Chief editor of the site:
Snitkovsky Arkady Alexandrovich
Chief physician of the professorial dentistry “22 Century”, dentist, orthopedic dentist
Author of the article:
Scientific team of dentistry “22 Century”
Dentists, candidates and doctors of medical sciences, professors
Plate prosthesis
A plate prosthesis is the most common of the simple and affordable methods of removable prosthetics for complete or partial absence of teeth. Let's look at the materials and stages of its manufacture.
What is a plate prosthesis made of?
To begin with, let us recall the general requirements for the material:
- No impact on the oral mucosa and the body as a whole;
- Aesthetics;
- High strength, low abrasion;
- Preservation of shape during use;
- Easy to care for;
- No unpleasant taste or smell;
- Must be repairable;
- Must be technologically advanced.
Plate dentures consist of a base (foundation) and artificial teeth. Also, in case of partial absence of teeth, support-retaining elements (clasps) .
The base is made from:
Acrylic plastics
Plastics are polymers that represent a large group of high-molecular compounds obtained chemically from natural materials or by chemical synthesis from low-molecular compounds. One of the properties of polymers is their high manufacturability, the ability to be molded under heat and pressure and stably retain their given shape, which explains their widespread use in orthopedic dentistry. Plastics are made from powder and liquid.
Advantages:
- Affordable price;
- Simple manufacturing technology (various color and size combinations are possible);
- Short production time for the prosthesis;
- Easy to care for.
Flaws:
- With prolonged use of the structure, the material begins to release special substances that can cause a local allergic reaction;
- Acrylic plastics are porous compounds. With poor oral hygiene and poor-quality care of the prosthesis, it becomes contaminated with microorganisms, which helps to reduce local immunity. And this can cause the development of inflammatory diseases of the oral mucosa;
- Possibility of injury to the soft tissues of the oral cavity.
Nylon
Nylon removable dentures
Nylon is an elastic material.
Advantages:
- Hypoallergenic;
- High aesthetics (complete imitation of natural teeth and gums);
- In case of partial absence of teeth, the supporting teeth are not treated;
- The flexibility of the material ensures a short adaptation period and also has the least mechanical impact on the soft tissues of the oral cavity;
- Easy care;
- When used carefully they last quite a long time.
Despite the significant positive qualities, nylon prostheses have their disadvantages :
- The fixing elements do not transfer the load to the remaining teeth. As a result, the mucous membrane takes on the chewing load, which leads to gradual periodontal damage and further inflammatory process;
- The absence of a rigid frame leads to the fact that chewing pressure is distributed unevenly. Subsequently, this leads to atrophy of the bone tissue of the jaws;
- For technological reasons, nylon prostheses are not polished. This design absorbs and retains foreign odors;
- Frequent adjustments are necessary;
- High price.
The material for the base is selected based on the individual characteristics of the body and the condition of the oral cavity.
Indications for use
Indications for the use of prostheses with a metal base can be twofold: general medical (biological) and special. General medical indications include: allergies, bruxism, occupational characteristics, intolerance to plastic prostheses. Special ones include:
frequent breakdowns of plastic bases, multiple, small included defects in the dentition;
- replacement of central or lateral incisors;
- narrowing of the jaws;
- negative attitude towards continuous clasp;
- lack of even one distal support on the upper jaw;
- high attachment of the frenulum of the tongue;
- low clinical dental crowns.
Doctors suggest using removable dentures with a metal base in the treatment of patients with deep bites and maxillofacial patients (after resection of areas of the alveolar processes or jaws).
Features of patient examination. From the anamnesis, it is necessary to find out whether the patient has an allergic background, intolerance to acrylic plastics, whether the patient is undergoing prosthetics for the first time or repeatedly. The patient's feedback on old dentures and their general attitude towards removable plastic dentures are also taken into account.
Artificial teeth
Laminar dentures
For laminar dentures, artificial teeth are made of plastic.
There are frontal (front) and chewing (root) groups, produced in sets in headsets.
Plastic teeth are very similar in appearance to the enamel of natural teeth. During production, you can vary the color and shade. Artificial teeth are firmly connected to the base due to the homogeneity of the material (their connection occurs during polymerization of the base plastic). They are also easy to adjust both by a technician in the laboratory and by a doctor when handing over the prosthesis. Headsets are available in several styles and shades, many combinations are possible. Due to this, it is possible to harmoniously select and manufacture a prosthesis according to the individual parameters of the face.
