What is a stump tab
A stump inlay is a microprosthesis, which is a dental abutment made of metal, ceramic or zirconium dioxide. It is used in case of significant destruction of the crown part of the tooth and intact root. The prosthesis fills the resulting void and creates a support on which an artificial crown is applied. Before installing the inlay, the tooth must be cleaned.
A stump inlay on a tooth is one of the reliable methods of prosthetics. Thanks to a well-sealed channel and the choice of high-quality materials (such as gold), it can last up to 15-20 years.
Orthopedic dentistry has a number of requirements for the use of inlays:
- absence of purulent-inflammatory process around the root;
- the dental canals must be well passable along the entire length of the pin;
- the root stump should protrude above the gum, the walls should be of sufficient thickness (at least 2 mm).
The decision on the treatment method is made by the doctor after X-ray diagnostics, taking into account how much the tooth tissue is destroyed, how long it will take to develop the root canals for the pins, what kind of load will be on the tooth, that is, will it serve as a support for the prosthesis or is it a one-time restoration.
Manufacturing technology of stump inlays
- Layering ceramics. After receiving the impressions, a refractory model is made, a ceramic pin is firmly installed in the canal, ceramic is applied and fired. In the process of applying ceramic layers, you can choose different colors and shades of material, dyes and modifiers.
- Production of ceramics by pressing from tablet molds. The liner is modeled from wax, the sprues are installed in the direction of the ceramic flow. Using a silicone ring, a lining material is inserted and a limiter is placed. Pressing takes place in an oven equipped with a microprocessor control system. The resulting product after pressing and casting is a solid single crystal, the abrasion of which is comparable to the natural abrasion of hard tooth tissues.
- Manufacturing using CAD/CAM method. Allows you to create prostheses and parts that match the implant, abutment, and abutment shape. The device is scanned in the oral cavity or on a model, 3D modeling is performed using a special program, the information received is transferred to a drill, which mills the product under computer control. An accurate and sophisticated method that requires high costs for professional training of personnel to operate the equipment.
- Injection molding method. Casting a working model from plaster / polyurethane, choosing an ashless pin according to the type of root canal, applying silicone varnish to the root. The pin is inserted into the canal and an ashless plastic/wax modeling is performed. After a control check, the cast abutment inlay is removed and transferred to a metal casting. The method is technologically advanced, economical, requires a minimum of material costs, but is very sensitive to the quality of the casting. With strict adherence to all norms and rules, reliable and high-quality microprostheses are obtained.
Materials for manufacturing stump inlays
- Metal stump tab. The metal abutment inlay can be made of an alloy of chromium and cobalt, there are also inlays in a silver abutment and inlays in a gold abutment. They are reliable, but not aesthetically pleasing, which is why in modern dentistry gold supporting inlays and silver microprostheses are used quite rarely and only for chewing dentures.
- Metal-ceramic liner. A metal-ceramic abutment inlay is quite durable, but its quality is worse than that of inlays made from other materials due to the difference in the thermal expansion of metal and ceramic. Therefore, such microprostheses often fall out.
- Ceramic inlay. The ceramic abutment insert best preserves the aesthetics of a smile, since ceramics in its properties and appearance are as close as possible to natural tooth enamel. Therefore, the abutment tongue on the front tooth is made from this material.
- Zirconium stump inlay. The advantage of such structures lies not only in their high strength, but also in the white color of the abutment insert made of zirconium dioxide, which is not visible through the crown. Therefore, as an answer to the question “Which abutment inlays are better?” Together with a ceramic inlay, we can safely call an oxide or zirconium dioxide inlay a pin. Therefore, the anterior tooth stump can also be made of zirconium.
- Composite stump inlay. The type of inlay is suitable for a stump with a pin, which adheres better to the tooth tissue than others, but is not strong enough compared to inlays made from other materials.
Hypoplasia and hyperplasia
These are rare congenital pathologies. With hypoplasia, the enamel is underdeveloped or absent altogether. With hyperplasia, its quantity, on the contrary, is excessive. Such disorders arise due to metabolic failure, general pathologies of fetal development, diseases of the gastrointestinal tract, as well as health problems that arise in women during pregnancy. Usually the problem of hyper- and hypoplasia is solved in childhood by removing “extra” or replenishing missing hard tissues. Sometimes those who had congenital hypoplasia may require more frequent remodeling therapy in adulthood.
