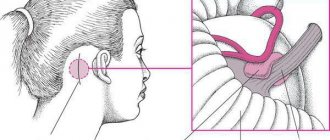
Trigeminal neuropathy (trigeminal neuralgia) is a chronic pain syndrome that involves the trigeminal (5th cranial nerve). Trigeminal neuropathy is a type of neuropathic pain (pain associated with injury or damage to a nerve). The usual or “classic” form of the disease (the so-called “Type 1”) is characterized by attacks of intense pain in the form of a burning sensation or shock that last from a few seconds to two minutes. These attacks can occur in group episodes lasting up to two hours. The “atypical” form of the disease (the so-called “Type 2”) is characterized by constant aching, burning, stabbing pain of somewhat less intensity than with type 1. Both forms of pain can occur in the same person, sometimes at the same time. The intensity of pain can lead to disability, both physical and mental.
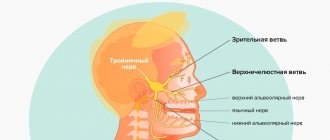
The trigeminal nerve is one of 12 paired nerves that exit the brain. The nerve has three branches that carry sensory sensations from the upper, middle and lower parts of the face, as well as the mouth, to the brain. The ophthalmic or superior ramus provides sensory sensation to most of the face, forehead, and front of the head. The maxillary or middle branch provides sensation to the cheek, upper jaw, upper lip, teeth and gums, and side of the nose. The mandibular or inferior branch innervates the lower jaw, teeth and gums, and lower lip. With trigeminal neuropathy, more than one branch may be affected. In rare cases, there may be manifestations of neuropathy on both sides at different times. Even less common is bilateral involvement.
Trigeminal neuropathy occurs most often in people over 50 years of age, although the condition can occur at any age, including in infants. The possibility of developing trigeminal neuropathy increases slightly with multiple sclerosis when it occurs in young people. The rate of new cases is approximately 12 per 100,000 people per year; the disease is more common in women than in men.
How does neuritis of the facial nerve appear?
Neuritis of the facial nerve can begin with mild pain in the ear area. Simultaneously with the onset of pain or after a couple of days, the facial muscles partially or completely lose mobility. The patient's face becomes distorted, the affected part freezes in the mask.
With timely treatment, the patient has a great chance of recovery - in 75% of cases the disease goes away completely. If facial paralysis does not resolve within three months, the patient's chances of making a full recovery are greatly reduced.
In order for facial neuritis to pass without consequences, you need to consult a doctor in the first hours after the onset of symptoms.
Causes
Trigeminal neuropathy can be associated with a variety of conditions. Neuropathy can be caused by blood vessel compression on the trigeminal nerve as it exits the brainstem. This compression causes the protective covering around the nerve (myelin sheath) to wear or become damaged. Symptoms of trigeminal neuropathy can also occur in patients with multiple sclerosis, a disease that damages the myelin sheath of the trigeminal nerve. Rarely, symptoms of neuropathy may be due to nerve compression by a tumor or arteriovenous malformation. Damage to the trigeminal nerve (possibly as a result of oral surgery, stroke, or facial trauma) can also lead to neuropathic pain.
Symptoms
The following symptoms of inflammation of the facial nerve are distinguished:
- partial or complete impairment of facial muscle movements;
- the corner of the mouth lowers, the nasolabial fold on one side is smoothed out;
- the face becomes asymmetrical;
- the eyelid does not close completely;
- the eyeball protrudes and turns upward;
- pain in the ear, taste disorder;
- watery or dry eyes;
- hearing loss or sensitivity to loud sounds;
- the patient cannot whistle or stretch out his lips with a straw.
How is the disease diagnosed?
The diagnosis of a neurological disorder is carried out by a specialist - a neurologist. To exclude dental pathologies, an initial consultation and examination by a dentist will be required. The primary examination is carried out by palpation. The doctor determines the pain of the main points located on the tongue and in the sublingual area. Unpleasant sensations occur when pressure is applied to the skin located in the lower part of the jaw on the side in which the disorder develops. In this case, there is no change in taste sensations. Degenerative changes in the mucosa, ulcerative lesions, and deformation of the lingual papillae can be visually determined.
