1.General information
Actinomycosis is a fairly typical chronic infectious-inflammatory disease, caused, however, by a not quite typical pathogen.
The fact is that actinomycetes, a rod-shaped microorganism from the class of actinobacteria, show some similarities with fungal cultures, since during the life cycle they form the so-called. thin filaments similar to mushroom mycelium. The word “actinomycetes” itself literally means “ray” or “radiant fungi”, although at present this term is not used as outdated and does not correspond to reality: actinomycetes are precisely bacteria. In nature, they are found primarily in soil; Once in the human body, they form colonies in the oral cavity, gastrointestinal tract, tonsils, and skin.
Their pathogenic activity under certain (unfavorable for humans) conditions leads to actinomycosis: infiltrative damage to the skin and internal organs, with the formation of suppuration and fistulas. There is no exact epidemiological information regarding actinomycosis, but it is known that this infection is rare. The incidence does not depend on the region of residence and is estimated at approximately one case per 300 thousand people per year. It has been repeatedly proven that men get sick up to three times more often, with the peak incidence occurring in the age group of 30-60 years. Some publications report that urban residents are more susceptible to this disease.
A must read! Help with treatment and hospitalization!
Publications in the media
A variety of microorganisms, populating almost any natural environment, invisibly accompany a person throughout his life. Living in soil, water, air, on plants, on the walls of residential and industrial premises, microorganisms are constantly in contact with humans. And, as a result, some of them have adapted to life on the skin, mucous membranes and internal cavities of humans (gastrointestinal tract, upper respiratory tract, urogenital tract, etc.), forming complex associations with specific relationships in their habitats. The human body normally contains hundreds of types of microorganisms: bacteria, protozoa, viruses, fungi. Opportunistic microorganisms constitute the normal microflora of a person, without causing harm to him. The term “normal microflora” unites microorganisms that are more or less often isolated from the body of a healthy person. It is often impossible to draw a clear boundary between saprophytes and pathogenic microbes that are part of the normal microflora. All microbes living in the human body simultaneously exist in these two states. Any of them can be the cause of infectious processes. Harmless “helpers” (lactobacteria, bifidobacteria) with a high degree of colonization can cause diseases. Conversely, pathogenic bacteria (pneumococci, meningococci, clostridia) colonizing the surfaces of human organs do not cause infection, which is facilitated by the competition of previously formed microflora and the protective properties of the macroorganism.
One of these “double” agents of human normobiota are actinomycetes.
They are widespread in the environment: in soil, water, including tap water and spring water, in hot mineral springs, on plants, on rocks and even in deserts. In the human body, actinomycetes saprophyte on the skin, in the oral cavity, dental plaque, tonsil lacunae, upper respiratory tract, bronchi, on the mucous membrane of the gastrointestinal tract, vagina, anal folds, etc.
The term actinomycetes (an outdated name for radiant fungi) currently extends to a wide range of gram-positive aerobic and microaerophilic bacteria that have the ability to form branching mycelium with characteristic sporulation, as well as irregularly shaped rods and coccoid elements that are formed as a result of fragmentation of the mycelium.
Actinomycetes include bacteria of the genera Actinomyces, Actinomadura, Bifidobacterium, Nocardia, Micromonospora, Rhodococcus, Streptomyces, Tsukamurella, etc.
The transition of actinomycetes from a saprophytic to a parasitic state is facilitated by a decrease in the immune defenses of the body, the presence of severe infectious or somatic diseases (chronic pneumonia, hidradenitis suppurativa, diabetes, etc.), inflammatory diseases of the mucous membranes of the oral cavity, respiratory and gastrointestinal tract, surgical interventions , long-term use of intrauterine contraceptives, hypothermia, injuries, etc.
In such cases, actinomycosis develops - a chronic purulent non-contagious disease caused by the formation of characteristic bluish-red and then purple infiltrates of dense consistency with multiple foci of fluctuation and fistulas with purulent discharge in soft and bone tissues of almost any localization. The duration of the incubation period can vary from 2–3 weeks to several years (from the time of infection to the development of manifest forms of actinomycosis).