Over time, the technology for making artificial teeth has progressed.
proposed to produce acrylic artificial teeth using the injection-compression method (continuous injection of material during polymerization to compensate for its shrinkage, followed by compaction of the material to a homogeneous state). This makes them incredibly durable.
The Ukrainian company produces artificial teeth in the form of a set in Estedent, Estedent-02. They have the following positive properties: imitation of the anatomical shape and color of the tooth; high strength indicators; fluorescent effect (both in natural and artificial lighting). Estedent-D is used for prosthetics for children during the period of temporary and mixed dentition.
“Executive” artificial teeth (“Dentsply”, USA) have five distinct shade zones, which will allow you to imitate natural teeth as accurately as possible.
Also in our country, headsets “Megastar” (Great Britain), “Ivoclar” (Liechtenstein), etc. have found use.
When selecting artificial teeth, not only the color of natural teeth (if any) is taken into account, but also the shape of the patient’s face and constitution. Thanks to a wide selection of artificial teeth in color and shape, an individual approach to each clinical case is possible.
Device structure
The base is made of acrylic plastic used for medical purposes. Often a metal alloy is included in the base or reinforcement is made, this allows improving the technical properties of the material:
- the strength of the apparatus increases;
- characterized by high thermal conductivity;
- has increased hypoallergenicity.
The element must have a certain structure that will guarantee long-term operation of the device and make its use more comfortable for the patient:
- for correct, uniform distribution of pressure when chewing;
- the material should minimally adsorb elements of saliva and food residues;
- a base that is convenient for easy and quick cleaning of the material with specialized means;
- strength characteristics must be high;
- the elasticity must also be sufficient, since the material is modeled under the alveolar process of the jaw arch;
- the plasticity of the apparatus should be minimal;
- an increased level of biocompatibility of the material is necessary to eliminate unwanted reactions of the body.
Clasps
Clasp denture with clasps
In case of partial absence of teeth, one of the ways to fix the prosthesis in the oral cavity is the presence of clasps. They are usually made of metal. They tightly cover the tooth, can only serve as a retaining element, and also act as a support, that is, transmit chewing pressure to the tooth. Noticeable when talking and smiling.
Clasps made of elastic material (nylon dentures) can only perform a retaining function. Excellent aesthetics, but unreliable and can become deformed and break.
A systematic approach to the manufacture of complete removable dentures
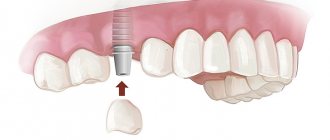
It has historically happened in dentistry that doctors almost never associate complete removable dentures with a high level of aesthetics, and place them at the diametrically opposite end of the pyramid of needs when treating patients with complete edentia compared to other designs. But today, the use of implants has made it possible to combine these two aspects into a single coordinate system. Complete dentures supported by dental implants are a fairly effective treatment option for patients with complete or partial edentia, providing a fairly predictable and successful rehabilitation option. But as Dr. Walter “Jack” Turbifil, DDS, once concluded, “the use of implants will never relieve the dentist of the need to ensure that the prosthesis meets all physiological and mechanical criteria.”
Rehabilitation of a completely edentulous patient poses many challenges. The position of the teeth, aesthetic parameters, phonetic function, occlusal plane, vertical component of the bite and the position of the condyles of the joint are determined according to canonical orthopedic principles. But most of these principles, unfortunately, are leveled out in a state of complete edentia. Even if a patient has been using a certain prosthesis design for some time, it should not be regarded as some kind of referent determinant, since old prostheses are very rarely associated with what the patient actually wants. In addition, during the treatment of patients with complete edentia, the dentist faces psychological problems associated with the patient’s loss of teeth, the development of xerostomia and neuromuscular disorders. This is also one of the reasons why dentists often shy away from treating patients with complete absence of teeth.
