Correction of bite in children is carried out in several ways. The likelihood of a favorable outcome increases if parents noticed the anomaly in time and showed the child to a specialist. Treatment is selected depending on the type of pathology and the reasons for its formation. It is better to start it before the final period of bite formation (growth of molars) begins.
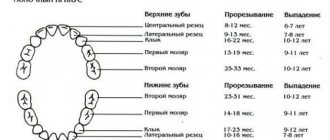
Pediatric dentistry is required from the appearance of the first teeth. The child should undergo the first examination by a pediatric orthodontist at the age of two, since during this period baby teeth are formed. The next visit to a specialist is necessary at the age of mixed dentition, which corresponds to the child’s seven to nine years of age. Upon reaching the age of fifteen, visits to the dentist-orthodontist should become annual.
Types of dental malocclusion in children
Bite correction is necessary for children with obvious disorders of chewing function. These include the following types of anomalies:
- Open. Affects molars, premolars and incisors. The upper and lower jaws do not meet.
- Cross. Diagnosed in children at 6-7 years of age. In this case, the child’s lower jaw moves forward and overlaps the upper jaw.
- Deep. The type can be confused with distal occlusion. The child's speech is impaired and his gums are often injured. When chewing, the teeth of the lower row touch the upper jaw: the incisors almost completely overlap each other.
- Mesial (progeny). In this case, the child’s lower jaw is strongly pushed forward. The development of an anomaly can be triggered by heredity.
- Distal. Children most often suffer from prognathia in preschool age. Their chewing muscles are poorly developed, so the upper jaw hangs over the lower jaw.
Pathology can be recognized by the following signs:
- unclear speech;
- impaired breathing, especially during sleep;
- non-closure of the lower and upper canines;
- overlap of the lower jaw with the upper;
- lingual or vestibular tooth growth;
- curvature of bone tissue;
- inward displacement of the jaw.
Treatment can begin after identifying the exact causes of the pathology.
Types, types and forms of deep bite
The type of bite is determined by the level of overlap of the lower teeth:
- Mild degree.
The lower teeth are half visible.
- Average.
The lower teeth are 50–100% invisible.
- Severe degree.
The upper incisors cut into the soft tissue of the lower jaw, completely covering the lower teeth.
There are two types of deep bite:
- Distal.
This is the most common type of deep bite. With it, the lower jaw is slightly shifted back, and the lower teeth are not visible by approximately 1/3. The relationship of the distant teeth is disturbed. The patient has difficulty biting, chewing, nasal breathing, and sometimes experiences pain in the temporomandibular joint.
- Neutral.
With such a bite, the upper incisors also overlap the lower ones by 1/3, but the lateral teeth remain in place and their relationship does not suffer.
There are such forms of deep bite:
- Roof-shaped.
The upper front teeth protrude strongly forward, overlapping the lower ones.
- Blocking.
The upper incisors overlap the lower ones and are inclined backwards.
Causes of malocclusion in children
Predisposing factors influencing the formation of malocclusion in a child:
- loss of baby teeth or delay in their growth (removal of baby teeth should only be performed by a dentist);
- diseases that developed in the womb;
- poor posture in a child;
- vitamin or mineral deficiency;
- diseases of the upper and lower respiratory tract;
- improperly started complementary feeding;
- congenital anomalies (narrow jaw);
- finger sucking in sleep;
- improper grip of the bottle or mother's breast;
- genetic factor.
If a child is given solid food late (fresh fruits, vegetables, nuts, sunflower seeds), then the risk of developing an anomaly is quite high.
What happens if you don't correct a deep bite?
Complications of uncorrected deep bite:
- loosening of incisors,
- cracks and chips on the front teeth,
- abnormally rapid and uneven wear of enamel (especially lateral teeth),
- sensitivity of the anterior incisors to cold and food,
- gradual protrusion of the upper incisors,
- wedge-shaped defects.
Such defects appear due to the strong pressure of the lower front teeth on the upper palate.
There are also complications that do not directly affect the condition of the teeth:
- Trauma to the mucous membrane of the palate.
Constant friction of the lower incisors against the upper palate provokes persistent wounds. But the mucous membrane must constantly renew itself, which is why an excessive number of new cells appear. This, in turn, increases the risk of mutations and cancer.
- Disorders of the temporomandibular joint.
The patient can move the jaw limitedly, the muscles are stiff. People often experience pain in this area, hear crunching or clicking noises when chewing, and suffer from migraines. If this is not corrected, over time the patient will experience degenerative processes in the joint.
Exercises to correct your bite
After identifying malocclusion in children, the doctor may prescribe myogymnastics. The therapy is aimed at restoring muscle motor activity, training the tongue and lips. To correct a child’s bite, it is necessary to achieve myodynamic balance: the strength of the muscles outside and inside the oral cavity must be equal. The development of facial and dental pathologies can provoke weakening of muscle tissue.