Types of stump inlays
Collapsible and non-collapsible
Non-separable is a one-piece structure containing one abutment and 1-2 supports in the channels. Unbendable ones are often made by casting, so they are very strong and durable. They are used to restore teeth with one or two canals.
Collapsible - used in multi-rooted teeth with two or three root canals. The design consists of several pins fixed in the channels. The products are used when, due to the complex anatomical structure of the tooth, it is impossible to cast an inlay. The process of creating and pinning folded cards is more complex, but effective. Therefore, structures are widely used to restore teeth that have been destroyed by more than 50%.
Single-channel and multi-channel
Depending on the number of channels, designs are: single-channel, two-channel, three-channel and four-channel. The latter are used quite rarely; often 2-3 pins are enough to restore even a large molar. Products in 1-2 channels are cast structures made of various materials. Tabs with 3-4 channels are often made foldable. They are made from metal alloys.
Inlays for front and chewing teeth
In the frontal region, the teeth have a root, so single-rooted teeth are used for treatment. The front teeth are visible when smiling and talking, so aesthetic materials are used to make products - ceramics, fiberglass. They are light or transparent, completely hidden from others. Such tabs do not spoil the appearance, do not shine over time and do not cause inconvenience.
Products for chewing teeth can have a different number of pins - from 1 to 4. A variety of materials are used for their manufacture. The choice of design should be made by a specialist, taking into account the wishes of the patient and the individual characteristics of the clinical situation.
Orthopedic treatment of tooth crown defects using inlays
For several decades, the search for optimal ways to replace defects in the crown of the tooth has been ongoing. The development of technology constantly tilts the scales, which tilts towards either therapeutic or orthopedic techniques. Our goal was not to conduct a comparative analysis of various methods for restoring crown defects. This publication is devoted only to illustrating certain recovery methods that, in our opinion, deserve attention.
The main method of eliminating defects in the crown of a tooth, especially in the initial and middle forms, is undoubtedly filling. Dental filling compared to prosthetics is a less labor-intensive process, which consists of surgical removal of the affected tissue, medicinal treatment of the cavity and filling the defect with filling material. However, this method of treatment, even at the modern level of development of dentistry, cannot always provide a solution to the problem of restoring the shape and function of teeth, especially with carious defects of classes II, IV of the Black classification, systemic hypoplasia, increased abrasion, hereditary disorders and malformations of hard tissues, etc.
The significant and most characteristic disadvantages of fillings include, first of all, secondary caries and loss of fillings (Abolmasov N. G. et al., 2003). M. B. Bushan and V. N. Kopeikin note that filling materials have a lower coefficient of wear resistance compared to metal and porcelain. They may be porous and not strong enough. Therefore, interest in alternative types of treatment and, in particular, in replacing tooth crown defects with inlays is quite justified.
Inlays are called microprostheses used to restore defects in the coronal part destroyed as a result of carious and non-carious lesions. Unlike a filling, the tab is inserted into the prepared cavity not in a plastic state, but in a solid state. This avoids shrinkage that occurs when the filling material hardens, and therefore improves the marginal fit and reduces the frequency of caries relapses.
The design of the inlay is selected taking into account the topography, shape, size of the defect, anatomical and topographic relationships of hard and soft tissues, type of bite, direction of loads, tooth inclination, radiographic results, presence or absence of pulp. Depending on the material from which the inlays are made, they are divided into: a) metal (gold 900, 750, cobalt-chrome alloy, silver-palladium alloy, titanium alloys, for example VT5L); b) non-metallic (porcelain, composite); c) combined metal-ceramic and metal-composite (Fig. 1).
Rice. 1a. Inlay made of 900-carat gold alloy.
Rice. 1b. Inlay made of 900-carat gold alloy.
For a number of years, the main structural material for inlays has been gold alloys. The method of manufacturing a cast inlay using a wax model was described by Taggart in 1907. Since then, the technology has undergone certain changes, but the high strength characteristics and accuracy of the fit of the gold inlays to the walls of the cavity, maintaining a constant volume, protecting the edges of the enamel from chipping, inertness, non-oxidation in the oral cavity, the ability to unravel during chewing and better adapt to the walls of the cavity.