The step-by-step analog protocol for the fabrication of complete denture structures has remained virtually unchanged since its invention. Based on the existing impressions, models are cast, on which the technician models the wax base and bite ridges - that’s all. At this stage, proper communication between the dentist and the dental technician is extremely important to correctly determine the proper position of the anterior teeth, transmit data about the vertical component of the bite and the position of the joint. Even if digital technologies are used in the work, the clinician must be able to assess the patient's phonetic function, check aesthetic parameters and correct potential violations in the design of the prosthesis. When using complete denture structures as temporary or permanent restorations, or even as diagnostic structures, the protocol for their production requires a certain level of systematicity in its implementation. The latter should include:
- Registration of the position of the incisal edge of the teeth of the upper jaw
- Registration of the position of the incisal edge of the lower jaw teeth
- Determining the proper vertical bite
- Registration of the central ratio
- Proper installation of plaster models into the articulator
- Phonetic function check
Registration of the position of the incisal edge of the teeth of the upper jaw
The starting point for the manufacture of a complete removable denture is the determination of the vertical and horizontal position of the maxillary anterior teeth. This is achieved by using a sheet of base wax and a wax roller (photo 1).
Photo 1: Maxillary wax ridge with midline and high smile line markings.
The wax bead is contoured and reshaped to conform to surrounding structures, including:
- Horizontal and vertical position of the incisal edge of the teeth of the upper jaw
- Midline of the upper jaw
- Buccal corridors
- Occlusal plane of the maxilla
- High smile line
To check the correct position, you can fix them in a wax base (photo 2). To confirm the correct position of the teeth, the doctor must check the patient’s pronunciation of the sounds “F” and “V”: in this case, the patient must touch the line of transition of the wet part of the lower lip with the dry part with his front upper teeth. To record this position, the doctor may ask the patient to count to 50 or 60 out loud. For diagnostic purposes, the doctor can also obtain photographs of the position of the wax base and teeth at rest, with a high smile, and also in profile. Additionally, you can record several videos of the patient during a conversation, after which all this data can be transferred to the dental technician.
Photo 2. View of the wax roll with teeth 8 and 9 installed.
Registration of the position of the incisal edge of the lower jaw teeth
After determining the proper position of the incisal edge of the maxillary teeth, it is necessary to record the position of the incisal edge of the mandibular teeth. To do this, use a base wax plate and a wax roller (photo 3). The height of the wax ridge in the anterior part of the lower jaw should be 18 mm from the level of the vestibule to the predicted position of the cutting edge of the incisors. In order to eliminate restrictions on the articulation of the lower jaw, the distal parts of the wax roller are made below the occlusal plane, after which cuts are formed on the roller for connection with the wax roller of the upper jaw. In fact, the use of special wax in the projection of the anterior teeth of the lower jaw is the starting point of the next stage - determining the vertical component of the bite.
Photo 3. Using a special portion of yellow wax to test phonetic function with a height of 18 mm from the vestibule of the oral cavity.
Determination of the vertical component of the bite
According to the Academy of Prosthetic Dentistry Glossary of Prosthetic Terms, vertical occlusion is defined as “the distance between two selected anatomical or other marked points (usually one on the tip of the nose and the other on the chin) at maximum fissure-tubercle contact. The classic studies of Dr. Earle Pound demonstrate that the most accurate parameter determining the vertical component of the occlusion is “the height comfortable for normal phonetic function,” since it allows the most open and closed range of tooth relationships during jaw movements to be established, and does not depend on the level achieved bone atrophy or patient age. Recording the bite height that is comfortable for proper phonetic function is done when the patient produces the “C” sound, since the anterior teeth can then be used as a reference point. To pronounce the sound “C”, the lower jaw moves to the closest “conversational” position. The latter corresponds to the contact of the upper and lower incisors edge to edge, or the overlap of the upper incisors with the lower ones by 1.0-1.5 mm. The pure "C" sound is produced when air passes through the formed contact between the teeth.
In order to register the vertical position of the bite, it is the sound “C” that is used, since it is formed by repeated movement of the jaw, regardless of whether the patient has teeth or not. Programming of the muscles for the pronunciation of a given sound is ensured throughout the entire period of formation and growth. The trajectory of this movement depends on the class of skeletal relationships present in the patient. For example, with class 2 skeletal relationships of the lower jaw, you have to overcome a relatively greater distance to pronounce the sound “C” than with class 1.