The leading way in the development of actinomycosis is the endogenous method, in which the pathogen penetrates into tissues from places of its saprophytic habitat, most often through the digestive tract and oral cavity (carious teeth, gum pockets, tonsil crypts). The most favorable conditions for the introduction of actinomycetes are created in the large intestine, due to stagnation of food masses and a greater likelihood of injury to the wall. With the exogenous method, pathogens enter the body from the environment aerogenously or through traumatic injuries to the skin and mucous membranes.
The spread of actinomycetes from the primary lesion occurs by contact through the subcutaneous tissue and connective tissue layers of organs and tissues. The hematogenous route is also possible when an actinomycotic granuloma breaks through into a blood vessel.
The main causative agents of actinomycosis are Actinomyces israelii, A. bovis, Streptomyces albus, Micromonospora monospora; nocardiosis (“atypical actinomycosis”) and mycetoma - Nocardia asteroides, N. brasiliensis. The list of detected pathogenic actinomycetes is expanding. Modern literature increasingly describes cases of actinomycosis caused by rare species: Actinomyces viscosus, A. graevenitzii, A. turicensis, A. radingae, A. meyeri, A. gerencseriae, Propionibacterium propionicum, etc.
In the emergence and formation of the actinomycotic process, accompanying aerobic and anaerobic bacteria also play a significant role. Most cases of actinomycosis are caused by polymicrobial flora. Usually, along with actinomycetes, Staphylococcus spp., Streptococcus spp., Fusobacterium spp., Capnocytophaga spp., Bacteroides spp., representatives of the Enterobacteriaceae family, etc. are isolated. The addition of pyogenic microorganisms aggravates the course of actinomycosis, changes its clinical picture, and contributes to the spread of the process.
The clinical picture of actinomycosis is varied and is found in all countries in the practice of doctors of various specialties (dentists, surgeons, dermatologists, gynecologists, etc.). The main localizations are maxillofacial (up to 80%), thoracic, abdominal, pararectal, mycetoma (Madura foot). In addition, actinomycotic lesions appear not only in the classical form with characteristic tissue infiltration, abscesses and fistulas, but also in the form of the dominant pathogenic flora of a nonspecific inflammatory process, complicating the course of the underlying disease.
Actinomycetes may play an active role in the etiology of chronic tonsillitis. The palatine tonsils are colonized by actinomycetes in chronic tonsillitis and, in association with other bacteria, often provoke inflammatory reactions. Actinomycotic bacteremia of the oral cavity may occur as a result of dental procedures. In 30% of cases out of 80% of identified bacterimia, the actinomycotic nature of stomatitis is determined, the etiological agents of which are saprophytes of the oral cavity - A. viscosus, A. odontolyticus and A. naeslundi. By joining the local pathogenic flora, actinomycetes contribute to the development of a long-term non-healing inflammatory process with acne, trophic ulcers, hyperemia, maceration and weeping on the skin. Possessing a high degree of intestinal colonization, they are one of the main agents of dysbiosis. Summarizing all of the above, it should be noted that bacteria from a large group of actinomycetes can appear as participants in any infectious and inflammatory manifestations of the human body from dermatitis to endocarditis.
Thus, actinomycosis, characterized by a variety of localizations and clinical manifestations, needs to be diagnosed in a timely manner and possibly effectively treated, knowing the patterns of pathogenetic development, predisposing factors of infection, characteristics of pathogens and treatment methods.
However, the diagnosis and treatment of diseases associated with actinomycetes are the subject of a few specialized laboratories and clinics in the world. Difficulties in their differential diagnosis hinder the widespread recognition of these microorganisms in clinical practice.