In connection with the increasing requirements for the aesthetics of restorations and constantly improving technologies for the manufacture of dentures, one of the most promising areas is the prosthetics of partial defects in the coronal part of the tooth with ceramic inlays. The current level of development of dentistry makes it possible to produce these structures in the following ways:
- firing on foil;
- firing on a fireproof model;
- production of a ceramic frame by firing on a refractory model, followed by cladding;
- production of ceramic inlays by pressing;
- manufacturing a frame from aluminum oxide and zirconium dioxide by electrophoretic deposition with subsequent lining;
- manufacturing the inlay frame by ultrasonic condensation of aluminum oxide with the addition of zirconium dioxide, followed by layer-by-layer application and firing of porcelain;
- firing of the aluminum oxide frame followed by cladding;
- milling using a computer program.
The technology for manufacturing ceramic dentures by hot pressing is implemented using the IPS-Empress I, II systems. One of the advantages of these systems is the use of fluorapatite as a structural material, which, compared to other ceramic materials, causes less abrasion of natural antagonist teeth (Fig. 2).
Rice. 2a. Porcelain inlay made by pressing (painting technique).
Rice. 2b. Porcelain inlay made by pressing (painting technique).
Initially, the IPS-Empress I system provided for the complete reconstruction of the anatomical shape of the coronal part of the tooth from wax and the subsequent simultaneous hot pressing of the ceramic mass. Thus, the finished restoration was monochrome, with a high degree of transparency, since porcelain of the same color was used. Color correction was carried out by applying dyes before glazing, which did not always make it possible to optimize the color rendition of the restoration with the individual coloring characteristics of natural teeth (coloring technique).
Ivoclar specialists continued to work on this issue, which was reflected in their later developments. When working with the IPS-Empress II system, you can create a wax model of the base of the inlay with subsequent pressing. Subsequently, dentin and enamel masses are applied to the model on the frame, ceramics are modeled and fired (layer-by-layer porcelain application technique).
The manufacture of the inlay frame by ultrasonic condensation of aluminum oxide with the addition of zirconium dioxide, followed by layer-by-layer application and firing of porcelain involves the introduction of a suspension of the VITA In-Ceram ZIRCONYA material into the cavity of the double model of the prepared tooth, compacted in a Vita Sonic II type apparatus, drying, and correction of the shape of the inlay base , glass infiltration and firing. After trying on the base in the oral cavity, it is veneered with ceramic mass (Fig. 3).
Rice. 3a. Ceramic inlay made using ultrasonic condensation technology of VITA In-Ceram ZIRCONYA material, followed by firing and layer-by-layer application and firing of ceramics.
Rice. 3b. Ceramic inlay made using ultrasonic condensation technology of VITA In-Ceram ZIRCONYA material, followed by firing and layer-by-layer application and firing of ceramics.
Rice. 3c. Ceramic inlay made using ultrasonic condensation technology of VITA In-Ceram ZIRCONYA material, followed by firing and layer-by-layer application and firing of ceramics.
The most interesting direction may be related to milling a ceramic block using a computer program. Since the early 90s, zirconium oxide has been increasingly used in dentistry. According to in-vitro studies, zirconium oxide denture frames have high tensile strength comparable to that of metal alloys. The introduction of CAD/CAM technology in dental prosthetics makes it possible to produce structures with high accuracy and predictably reproducible quality. Based on the general user algorithm and hardware layout, CAD/CAM systems can be divided into 3 main groups:
- Centralized macrosystems (Procera, Decim).
- Individual mini-systems (Hint-Els, Precident).
- Custom microsystems (Cerec).
The use of modern computer technologies can significantly increase the accuracy of restoration manufacturing and minimize the influence of the human factor. However, most of the well-known CAD/CAM systems are expensive, which limits their distribution in the dental market. A number of inventors set out to create compact and inexpensive milling equipment that makes it possible to produce extended structures from zirconium oxide (Fig. 4).
Rice. 4a. Manufacturing of inlays using copy-milling technology and a zirkonzahn machine.
Rice. 4b. Manufacturing of inlays using copy-milling technology and a zirkonzahn machine.
Rice. 4c. Manufacturing of inlays using copy-milling technology and a zirkonzahn machine.
Rice. 4g. Manufacturing of inlays using copy-milling technology and a zirkonzahn machine.