To clarify the diagnostic assumption, the described nerve processes are blocked. Common anesthetics are used for this: lidocaine, novocaine. Confirmation of the suspected disease occurs if the pain disappears as a result of the administration of local anesthesia. At the same time, the neurologist tries to exclude anomalies with similar symptoms: tumors, cystic processes, damage to the trigeminal nerve, etc.
Causes of inflammation
Primary neuritis of the facial nerve occurs due to:
- hypothermia of the face, cold, wind, drafts;
- insufficient blood supply (ischemia) to the nerve.
Secondary neuritis of the facial nerve is caused by the following reasons:
- inflammatory diseases of the ear: otitis media, eustachitis, mastoiditis;
- infections: mumps virus, measles, herpes;
- traumatic brain injuries;
- vascular disorders - for example, atherosclerosis of the vertebral arteries;
- brain tumors;
- anesthesia of the inferior alveolar nerve by the dentist.
Other factors that provoke inflammation include:
- traveling on a bus or minibus next to an open window;
- long work under air conditioning;
- metabolic disorders in the body;
- endocrine diseases - for example, diabetes;
- hypertension, intoxication of the body;
- nervous stress, emotional instability.
Description of the pathological condition
The disease of the nerve branches located in the tongue and lower jaw is accompanied by pain and salivation disorders. Nerve clusters (nodes) located in this area belong to the peripheral parts of the NS. Despite the fact that neurologists anatomically separate the sublingual and submandibular nodes, degenerative processes occur in them simultaneously. This is due to the fact that numerous neural connections are distributed between the channels. This allows the pathology to be classified as one disease.
Complications of the disease
Neuritis of the facial nerve can lead to contracture of the facial muscles. It appears 4-6 weeks after the onset of the disease due to incomplete restoration of the motor functions of the facial muscles. Contracture is a contraction of the muscles of the affected half of the face. At the same time, it seems that it is not the diseased part of the face that is paralyzed, but the healthy one.
To avoid complications of inflammation of the facial nerve, you need to consult a doctor in time. For prevention, we recommend doing facial exercises. You will find examples of exercises at the end of the article.
Treatment
Treatment options include medication, surgery, and multimodal treatment.
Medications
Anticonvulsants, used to block nerve stimulation, are generally effective in treating type 1 NTN but are often less effective in treating type 2 neuropathy. These drugs include carbamazepine, oxcarbazepine, topiramate, gabapentin, pregabalin, clonazepam, phenytoin, lamotrigine, and valproic acid.
Tricyclic antidepressants such as amitriptyline or nortriptyline may also be used to treat pain. Analgesics and opioids are usually not effective for treating acute, recurrent pain caused by T1, although some patients with T2 respond to opioids. Ultimately, if treatment does not relieve pain or results in significant side effects such as cognitive impairment, memory loss, excessive fatigue, bone marrow suppression, or allergies, then surgery may be recommended. Because trigeminal neuropathy is most often a progressive disease that becomes drug-resistant over time, patients often seek surgical treatment.
Surgery
Several neurosurgical techniques are generally used to treat NTN, depending on the nature of the pain, the wishes of the individual, physical health, blood pressure and the presence of previous operations. Some procedures are performed on an outpatient basis, while others, which are performed under general anesthesia, are performed in a hospital setting. After these surgical procedures, there may be some reduction in the face and it is not uncommon for NTN to recur, even if the procedure was initially successful. Several procedures will be used. These are like:
- Rhizotomy is a procedure in which nerve fibers are damaged to block pain. Rhizotomy to treat NTN always causes some degree of sensory loss and facial numbness.
- Glycerin injections are an outpatient procedure that is performed after light anesthesia. This form of rhizotomy usually results in pain relief within 1-2 years. However, this procedure can be repeated several times.
- Radiofrequency thermal ablation is most often performed in an outpatient setting.