Diagnosis of actinomycosis
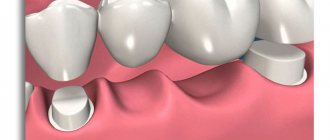
A reliable sign of actinomycosis is the detection of characteristic actinomycotic drusen in the form of small yellowish grains, resembling grains of sand, in pus from fistulas, in biopsies of affected tissues. In native (not stained) and histological preparations, drusen are clearly visible against the background of purulent detritus in the form of radiant formations with a denser homogeneous granular center of thin, densely intertwined mycelium (photo 1). For their ability to form radially arranged filaments of mycelium, often with “cones” at the ends, actinomycetes were once called “radiant mushrooms”. The leading role in the formation of drusen - tissue colonies of actinomycetes - is the response of the macroorganism to antigens secreted by actinomycetes into the environment. Drus formation helps slow down the dissemination of the pathogen in the affected organism, as well as the localization of the pathological process. Actinomycosis is characterized by specific tissue reactions: granulomatous productive inflammation, leukocyte infiltration, microabscesses, “cellular” tissue structure, specific granuloma surrounded by polynuclear cells, giant and plasma cells, lymphocytes and histiocytes.
In the body of patients, drusen do not develop at all stages of the disease and are not characteristic of every variety of “radiant fungus”, so they are not always found, and the absence of drusen at the initial stages of diagnosis does not deny actinomycosis. In addition, these formations are capable of spontaneous lysis, calcification, deformation, calcification and other degenerative changes.
Drusen do not form in nocardiosis. In tissues, Nocardia is found in the form of thin mycelial filaments 0.5–0.8 μm and rod-shaped forms of the same thickness. Due to its acid resistance, Nocardia stains well according to Gram-Weigert in blue and according to Ziehl-Neelsen - in red: all this allows for differential diagnosis between actinomycosis and nocardiosis, since this is dictated by the difference in treatment methods for these diseases.
Microbiological examination, which includes microscopy and inoculation of pathological material on nutrient media, is important for the verification of actinomycosis of any localization. The optimal temperature for growth is 35–37°C.
When microscopy of clinical material and grown cultures stained with Gram or methylene blue, actinomycetes look like branched filaments 10–50 µm long or are represented by polymorphic short rods 0.2–1.0×2–5 µm, often with club-shaped ends, solitary, in pairs of V- and Y-shape configurations and in stacks. Gram-positive, but often the coloring is not typical, in the form of a rosary.
Many aerobic actinomycetes grow well on common bacteriological media - meat-peptone, trypticase-soy, blood and brain heart agars. To identify microaerophilic species, thioglycollate medium is used. The cultural characteristics of actinomycetes are very diverse. On dense agar media, colonies resemble bacterial ones in size - 0.3–0.5 mm in diameter. The surface of the colonies may be flat, smooth, bumpy, folded, granular or mealy. The consistency is doughy, crumbly or leathery. Many actinomycetes form pigments that give the colonies a variety of shades: grayish, bluish, orange, crimson, greenish, brown, blackish-violet, etc.
Clinical aerobic isolates, for example Nocardia asteroids and Streptomyces somaliensis, on a rich nutrient medium produce so-called atypical growth - dense leathery colonies, usually not pubescent with the aerial mycelium so typical of strains and without sporulation. To demonstrate differentiation and the formation of characteristic spores and pigments, special media are required: with colloidal chitin, soil extract or decoctions of plant materials.
In a liquid nutrient medium, pure cultures of microaerophilic actinomycetes form whitish “lumps” suspended in the substrate. The environment remains transparent. If there are bacterial impurities, the medium is cloudy and homogeneous.
Description of clinical cases of “atypical” actinomycosis
During the period of 2007, 25 patients with various clinical forms of actinomycosis were under our supervision. Among the examined patients there were 12 women and 13 men (aged 15-25 years - 4 people, 26-35 years - 4 people, 36-45 - 2, 46-55 - 5 people and 56-66 years - 10 people).