One of them was Enrico Steger, inventor, owner and CEO of Zirkonzahn. The operation of his system is based on copy-milling technology. First, a prototype of the product is created from a light-curing composite material, then it is milled from a zirconium oxide blank in a copy-milling machine.
To facilitate this process and reduce wear on grinding tools, the Zirkonzahn machine works with an unsintered (pre-agglomerated) form of zirconium dioxide. The zirconium oxide inlay blank is 25% larger than the composite counterpart, since further firing of the product will lead to significant shrinkage of the material. The author managed to calculate these volumetric changes and transfer them with high accuracy into the basis of the operation of his copy-milling machine.
Along with the above-described methods for making inlays, restoration of defects in the coronal part of the tooth is also currently used using inlays made of light-curing composite materials. Compared to porcelain and metal-ceramic inlays, composite inlays have a less abrasive effect on natural teeth; due to the elasticity of the composite, they absorb part of the occlusal load, are less labor-intensive to manufacture and do not require expensive bulky equipment and specially trained dental technicians, and can be easily restored in the oral cavity. , much cheaper.
The disadvantages of composite inlays include insufficient color stability, the possibility of allergic reactions to the composite, and the abrasion of modern composite materials, although close to the abrasion of tooth enamel, is somewhat higher, which can lead over time to a decrease in the height of the lower third of the face in the position of central occlusion with multiple restoration of lateral teeth, with single restorations - to the development of deformation of the occlusal curves. Composite inlays have lower strength, greater porosity, and, compared to porcelain and metal ones, are characterized by less tolerance to the gingival margin, but despite this, they can be a serious alternative to direct restorations (Fig. 5).
Rice. 5a. Stages of tooth restoration using a composite inlay.
Rice. 5 B. Stages of tooth restoration using a composite inlay.
Rice. 5th century Stages of tooth restoration using a composite inlay.
Rice. 5g. Stages of tooth restoration using a composite inlay.
Rice. 5d. Stages of tooth restoration using a composite inlay.
Rice. 5e. Stages of tooth restoration using a composite inlay.
The development of dentistry at the present stage is characterized by the rapid growth of new technologies for the manufacture of dentures. And it’s quite difficult for a dentist to navigate this diversity. We hope that this publication expands the horizons of choosing restoration techniques for defects in the coronal part of the tooth.
LITERATURE
- Abolmasov N. G. Replacement of defects of teeth and dentition with fixed dentures N. G. Abolmasov, N. N. Abolmasov, V. A. Bychkov, V. R. Shashmurina. - Smolensk, 1995. - 175 p.
- Bragin E. A. Fundamentals of microprosthetics. Pin structures of dentures, inlays, veneers, artificial crowns, decorative dental onlays. / E. A. Bragin, A. V. Skryl. - M.: Medical press, 2009. - 508 p.: ill.
- Volvach S.I. CAD/CAM technologies in the dental laboratory - myth or reality? / S. I. Volvach // New in dentistry for dental technicians. - 2000, No. 4 (12). - P. 3-13.
- Dyakonenko E. E. Orthopedic treatment with metal-free ceramics as an alternative method of tooth restoration / E. E. Dyakonenko // New in dentistry for dental technicians. - 2000, No. 1 (9). - P. 3-14.
- Prosthetic restoration of teeth. CEREC system. Textbook, ed. prof. V. N. Trezubova, S. D. Arutyunova. - St. Petersburg: Spetslit, 2003. - 64 p.
- Skryl A.V. Restoration of defects in tooth crowns with ceramic inlays / A.V. Skryl // Modern orthopedic dentistry. - 2008, No. 10. - P. 46-48.
- Steger E. ZIRKON milling technology / E. Steger // Dental technician. - 2007, No. 4. - P. 33-41.
Why core inlays are better than fillings and pins
Fillings and pins are only applicable if the tooth has a sufficient amount of healthy tissue. If only the root or thin walls of the tooth remain, it will not be possible to restore it with a pin, since this restoration method will not differ in either quality or reliability.
Firstly, under load, the pin can break and damage the tooth root. Trauma to the root of a tooth is a direct indication for its removal; In case of damage to the root system, no technique will help save the tooth.