A set of therapeutic exercises:
- Massage your lower and upper lips with your index finger for 3-5 minutes. The exercise must be repeated several times a day.
- Connect 2 large buttons with a cord. The child must hold one of them with his teeth, and the second he must pick up and stretch the lace. Do 10 approaches.
- Pull out your lips with a tube. Forcefully inhale and exhale air through your mouth. Repeat the exercise several times.
- Purse your lips tightly and draw air into your mouth. Press your fingers on the swollen cheeks, do 5-7 approaches.
- The lips, stretched out like a tube, should be compressed and unclenched with force. Perform the exercise for 2-3 minutes.
- Move the lower jaw forward as much as possible, and try to reach the upper lip with your teeth. Fix the position for 2-3 minutes.
- Place a plastic ruler between your lips and press on the opposite edge with your finger.
- Hold the plastic card between your lips and hold the position for a few minutes.
Tongue exercises are best done after gymnastics. These include:
- counting teeth from the inside;
- stroking the soft and hard palate with the tongue;
- clicking.
If a child has one or more teeth growing incorrectly, they can be gently pressed with the tip of the tongue from the inside for 2-3 minutes. To strengthen the cheek muscles, the child should take water into his mouth and hold it for several minutes, then spit it out. To practice breathing, experts recommend alternately pinching first the left, then the right nostril.
The technique has age restrictions. Treatment can begin at 3 years of age. Playing the trumpet and other wind instruments and blowing soap bubbles through a plastic tube or straw will help train your muscles.
Causes
A child's malocclusion may have hereditary roots. If parents' jaws are anatomically incorrect, most likely their child will experience the same thing. Bite abnormalities appear gradually. In infants, the jaws consist mainly of the alveolar process, and their basal parts are still underdeveloped. At the same time, the bones of the upper jaw grow faster than the lower jaw, and the lower jaw has two halves that fuse when the child turns 1 year old (on average).
The jaws change, which is reflected in the bones and muscles, including the temporal, chewing and pterygoid. The most developed muscle in babies is the chewing muscle, because they need it to suck on their mother's breast. But the lateral and medial pterygoid, as well as the temporal muscles, thanks to which the lower jaw moves up and down and back and forth, are poorly developed during this period. And after the first teeth have erupted, they begin to actively develop. A child from 1 year of age begins to experience malocclusion.
Factors that influence bite problems in children:
- artificial feeding of a newborn (sucking a bottle is easier than extracting milk from the mother’s breast, therefore the muscles of the jaw and face develop less than they should at this age)
- use of a pacifier up to 1.5-2 years (during this period the baby is teething)
- after the eruption of primary molars, the child’s diet lacks food that must be chewed before swallowing
- baby's habit of holding and sucking fingers or toys
From 5-7 months of life, the child’s upper central incisors are also cut. This is the beginning of the formation of the baby rows of teeth. In cases where the upper jaw is more developed than the lower jaw, or the teeth are small, the spaces between the teeth (three teeth) can be more than 1 mm in size. This is a signal of future problems with the child's bite.
When a baby turns 3-4 years old, the bone structures of his teeth and jaws are actively forming. From the age of 5, the gradual resorption of the roots of baby teeth and the growth of the alveolar processes of the jaws begin. From the age of six, baby teeth fall out and molars grow in their place.
Orthodontists call replacement teeth those that a child has until the age of 13-14 years. During the same period, the size of the jaws also changes, because their basal part is actively growing. If deviations occur during this period, they may precede a malocclusion. The twisting of individual teeth relative to their axis or erupting them in the wrong place is almost a guarantee that the child will develop a malocclusion. Violation of occlusion in children has a main cause - an anomaly in the shape of the dental arches.
The cause of malocclusion may be hidden in the syndrome of chronic difficulty in nasal breathing in various diseases of the ENT organs or congenital pathologies of the nasopharynx and nasal septum:
- enlarged adenoids
- polypous rhinosinusitis
- sinusitis
- rhinitis
With such pathologies, the child breathes through his mouth, even in his sleep. Therefore, the muscles responsible for lowering the lower jaw do not relax at night, the upper jaw is pulled forward, and therefore the bite is disturbed. The proportions of the face change, which is called the adenoid type of the child’s face.
Endocrinologists say that bite defects can be a consequence of functional disorders of the thyroid and parathyroid glands. In particular, due to a lack of production of thyroxine and thyrocalcitonin, bone growth is delayed. The maxillofacial bones also grow poorly, and the child’s baby teeth are cut slowly and belatedly. When the parathyroid glands are underdeveloped or diseased, the production of parathyroid hormone, which regulates calcium levels in the body, is disrupted. Impaired calcium metabolism causes demineralization of bone tissue, which can cause the jaws to lose their normal anatomical shape and location.
Treatment of malocclusion in children
Treatment of pathology with radical methods involves installing braces and wearing orthopedic structures (mouth guards, plates). With their help you can straighten your teeth. You can also use a device to correct bites in children - a trainer. It is selected depending on the age of the child.