In addition to the “classical” actinomycosis of the maxillofacial, axillary and inguinal areas in the fistulous stage, we diagnosed actinomycotic complications of various pathological processes. For example, actinomycetes were found in the vaginal discharge of a patient with nonspecific colpitis and vulvovaginitis, which seriously aggravated the course of the underlying disease and required multiple courses of anti-inflammatory therapy. Actinomycetes in diagnostically significant quantities were identified during inflammatory processes in the oral cavity (in scrapings from the pharynx, tonsils, tongue), during otomycosis, during long-term non-healing macerations and hyperemia of the skin in the perianal area, from the mucous membranes of the rectal ampulla. The addition of actinomycetes to the pyogenic microbiota of trophic ulcers significantly aggravated the course of the disease, complicated the process of treating such patients, slowing down the regression of lesions. In patients with acne, when opening foci of inflammation in the sebum, actinomycetes were often found, the presence of which contributed to the development of a protracted course of the disease.
Under our observation was patient K., 43 years old, with a rare case of primary actinomycosis of the skin of the soft tissues of the groin areas, fistulous form.
She has been ill for 1 year, when changes appeared in the groin area on the left due to constant rubbing of the skin with uncomfortable underwear. I didn’t go to the doctors. It worsened in December 2007, when 2 ulcers and fistulas with purulent discharge appeared. She was consulted by a dermatologist who suspected a neoplastic process. Examined by an oncologist and parasitologist. The diagnosis of cancer or parasitic disease could not be established. She was referred to a mycologist with suspicion of deep mycosis. On examination: the lesion is located in the left groin area, measuring about 1.7x5 cm, there are 2 functioning fistulas with scanty purulent and sanguineous discharge. The patient was examined in the mycological laboratory of the Institute. E. I. Martsinovsky MMA named after. I.M. Sechenov for actinomycosis and bacterial infection. In the pathological material studied, microscopy of the specimens revealed actinomycetes, rods, cocci, and leptotrichia. When purulent discharge from fistulas was inoculated onto nutrient media, the growth of actinomycetes and coccal flora was obtained.
The diagnosis of actinomycosis of skin and soft tissues was verified. The patient is being observed and treated by a mycologist.
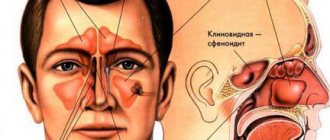
Patient N., 24 years old, diagnosed with acne, actinomycosis (photo 2).
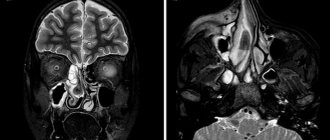
Complaints of rashes on the skin of the body since childhood. We can reliably say that the disease was 10 years old, when acne was diagnosed at the age of 14. The patient was treated with external agents and antibiotics of various groups with a temporary effect. The general condition is currently complicated by chronic gastritis. On examination: the skin of the torso, face, and back is affected by inflammatory elements (papulopustular rash, open and closed comedones), in some places confluent in nature, infiltration of the skin and soft tissues. A microscopic examination of sebum from acne elements in the patient revealed cocci and single rods. In culture from the test material under the conditions of a mycological laboratory (photo 3).
Diagnosis: acne, actinomycosis of the face, trunk, back of the skin and soft tissues of a secondary nature, infiltrative form in the stage of moderate exacerbation. Currently, the patient is being treated by a mycologist at the clinic of the Institute named after. E. I. Martsinovsky MMA named after. I. M. Sechenov.
Treatment
Treatment of patients with actinomycosis is carried out comprehensively in various combinations depending on the location and clinical manifestations - iodine preparations, antibiotics, immunocorrective and restorative agents, actinolysate, local treatment with ointments, physiotherapeutic procedures and surgical intervention.
Iodide preparations (up to 3 g of potassium iodide per day), previously dominant in the treatment of actinomycosis, can now be used in combination with antibiotics or radiotherapy as an additional means for softening and resorption of the infiltrate.
Antibiotics occupy a leading place in the treatment of actinomycosis . The most commonly used antibacterial drugs are from the group of tetracyclines, penicillins, carbopenems, lincosamines, aminoglycosides, cephalosporins, the active ingredients of which are gentamicin, amikacin, tobramycin, lincomycin, levofloxacin, cefaclor, cephalexin. The drugs “Panklav”, “Flemoxin Solutab”, “Unidox Solutab”, etc. have proven themselves well. A long course of antimicrobial therapy (from 6 months to 1 year) and high doses of drugs are required. Traditional therapy for actinomycosis involves intravenous penicillin at a dose of 18–24 million units daily for 2–6 weeks, followed by oral penicillin, amoxicillin, or ampicillin for 6–12 months. In milder cases, in particular with cervical-maxillofacial actinomycosis, less intensive treatment with short courses of antibiotic therapy is sufficient. There is experience with effective short-term treatment of actinomycosis with imipenem for 6–10 weeks and ceftriaxone daily for 3 weeks. Antimicrobial therapy is continued for some time after symptoms disappear to prevent relapse.