Secondly, dentures installed on large fillings and pins are more likely to fall out some time after prosthetics. In this case, the treatment will have to be repeated, and this entails new significant financial costs.
Important: Some dentists try to cement a fallen crown and post using cement. But this is useless - the structure will not hold firmly and, moreover, an inflammatory process can begin under it, which leads to caries.
Therefore, in the case of severe caries, only an abutment inlay can provide high-quality and durable prosthetic results.
Let's sum it up
When a carious lesion occurs, it is important to understand why dental inlays are needed, why they are better than a composite filling, and when they are contraindicated. It is important to understand that installing such structures is not always advisable and in some cases can lead to complications, which are much more difficult to get rid of than preparing a cavity and pouring filling material into it or installing a microprosthesis on cement.
Before starting treatment, you need to choose a good doctor who will prescribe diagnostic procedures, carefully study the research results and give recommendations during the recovery period. Although almost the entire process is automated, the participation of a professional orthopedist is the key to quality therapy without unpleasant consequences.
Specialists provide a full range of dental and orthopedic services, advise patients and offer optimal solutions to problems. Sign up for a consultation by phone or leave a request on our website, and we will contact you as soon as possible.
Indications and contraindications for the installation of stump inlays
Installation of dental inlays is indicated in the following cases:
- crown inlay for prosthetics;
- fracture of the crown of the tooth;
- carious destruction of the crown;
- abnormalities in the position, shape or size of the tooth;
- low dental crown;
- production of a bridge prosthesis, when the stump inlay for the tooth is used as a supporting element;
- need for splinting.
The strength of fixation, quality of construction and durability of the product depend on the condition of the tooth root when a microprosthesis is installed into it. The root should not wobble, it should be free of curvature in the upper third, with passable and well-sealed canals and walls of sufficient thickness for prosthetics. The use of an abutment design is not recommended in the following cases:
- circular ligament damaged;
- resection of the root apex (temporary relative contraindication), as well as inflammatory processes that can injure the gums or root tissues;
- poor hygiene;
- incomplete obturation of the canals;
- mobility 3 degrees.
In each clinical case, the decision to place an abutment design is made by the treating orthopedic surgeon together with the relevant specialists, taking into account all the advantages and disadvantages of using this reconstruction. If there are relative (temporary) contraindications, therapeutic or corrective surgical treatment, as well as replacement of incompetent orthopedic structures, can be performed before prosthetics.
Tooth preparation
Before installing core inlays, the tooth must be properly prepared, that is, undergo endodontic treatment
.
The canals of the tooth must be properly sealed
. The quality of the filling can be checked by x-ray examination. Next, oddly enough, the canals are unsealed to 1/2 - 1/3 of the root length. In other words, a bed is being prepared for the stump insert. The channel is given a certain taper and width. Then a silicone two-layer impression is taken, imprinting the ideal shape of the inlay. Impressions are taken from both the upper and lower jaws, since during production in the laboratory it is necessary to understand the relationship of the antagonist teeth and jaws so that the coronal part of the inlay has the required inclination, size and shape.
The tab is then fixed with cement. A day after fixing the tab, impressions can be taken for further crown manufacturing.
With high-quality and correct restoration of teeth using core inlays
, “missing” teeth, as it already seemed, will serve for many more years, fully performing their functions.
The description and photo for this clinical case were provided by ViTerra orthopedic dentist Z.E. Kadiev.
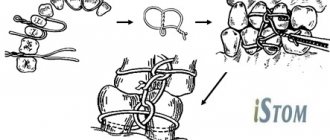
The procedure for manufacturing and installing the stump tab
Production and installation take place in several stages:
Preparation
It includes an examination, consultation, treatment plan and selection of an appropriate design. At this stage, the oral cavity is disinfected and the roots are prepared for dentures. Next, the doctor takes impressions of the tooth, since the pins of the structure must accurately follow the shape of the root canals. The impressions are sent to a dental laboratory for subsequent production.
Production
A dental technician makes plaster and wax models. Based on the models, make an insert insert from the selected material, taking into account the specifics of the manufacturing technology.
Installing a tab
During the follow-up examination, the doctor prepares the root canals and fills them with dental cement. For better fastening, the studs of the structure are pressed forcefully into the solution.
Preparation for prosthetics
The specialist makes repeated impressions for the subsequent production of the crown.