Up to 2 years of age, children are given anatomical attachments on their bottles that are shaped like a nipple. They vary depending on the type of food, size, number of holes and age of the child. Based on the diameter of the holes there are:
- L - nozzle with a wide hole for purees or thick soups;
- M - a medium-sized hole through which liquid porridge or milk mixture passes;
- S - with a small hole for juices and milk.
For children over 4 years old, the bite can be corrected with vestibular shields. With their help, they strengthen muscles and get rid of bad habits (sucking fingers or household objects). The shield fits tightly to the surface of the teeth and improves the degree of their closure.
Oral shields are installed for children over 5 years of age. The simulator returns the normal position of the tongue, prevents the jaw from moving forward and helps to relax the muscle tissue.
Children over 7 years old are fitted with passive dental appliances. They consist of several parts:
- an arch made of metal (for the front teeth);
- clasps (retaining and supporting elements);
- springs (located in the middle part);
- base (made of plastic).
The principle of operation of this device is based on the ability to expand the upper jaw and stimulate the growth of its apical base.
The Klammt device will help correct mesial or distal occlusion. It promotes protraction of the lower jaw and tilting of the lower canines in the desired direction. If the child does not have incisors, the device is not installed.
Distal bite – correction with braces
Correction of distal occlusion with braces gives good results in adolescence and adulthood. If you are concerned about the aesthetic issue, then you can choose a lingual system. In this case, braces are placed on the inner surface of the teeth.
- Lingual braces are more expensive, but they correct the bite better and faster. The most important thing with lingual braces is regular oral care, since pieces of food can accumulate under braces. If you do not clean your mouth properly, caries appears and your teeth begin to deteriorate. You need to go to the dentist every four weeks.
- Metal braces are most often used to correct malocclusion. They are worn without taking them off. You also need to take care of your oral cavity carefully, brush your teeth in the morning and evening, and clean the plates with a special brush.
- Ceramic braces are not as noticeable as metal braces. The arch of ceramic braces is nylon or metal.
The first four weeks a person should get used to braces. In order not to injure the oral mucosa and ensure patient comfort, medical wax is applied to the sharp parts of the plates. The duration of wearing is from six to twenty-four, it all depends on the severity of the disease.
There are few contraindications for wearing braces, but they need to be taken into account:
- Immune pathologies.
- Tuberculosis open and closed form.
- Oncology of any form.
- Endocrine diseases.
There are no more restrictions. If braces do not correct the bite, then surgical treatment methods are used.
When does a child need to have their bite corrected?
You can be of any age to correct your bite. Treatment can begin at 3-4 months. You can notice a malocclusion in an infant by abnormal breathing: it is often difficult. During feeding, you need to pay attention to the position of the baby's head: it should not be thrown back or pressed with the chin to the chest.
In children under 2 years of age, the facial muscles are poorly developed, so it is impossible to recognize an incorrect bite without consulting a specialist. In this case, hardware techniques are not used; the child can be prescribed physiotherapeutic procedures and massage.
In children over 5 years of age, disorders are clearly visible. The child's speech may be impaired, as well as chewing function. The defect can be seen upon visual inspection: the teeth grow incorrectly (displaced, crowded). The child has asymmetry of the jaw or face (partial closure, protruded lower or upper jaw).
If the molars grow incorrectly, the child may complain of headaches, constant biting on the inside of the cheeks and clicking in the temples.
Surgical treatment
Correction of distal occlusion surgically is carried out in cases where conservative methods are powerless. For example, with complex jaw deformities, or very noticeable defects.
Problems with bite provoke gastrointestinal diseases and speech defects, so the pathology cannot be left without treatment. The operation to correct the bite is multi-stage and complex and is performed under general anesthesia.
First, the doctor does computer diagnostics and modeling, and only then the operation is prescribed. During the process, the orthodontic surgeon corrects the jaw bones into an anatomically correct position. Then he fixes it using devices. Next, a special splint is applied, which the patient must wear for two weeks. The duration of the process varies from one to seven hours, it all depends on the complexity of the case.
Prevention of malocclusion
Preventive measures begin almost immediately after the birth of the child. Experts recommend following a number of recommendations:
- Gently massage lips and cheeks;
- use orthopedic attachments that form the correct bite;
- introduce solid foods into the diet in a timely manner;
- When baby teeth appear, gradually wean off the pacifier;
- monitor the baby during sleep, not allowing him to suck his fingers;
- correctly apply the baby to the bottle or breast.
If a young mother does not have the proper experience and does not know how to properly attach a baby to the breast, then she needs to consult with a local pediatrician. A visit to the pediatric dentist is a must to minimize the risk of developing facial or dental pathologies. Children aged 4 years and older should be taught to brush their teeth on their own.
Timely prevention will help minimize the risk of complications. As a child gets older, his diction deteriorates, which can cause problems communicating with peers and lead to depression. Aesthetic defects are easiest to correct at an early age.