- Stereotactic radiosurgery (using Gamma Knife or CyberKnife) uses CT scanning to deliver highly focused radiotherapy to the area where the trigeminal nerve exits the brain stem. This causes slow nerve damage, which disrupts the transmission of sensory signals to the brain. Patients who have had this procedure can go into remission for up to three years.
- Microvascular decompression is the most invasive of all surgeries for treating NTN, but it also has the best long-term results and the lowest likelihood of pain recurrence. About half of people who have this procedure will experience periodic pain for 12 to 15 years.
- A neurectomy, which involves a partial incision of the nerve, can be performed at the nerve's entry point into the brainstem while attempting microvascular decompression. A neurectomy can also be performed by cutting the superficial branches of the trigeminal nerve on the face.
Surgical management of T2 is usually more problematic than for T1, especially where vascular compression is not detected on neuroimaging.
Additional treatments
Some patients benefit from combining medications with other treatment methods. These methods have varying degrees of effectiveness. Some patients find that gentle exercise, yoga, creative visualization, aromatherapy, or meditation can help. Other treatment options include acupuncture, chiropractic care, biofeedback, vitamin therapy, and nutritional therapy. Some patients note a certain effect from the use of botulinum toxin.
Causes and symptoms
As a rule, we are talking about inflammation of the temporomandibular joint (TMJ).
This can happen either as a result of mechanical trauma or an infection that has entered the body. In addition, inflammation can be acute and chronic, serous, aseptic, purulent and deforming. This disease often occurs in patients with rheumatism. Older people are especially susceptible to a type of this disease called osteoarthritis.
The main causes of TMJ inflammation:
- injuries to the bones of the facial skeleton;
- problems in the development of jaw bone tissue;
- lack of chewing teeth;
- incorrect orthopedic treatment;
- constant chewing on one side.
In patients, diseases of the jaw joint manifest themselves as follows:
- a crunching or clicking sound is heard when opening the mouth;
- it hurts to chew and yawn;
- the bite is deformed;
- headache, ringing in the ears.
Moreover, in the early stages, a person may not even experience pain, but only notice various oddities such as a jaw crunch or feeling unwell. And in some situations, on the contrary, everything is so neglected that it is impossible to even open your mouth. Here we need to take action immediately.
Trigeminal neuralgia
Trigeminal neuralgia (TN) - (synonyms: tic douloureux, or Fothergill's disease) is one of the most common facial pain (prosopalgia - (Greek prosopon (face) + algos (pain)) and is one of the most persistent pain syndromes in clinical neurology TN is a typical example of neuropathic pain and is considered the most painful type of prosopalgia. TN most often has a chronic or recurrent course, much more difficult to treat than many other types of chronic pain. High intensity and persistence of trigeminal neuralgia, its special, often painful nature, resistance traditional methods of pain relief give this problem exceptional relevance. According to WHO, the prevalence of TN is up to 30–50 patients per 100,000 population, and the incidence is 2–4 people per 100,000 population. TN is more common in women than in men, debuts in fifth decade of life and in 60% of cases has a right-sided localization.Causes of TN The most common cause of TN is compression of the proximal part of the trigeminal root within a few millimeters from the entrance of the root to the pons (i.e. n. "entry zone of the spine"). In approximately 80% of cases, compression occurs by an arterial vessel (most often a pathologically tortuous loop of the superior cerebellar artery). In other cases, such compression is caused by an aneurysm of the basilar artery, space-occupying processes in the posterior cranial fossa, tumors of the cerebellopontine angle and multiple sclerosis plaques. At the extracranial level, the main factors leading to the occurrence of TN are: tunnel syndrome - compression in the bone canal through which the nerve passes ( often in the infraorbital foramen and lower jaw), associated with its congenital narrowness, the addition of vascular diseases in old age, as well as as a result of a chronic inflammatory process in adjacent areas (caries, sinusitis); local odontogenic or rhinogenic inflammatory processes. The development of TN can be provoked by infectious processes, neuroendocrine and allergic diseases, demyelination of the trigeminal nerve root in multiple sclerosis.
