation of children with diseases of the digestive system. Biol. Med., 2000,2:48-51.
14. Ilyenko L.I., Syryeva T.N., Kholodov D.I., Gainova L.V., Semashina G.A. The use of natural products for pathological dentition in children of the first years of life. Questions of Pediatric Dietetics, 2011,9,2:2-4.
15. Shpigel A.S. Evaluation of the effectiveness of antihomotoxic pharmacotherapy in accordance with the principles of evidence-based medicine. Viol Med 2002,2:56-64.
16. Kurz R, Clinical medicine versus homeopathy. Pediatr. Padol., 1992,27: 37-41.
17. Ilyenko L.I., Kholodova I.N., Syryeva T.N., Kholodov D.I., Ilyina ID. New opportunities to improve the quality of life of children with painful teething. Pediatrics 2010,89, 4:106-110.
18. Kazyukova T.V., Kotlukov V.K., Shevchenko N.N., Rusakova VD Symptoms of teething in infants: condition or disease? Pediatrics 2013,92,4:1-5.
19. Stagnara J, Besse R, Feyard AL et aL P174. Symptomatologie et prise en charge de la pausse dentaire. Archives de p'diotrie, 2010,17{6S1): 93-94. Doi: 10.1016/S0929-693X (10) 705 74-1.
Published: Medical Council, No. 01, 2016.
On terms of commercial partnership
Read the instructions