Once the proper position of the maxillary anterior teeth is recorded, the wax bead is secured to the mandible and the clinician asks the patient to count to 60 or 70. The clinician observes the movements of the mandible and adjusts the lower wax bead until the patient can clearly pronounce the "C" sound. . If, during the pronunciation of the sound “C”, the wax roller of the lower jaw hits the front teeth on the upper jaw, then it can be cut off somewhat. You can also modify the configuration of the cushion in the lingual-vestibular direction (photo 4).
Photo 4: Profile view with the anterior teeth mounted in the upper wax roll and a portion of wax mounted on the lower wax roll to test phonetic function.
Another factor that determines the vertical parameter of occlusion is the available "posterior utterance space". The latter is the space between the back teeth when the lower jaw moves forward to produce the “C” sound. The size of the gap between the posterior teeth will also vary depending on the class of skeletal relationship observed in the patient: in a patient with class 2 relationships, the value will be greater than in a patient with class 1. If, when pronouncing the sound “C”, the back teeth completely touch, this means that the vertical dimension of the occlusion is too large. The method of assessing adequate vertical space for pronunciation, which aims to record the occlusal height parameter, should not be confused with the method of recording free space at the centric relation position. The free space in the centric relation position is the space between the occlusal surfaces of the upper and lower teeth in a state where the mandibular muscles are completely relaxed, while at the same time, when assessing the proper vertical space for pronunciation, the muscles are active. Resting jaw position is highly variable and therefore cannot be used to determine bite height (Figure 5).
Photo 5. Measurement of the vertical component of the bite in a state of occlusion and the height of the bite at rest.
After the doctor has recorded the relationship of the teeth when pronouncing the sound “C”, he can set the vertical occlusion parameter, reducing the vertical space for pronunciation by a few millimeters. If this is not done, then the teeth will contact unphysiologically during the phonetic function.
Central ratio registration
The centric relation is defined as “a maxillomandibular relationship, independent of dental contact, in which the articular condyles contact the thinnest avascular part of the articular discs in an anterosuperior position opposite the posterior slope of the articular eminences.” This provision is repeatable and reproducible. When using complete dentures, it is important to restore the patient's bite in harmony with the centric relation at an appropriate bite height. This minimizes the possibility of developing defective occlusal contacts, which can provoke the development of pain and interfere with the retention and stability of the prosthesis. Before registering the central ratio, it must be initially established by the patient himself. To do this, the doctor performs bimanual manipulation with the load on the condyles with three increasing levels of force (photo 6). After each level of exercise, the doctor asks the patient if there are any signs of tension or pain in the joint area. In the absence of these at each load level, the doctor states that the central ratio position has been achieved. During this diagnostic procedure, wax rollers are not introduced into the patient's oral cavity, since the centric relation does not depend on the contact of the teeth.
Photo 6. Bimanual manipulation technique.
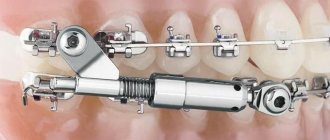
After checking the central ratio, it is recorded using special devices. The most accurate of these is the device for tracing the Gothic arc. This device has a number of advantages, including that it eliminates physical interference on the wax rolls, stabilizes the baseplates, and places the condyles in centric relation during functional movements.
When working with a Gothic Arc Tracer, it is preferable to use a separate set of base plates. The maxillary base plate holds the impact plate (photo 7) and the mandibular base plate holds the pin (photo 8).
Photo 7. Fixation of the impact plane on the wax roll of the upper jaw to control the movements of the Gothic arch.
Photo 8. Fixation of the tracer pin on the wax roll of the lower jaw to control the movements of the Gothic arch.
After placing the base plates inside the mouth, the patient is asked to move the lower jaw back and forth, to the right and then back, to the left and then back. This series of movements is repeated several times and aims to train the patient to deprogram the muscles to ensure the condyles are positioned in centric relation. The impact plate is then covered with a permanent black marker and the patient is asked to perform functional tracing movements again. When the pin is at the intersection of the three tracing lines, the jaw is in the center position (Photo 9). Using a drill, a hole is formed on the impact plate at the intersection of these lines. The patient is then asked to move the mandible back until the pin fits into the socket. With this fixed position, a material is introduced between the plates to register the bite, which will allow fixing the achieved spatial position of the jaws.