When treating actinomycosis, it is also necessary to take into account the adjoining pathogenic microflora, which may exhibit increased resistance to antibiotics, which is explained by the long-term previous use of various chemotherapy drugs. To influence the accompanying flora, metronidazole (Metrogyl, Trichopol, Efloran) and clindamycin (Dalacin, Klimitsin) are used. A good anti-inflammatory effect is shown by the use of sulfonamide drugs (co-trimoxazole, sulfadimethoxine, sulfacarbamide). When a mycotic infection occurs, antifungal drugs are prescribed: fluconazole, itraconazole, terbinafine, ketoconazole, etc.
Immunocorrective agents . To correct immunodeficiency, Diucifon is indicated orally - 0.1 g 3 times a day or intramuscularly in the form of a 5% solution of 5 ml every other day for 3-4 weeks. In our opinion, the immunocorrective drug “Cycloferon” has also proven itself well - 2 ml intramuscularly every other day, 10 days.
General strengthening therapy stimulates the body's reactivity and increases the effectiveness of immunotherapy. Detoxification therapy is carried out with intravenous solutions of Hemodez, 5% glucose solution, etc. In order to activate regeneration, autohemotherapy is used - weekly, for a total of 3-4 transfusions per course. Vitamins are prescribed in average therapeutic doses.
Immunotherapy with Actinolysate promotes the accumulation of specific immune bodies and improves treatment results, allowing to reduce the amount of antibacterial agents and avoid unwanted side effects. Actinolysate is administered intramuscularly 2 times a week, 3 ml, for a course of 25 injections, courses are repeated 2-3 times with an interval of 1 month.
As local therapy , ointment treatment with antibacterial drugs of these groups, washing of fistulas with antiseptic solutions, furan-type drugs, administration of 1%, 2%, 5% alcohol solution of iodine, which help cleanse actinomycosis foci and eliminate inflammatory phenomena, are indicated.
Physiotherapeutic procedures . At the stage of lesion formation, electrophoresis of calcium chloride and Diphenhydramine is performed. After opening the lesions with residual infiltrates, iodine electrophoresis, Lidase, and fluoridation are prescribed. Ultrasound is applied directly to the area of the lesion according to the generally accepted scheme for 12–25 days (depending on the condition of the patient and the lesion) at intervals of 3–4 months.
Surgical treatment is carried out against the background of conservative therapy and consists of radical excision of lesions within apparently healthy tissue. If it is impossible to carry out radical surgery (for example, with cervical-maxillofacial actinomycosis), opening and drainage of abscess foci is indicated.
2. Reasons
The main predisposing factor is weakened immunity. Infection most often occurs through direct or indirect contact with the soil, or actinomycetes already present in the body are activated. There have been no reported cases of infection from an infected person or sick animal. Skin inflammation, as a rule, is secondary in nature - the pathogen spreads in the body through the blood and/or lymph.
Risk factors are injuries (including thermal), fractures, gastric ulcers, acute appendicitis, dysentery, staphylococcal infections, etc., as well as long-term use of intrauterine contraceptives in women.
The duration of the incubation period is not known exactly, but it has been established that it can vary widely, reaching several years.
Visit our Dermatology page
What is actinomycosis
The content of the article
Actinomycosis is a subacute chronic bacterial infection caused by filamentous, gram-positive, non-acidic, anaerobic and microaerophilic bacteria. The disease is characterized by purulent and granulomatous inflammation and the formation of multiple abscesses and sinus tracts that may secrete sulfur granules.