Clinical manifestations of TN
The disease, in most cases, develops on one side; a bilateral process is extremely rare. First, pain occurs at the site of innervation of any of the three branches; later, as the disease progresses, pain can gradually cover areas of the face innervated by neighboring branches. The localization of pain depends on which branches are involved in the process:
- when the first branch is affected, pain is localized in the area of the superciliary arch, forehead, temple, sometimes pain occurs in the eyelids and eyeball;
- when a pathological process occurs in the second branch, pain occurs in the upper lip, wing of the nose, in the projection of the zygomatic bone, upper cheek, upper jaw and palate;
- when the third branch is affected, the pain zone is localized in the lower lip, chin, cheek, lower jaw, half of the tongue and soft palate.
Taxonomy of trigeminal prosopalgia
From the point of view of topical diagnosis, the development of any form of trigeminal prosopalgia is associated with damage to the peripheral trigeminal neuron - the peripheral trigeminal branches, the sensory trigeminal ganglion (located at the base of the skull), the sensory root of the trigeminal nerve that follows it in the direction of the brain stem, as well as those entering the brain stem sensory trigeminal fibers and sensory nuclei of the trigeminal nerve. Depending on the impact of the pathological process on the corresponding part of the trigeminal system, TN is divided into predominantly central and peripheral genesis. In the occurrence of TN of central origin, neuroendocrine, immunological and vascular factors play an important role, which lead to impaired reactivity of cortical-subcortical structures and the formation of a focus of pathological activity in the central nervous system. In the pathogenesis of peripheral TN, the compression factor, infections, injuries, allergic reactions, and odontogenic processes play an important role. Despite the difference in the symptomatology of the clinical forms of trigeminal prosopalgia, the features of facial pain are of primary importance for their differentiation, in some cases manifested by prolonged (constant) pain, and in others in the form of paroxysms of pain. Paroxysmal forms of trigeminal pain are traditionally referred to as neuralgia, and non-paroxysmal forms - trigeminal neuropathy. These forms of facial pain—neuralgia and trigeminal neuropathy—fundamentally differ in their approaches to treatment. Deafferentation trigeminal neuropathy (prosopalgia)
Deafferentation facial pain (prosopalgia) is the most severe form of trigeminal lesion, manifested by highly intense facial pain, often resistant to conservative therapy, and severe sensory impairment. Develops as a result of significant damage (destruction) of the peripheral or central structures of the trigeminal system. The concept of “deafferentation trigeminal prosopalgia”, as a general syndromological definition, was proposed by Yu. V. Grachev and Yu. A. Grigoryan (1995) to designate a special form of facial pain that develops as a result of deafferentation in the sensory system of the trigeminal nerve. The pathophysiological term “deafferentation” (de- + lat. afferentis bringing), literally means the separation of the receptor zones of peripheral nerves from the central sensory structures, due to a violation of the integrity or conductivity of nerve fibers. Typical peripheral forms of deafferentation trigeminal prosopalgia are postherpetic, tumor and iatrogenically caused facial pain (caused by destruction of the ganglion and trigeminal nerve root), and central are two quite rare forms caused by syringobulbia and medulla oblongata infarction.
Diagnostics of TN
Clinical interview plan for the evaluation of patients with facial pain. Description of pain:
- Localization of pain
- Temporary characteristics of pain (paroxysmal/non-paroxysmal, prolonged)
- Frequency of pain attacks
- Pain intensity
- Sensory nature of pain
- Other sensations accompanying facial pain (associated signs)
- Conditions and time of pain occurrence
- Medicines (other factors) that reduce or eliminate pain
Anamnestic data:
- Duration of the disease
- Conditions for the development of the first exacerbation
- The nature of the course of prosopalgia (acute, recurrent, continuous)
- Frequency of exacerbations of prosopalgia
- Previous treatment
- Disorders (neurological, somatic) accompanying the development of the disease.