Photo 9. Tracing the movements of the Gothic arc: a central ratio is established in the area of intersections.
Fixing models in the articulator
Base plates and wax rollers are also used to correctly transfer the recorded occlusion parameters to the models, which are fixed in a semi-adjustable articulator, also using data from the facebow and the centric relation register. An incision is made on the back of the wax bead so that the bite registration material on the fork forms a monolithic register (Figure 10).
Photo 10. View of the facebow fork with the wax composition of the prosthesis.
First, a model of the upper jaw is fixed in the articulator. After this, base plates are installed with a register of movements of the Gothic arch, which allows for correct alignment of the lower jaw. The articulator pin is installed on the o. After this, the Gothic arc movement tracer is removed and the wax compositions are connected. The articulator pin is adjusted at this stage so that the portion of wax that was used to test phonetic function does not contact the maxillary wax ridge (Figure 11).
Photo 11. Lack of contact between portions of wax material when forming the proper occlusal pattern.
This position of the pin reflects the correct parameter of the vertical component of the bite, which was diagnosed in the patient. Taking this criterion into account, the dental technician places the tooth using a lingualized occlusal scheme to achieve a balance between bilateral balanced occlusion and centric relation. The lingualized occlusal scheme does not involve contact of the anterior teeth, which is why the articulator pin is installed so that the above-mentioned parts of the wax composition do not contact.
Phonetic function check
At the stage of fitting the prosthesis, the parameters of aesthetics and phonetic function must be checked. The patient is asked to pronounce the “C” sound several times and changes in jaw relationship are assessed. This approach helps achieve more predictable and successful results.
conclusions
Rehabilitation of completely edentulous patients is a challenging clinical task. However, by implementing the systematic approach described above, the doctor is able to achieve proper restoration of function, aesthetics and phonetics as a result of the treatment (photo 12).
Photo 12. View of the final designs of complete removable dentures in the oral cavity.
This approach can also be used in the rehabilitation of patients with removable structures on implants, since the adaptive capacity of such is somewhat lower than that of conventional removable dentures, given the stability of the installed intraosseous supports.
Posted by Kimberley D. Daxon, DDS
Stages of manufacturing a plate prosthesis
- Conversation with the patient (it is necessary to clarify complaints, the presence of chronic diseases, allergic reactions, etc.);
- Examination of the oral cavity, assessment of the condition of soft tissues and level of hygiene;
- Additional studies (radiography, tests, etc., if necessary);
- Selection of design;
- Taking impressions from the upper and lower jaws;
- Making a plaster model, then a wax template with bite ridges;
- Trying on in the oral cavity, determining the relative position of the jaws, the color and shape of the teeth, choosing fixing elements (if there are preserved teeth);
- Strengthening models into an articulator, placing artificial teeth on a wax base, placing fixing elements in the base;
- Try-on in the oral cavity, correction if necessary;
- Replacement of wax with the final material, processing, polishing of the prosthesis;
- Fitting in the oral cavity, correction. Recommendations for care.
Plate dentures have proven themselves to be affordable, quick to manufacture and aesthetic designs.
Date of publication: September 20, 2020 Last update: September 22, 2022 © 2020 Professorial Dentistry “22 Century”. All rights reserved.
Advantages
The metal base is more durable, and the structure can serve its owner for many years without losing its performance properties. This prosthesis has other advantages:
- Reasonable price;
- Prevention of gum diseases;
- The ability to combine prosthetics with dental treatment;
- Easy maintenance of the structure;
- Possibility to leave the denture in the mouth overnight.
The prosthesis is fixed in the mouth using clasps or attachments. Clasps are hooks attached to the very base of the supporting teeth.
Fixing creams
It is especially worth noting that in some cases, the system of prosthetic care products includes fixing agents, especially when the prosthesis has just been installed and one is getting used to it. This helps solve a number of physiological and psychological problems. Retention devices also give a person confidence that the denture will not fall out of the mouth. Fixation means are selected depending on the individual characteristics of the patient.
Doctor - dentist - orthopedist of the Dentalika clinic Belov S.A.
Dear Colleagues! When copying information, placing a link to the source site is mandatory!