The most common clinical forms of actinomycosis are cervicofacial (jaw), thoracic and abdominal. In women, pelvic actinomycosis is possible.
3. Symptoms and diagnosis
The pulmonary form of actinomycosis accounts, according to various estimates, from 15% to 50% of all cases; Another common location is the maxillofacial area and neck. There are also abdominal, urogenital, cutaneous forms, actinomycosis of the head, tongue, central nervous system, as well as generalized actinomycosis.
A typical external manifestation is dense red subcutaneous infiltrates with a cyanotic tinge, which, when suppurated and opened, leave long-term non-healing fistulas (fistulas). With actinomycosis of the chest organs, the symptoms may be similar to the clinical picture of tuberculosis: gradual onset, low-grade fever, cough, which after the aproductive period becomes expectorant (the discharge is often purulent or bloody). The course steadily worsens and, if left untreated, inevitably ends in death; Abdominal actinomycosis takes no less threatening forms (mortality without adequate therapy reaches 50%).
Difficulties in diagnosis are caused, as a rule, only by the very early, initial stages of the inflammatory process: in later stages the clinic is quite specific. The diagnosis is confirmed by laboratory bacteriological culture.
A differential diagnosis is made (it is necessary to exclude a malignant tumor process, “true” mycoses, tuberculosis, tertiary syphilis, etc.).
About our clinic Chistye Prudy metro station Medintercom page!
What happens if actinomycosis is not treated?
Inside the tumor, ulcers form, covered with purple, increasingly thinning skin. They gradually approach the surface and then open up. A purulent fluid is released containing fat cells, fibrin and, above all, grains with fungal drusen. If a secondary infection occurs, phlegmon and large abscesses may develop.
Actinomycosis does not spread through the lymphatic tract, but the ulcers can open into the vessels, due to which the fungus penetrates the blood and is carried into all tissues and organs. This picture ends in death. Death occurs from exhaustion or amyloid degeneration, due to the absorption of decay products, and not from the action of a specific poison.
4.Treatment
The main component of therapy is penicillin antibiotics, and if there are contraindications, erythromycin, tetracycline and other alternatives. Some forms are very severe, creating a threat to life, and require intensive long-term (up to a year) treatment, including surgery (opening of infiltrates).
Antibacterial therapy is combined with immunostimulating and immunomodulating. Fortunately, actinomycetes do not exhibit drug adaptation and resistance, but the probability of relapse is quite high, and therefore long-term observation with monitoring of bacterial activity for 0.5-1 year is necessary.
Diagnosis of radiation fungus lesions
Actinomycosis is usually a polymicrobial infection with isolates numbering up to 5-10 species of bacteria. Therefore, detection of this infection in humans may require testing for associated bacteria that are involved in maintaining the disease by producing a toxin or enzymes or by inhibiting the host's defenses.
To recognize actinomycosis, they are guided by the clinical picture and, above all, by the presence of drusen-containing granules in fresh pus, sputum and feces. It is possible to mix with other types of infectious granulomas, namely tuberculosis, syphilis, or true tumors.
Associated bacteria act as copathogens that increase the relatively low invasiveness of actinomycetes. In particular, they are responsible for the early manifestations of actinomycosis and treatment failure.
Actinomycetes: morphology
Actinomycosis is caused by microorganisms of the genus Actinomyces. Previously, pathogens were regarded as fungi, now - as bacteria. The disease they cause is called pseudomycosis. There are several types of actinomycetes that are pathogenic for humans and animals: A. bovis (type species), A. israelii (the most common causative agent of pseudomycosis in humans), A. odontolyticus, A. naeslundii, A. viscosus, etc.
- Aerobic actinomycetes: live in soil, found in water, air and on cereals.
- Anaerobic actinomycetes: are saprophytes. They live on the mucous membranes of humans and animals. They are most pathogenic.
Rice. 3. Threads of mycelium of actinomycetes (photo on the left) and accumulations of Actinomyces Israelii in tissues (photo on the right).