When conducting palpation examination of the facial area, it is necessary to distinguish between “neuralgic” and “myofascial trigger” (English trigger). Neuralgic trigger points or zones (in patients with trigeminal neuralgia) are hyperexcitable areas of the skin and mucous membrane, with mechanical irritation, including light touch, causing a painful attack. At the same time, strong pressure, usually applied by the patient himself, not only does not cause pain, but in some cases leads to a decrease or disappearance of pain. Myofascial trigger points (essentially pain points) are located in the soft tissues of the face in the projection of the masticatory muscles. “Pressing” on them is accompanied by localized or radiating pain.
Treatment of TN The main directions of drug therapy are:
- elimination of the cause of TN, if it is known (treatment of diseased teeth, inflammatory processes in adjacent areas, etc.),
- carrying out symptomatic treatment (pain relief).
- Anticonvulsants are the drugs of choice for the treatment of TN, and carbamazepine was one of the first drugs officially approved for the treatment of this condition.
In the early 90s of the last century, a new generation of antiepileptic drugs appeared, and now anticonvulsants are usually divided into first and second generation drugs. First-generation drugs are practically not considered as the first line of treatment for NB (with the exception of carbamazepine for TN). Second generation anticonvulsants include pregabalin (Lyrica), gabapentin (Neurontin, Gabagamma, Tebantin), lamotrigine (Lamictal), oxcarbazepine (Trileptal), topiramate (Topamax), levetiracetam (Keppra), tiagabine (Gabitril), zonisamide (Zonegran), vigabatrin (Sabril), felbamate (Taloxa). These drugs have more favorable pharmacokinetic characteristics and safety profiles, as well as a lower risk of drug interactions compared to first-generation anticonvulsants. According to the recommendations of the European Federation of Neurological Societies (2009), pharmacotherapy for TN is based primarily on the use of carbamazepine (Finlepsin, Tegretol) proposed by S. Blum in 1962 (200–1200 mg/day), which is the drug of first choice (level of evidence A) . The analgesic effect of this drug is mainly due to its ability to reduce the permeability to sodium of the membranes of neurons involved in nociceptive reactions. The following treatment regimen with carbamazepine is usually prescribed: in the first two days the daily dose is 200 mg (1/2 tablet in the morning and evening), then within two days the daily dose is increased to 400 mg (morning and evening), and after that - to 600 mg (1 tablet in the morning, lunch and evening). Gabapentin (Neurontin) is the first drug in the world to be registered for the treatment of all types of neuropathic pain. Many studies have shown the effectiveness of gabapentin in patients with TN who do not respond to treatment with other drugs (carbamazepine, phenytoin, valproate, amitriptyline); in most cases, complete relief of pain was observed. The therapeutic dose ranges from 1800 to 3600 mg/day. The drug is taken 3 times a day according to the following regimen: 1st week - 900 mg/day, 2nd week - 1800 mg/day, 3rd week - 2400 mg/day, 4th week - 3600 mg/day. The results of an open-label, prospective, 12-month study of 53 patients with TN were recently published, evaluating the effectiveness of pregabalin (Lyrica) at a dose of 150–600 mg/day. Treatment with pregabalin resulted in pain relief or at least a 50% reduction in pain intensity in 25% and 49% of patients, respectively. The use of levetiracetam (Keppra) in the treatment of TN was first reported in 2004 by KR Edwards et al. The properties of this drug are particularly suitable for the treatment of TN patients with severe pain who require a rapid response to therapy. Unlike other anticonvulsants, especially carbamazepine, the hepatic cytochrome P450 system is not involved in the metabolism of levetiracetam and the drug is excreted through the kidneys. In addition, this drug has a favorable therapeutic index and has few adverse side effects (which is the main problem when using drugs to treat TN). A 10-week, prospective, open-label study showed that higher doses of levetiracetam, ranging from 3000–5000 mg/day (50–60 mg/kg/day), were required for the treatment of TN compared with the treatment of epilepsy, but did not caused significant