Morphological characteristics of pathogenic actinomycetes
The growth of pathogens located in the tissues of granulomas and exudates is accompanied by the formation of intertwined threads of mycelium - drusen, which are located radially along the periphery (in the form of rays) and have club-shaped thickenings at the ends.
These formations in the pathological material have the appearance of small grains (lumps) of a yellowish or gray color ranging from 20 to 250 microns in size (depending on the age of the colonies).
- Microscopy reveals an accumulation of filaments of actinomycete mycelium in the center of the drusen, and flask-shaped swellings along the periphery.
- When histological material is stained with hematoxylin and eosin, the central part is colored blue, and the flask-shaped thickenings are colored pink. Sometimes there are drusen without flask-shaped thickenings along the periphery. In some cases, drusen do not form.
Actinomycetes occupy an intermediate position between bacteria and fungi. They have a cell wall, like gram-positive bacteria, but, unlike them, they contain sugars. They do not contain chitin or cellulose, are incapable of photosynthesis, do not have flagella, do not form spores, form primitive mycelium, and are not acid-resistant.
Rice. 4. Type of drusen of pathogenic actinomycetes.
Rice. 5. The photo shows densely packed filaments of mycelium of pathogenic actinomycetes.
Cultural characteristics of pathogens
For their growth, actinomycetes require anaerobic conditions (without oxygen). Grows well on protein media. When growing on solid nutrient media, by the end of the first day they form transparent microcolonies, after 7 - 14 days - lumpy colonies that have grown into the nutrient medium, resembling molars in appearance.
Rice. 6. Colonies of actinomycetes on chocolate agar.
Stability and sensitivity of pathogens
Actinomycetes exhibit resistance to desiccation and persist for 1–2 years at low temperatures.
Pathogens are sensitive to high temperatures of 70 - 800 C and die within 5 minutes. Within 5 - 7 minutes they die when exposed to a 3% formaldehyde solution. Sensitive to antibacterial drugs: benzylpenicillin, streptomycin, chloramphenicol, tetracycline, erythromycin, etc.
Rice. 7. Type of colonies of Actinomyces Israelii, the most common causative agent of pseudomycosis in humans.
How the disease develops
Actinomycetes are saprophytes. They are part of the normal microflora of the skin and mucous membranes of humans and animals. Some strains of pathogens, under certain conditions, acquire pathogenic properties and are capable of causing disease (endogenous pathway). In some cases, actinomycetes enter the body through damaged areas of the skin and mucous membranes (exogenous route).
When pathogens invade soft tissues, infectious granulomas are formed, in which accumulations of mycelium of radiant fungi - drusen - are found. Over time, as a result of infection with staphylococci (most often), abscesses develop in the granulations, and when they break through, fistulas are formed. Further, the pathogens, thanks to the production of aggressive enzymes, spread through the subcutaneous tissue, through the bloodstream and through the lymphatic vessels into tissues with a low oxygen content.
As a result of infection, specific sensitization and allergic changes develop in the patient’s body, which leads to the formation of antibodies.
Rice. 8. When actinomycetes invade soft tissues, an infectious granuloma is formed (photo on the left), where accumulations of mycelium of radiant fungi - drusen (photo on the right) are found.
Mycetoma
Mycetoma (maduromatosis or Madura foot) has been known since ancient times. The disease most often occurs in people living in tropical countries. Pathological lesions appear on the foot in the form of several dense nodes, ranging in size from a pea or more. The skin over the nodes is initially unchanged, but then acquires a red-violet or brownish color. Over time, new nodes appear on the foot. The foot swells and increases in size. Over time, its shape changes, and the fingers turn upward. When abscess formation occurs, fistulas appear, from which a purulent mass with an unpleasant odor and a mass of yellowish inclusions is released. The pain syndrome is slightly expressed. As the disease progresses, fistulas begin to appear on the dorsum of the foot. The foot takes on a peculiar appearance - it is deformed and completely riddled with fistulas. Atrophy of the leg muscles is often observed. Without treatment, tendons and bones become involved in the pathological process. Usually one foot is affected. The disease lasts a long time - 10 - 20 years.
Rice. 19. Madura foot.