side effects. This circumstance indicates the prospect of using this drug for the treatment of TN. Since the 1970s, antidepressants have been used to treat TN. Currently, the effectiveness of the use of tricyclic antidepressants (TCAs) in the treatment of TN has been proven. Pathogenetic treatment of patients with TN includes the use of drugs with neurometabolic, neurotrophic, antioxidant, and antihypoxic effects. In recent years, high efficiency of the use of metabolic drugs has been discovered. In the treatment of patients with TN, the high effectiveness of the metabolic drug Actovegin, a deproteinized derivative from the blood of young calves, has been shown. The main effect of this drug is to stabilize the energy potential of cells. Actovegin also has an antihypoxic effect, being an indirect antioxidant. In addition, the effect of Actovegin is manifested by indirect vasoactive and rheological effects by increasing capillary blood flow, reducing peripheral vascular resistance and improving the perfusion of organs and tissues. During an attack, it is advisable to use Actovegin intravenously in a slow stream or drip for 10 days at a dose of 400–600 mg/day. In the interictal period, the drug is prescribed orally at a dose of 200 mg 3 times a day for 1–3 months. The pathogenetic treatment of patients with TN includes the use of high doses of B vitamins as part of multicomponent preparations, which is due to their multimodal neurotropic effect (impact on metabolism, metabolism of mediators, transmission of excitation in the nervous system), as well as the ability to significantly improve nerve regeneration. In addition, B vitamins have analgesic activity. Such drugs, in particular, include Milgamma, Neuromultivit, Neurobion. Until now, the selection of analgesic therapy for NB is more an art than a science, since the choice of drugs is carried out mainly empirically. There are often situations when the use of one drug is not effective enough and there is a need for a combination of drugs. Prescribing “rational polypharmacotherapy” (simultaneous use of drugs with neurotropic, neurometabolic and analgesic mechanisms of action) allows increasing the effectiveness of treatment with lower dosages of drugs and fewer side effects.
Differentiated therapeutic approaches for paroxysmal and non-paroxysmal trigeminal prosopalgia.
Differentiated therapeutic approaches for paroxysmal and non-paroxysmal trigeminal prosopalgia
| Paroxysmal paroxysmal facial pain Duration of painful attacks: from several seconds (instant pain") to several minutes | Non-paroxysmal (long-lasting) facial pain |
| Clinical forms Trigeminal neuralgia - typical trigeminal neuralgia - trigeminal neuralgia with neuropathic manifestations (after “therapeutic blockades”) - trigeminal neuralgia in multiple sclerosis - symptomatic trigeminal neuralgia in tumors of the base of the skull and brain | Clinical forms Trigeminal neuropathy - odontogenic - traumatic - herpetic (including postherpetic neuralgia) - autoimmune (in systemic rheumatic diseases) Deafferentation trigeminal prosopalgia (high-intensity constant pain) - iatrogenic ("destructive") - postherpetic - tumor |
| Main treatment approaches - carbamazepine - a basic drug that helps suppress pain attacks - Milgamma, Milgamma-compositum Physiotherapy, reflexology - If conservative treatment of typical trigeminal neuralgia is ineffective - neurosurgical decompression of the trigeminal nerve root | Main treatment approaches - NSAIDs (diclofenac, ibuprofen, meloxicam) - gabapentin (Gabamma) - for herpetic and traumatic neuropathy, deafferentation prosopalgia - amitriptyline - for herpetic neuropathy (postherpetic neuralgia) - Milgamma, Milgamma compositum - Physiotherapy, reflexology |
For patients suffering from unbearable pain for a long time, and if conservative therapy is ineffective in the case of classical TN, surgical treatment is recommended. The following approaches are currently used:
- surgical microvascular decompression;
- stereotactic radiation therapy, gamma knife;
- percutaneous balloon microcompression;
- transdermal glycerol rhizolysis;
- Percutaneous radiofrequency treatment of the Gasserian node.
In conclusion, we note that the treatment of TN should be multidisciplinary in nature, and the choice of various treatment methods and the risks of possible complications should be discussed with the patient.