Unfortunately, not all dental defects are corrected with the help of braces, mouth guards and aligners. Quite often, patients experience pathologies, the elimination of which requires the use of more radical measures. This occurs in cases where the cause of malocclusion is not individual dental units, but a disproportion in the development of the upper and lower jaws.
A palatal expander is an orthodontic device that is intended to correct abnormalities in the development of the upper jaw.
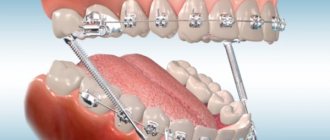
Design features of the palatal expander
A palatal expander is a metal orthodontic structure that has:
- support rings (crowns) - placed on molars;
- screw - designed to expand the device;
- wire arches - connected to supporting elements and a lock, creating a shock-absorbing effect of the structure.
Due to the constant pressure of the device on the lateral parts of the upper jaw, they quickly stretch.
General overview
The full name of the Ross apparatus is plate-type, non-removable, mechanically operating, single-jaw. The device consists of the following elements:
- Hyrex screw with guides on both sides. Serves to create an expanding force.
- Rings for temporary molars. Provide fixation of the device on the supporting teeth.
- Metal feet. They rest against temporary fangs, creating points of application of force to the dentition, additional to the rings.
- Plastic base (plate), consisting of two parts. Combines all components into a single design.
The device bears the name of its developer. It is made from a plaster model, molded according to an impression from the child’s upper jaw. Costs about 10,000 rubles.
The use of the device allows you to expand the upper jaw along the median seam by 10-13 mm, increase the length of the upper jaw arch, eliminate mesial occlusion, and achieve normalization of a number of other functions of the dentofacial apparatus in children aged 5-11 years.
Depending on the tasks being solved, the Ross apparatus can be modified, in particular, equipped with dental onlays.
Advantages and disadvantages of a palatal expander
Orthodontic construction has a number of advantages. These include:
- short active treatment period - it takes only a few weeks to correct the pathology;
- the ability to accurately predict the final result;
- expansion of the jaw does not entail a change in the position of the roots of the teeth, but allows them to remain in the same sockets without provoking;
- the design of the product is highly safe - the likelihood of injury to the oral mucosa due to device failure is excluded;
- high aesthetics - the device is invisible to others.
The negative points are the following:
- despite its high aesthetics, the palatal expander is a bulky orthodontic structure;
- the surface of the tongue is subject to a high probability of mechanical damage by the locking mechanism of the product;
- the adaptation period is accompanied by impaired swallowing function;
- presence of excessive salivation;
- pronounced articulatory disorders;
- the active period of treatment is accompanied by painful sensations.
Many patients are consoled by the fact that the discomfort associated with the use of a palatal expander does not have to be endured for long.
Ways to expand the jaw
There are several methods for expanding the jaw in adult patients: braces, aligners and, in extreme cases, surgery.
Bracket systems
The popular method of jaw expansion with braces has a significant drawback. When treated with braces, the effect is carried out due to the arch, under which the teeth tend to align. But the standard arch does not take into account the individual characteristics of the dental system, so uncontrolled expansion occurs. In some cases, improper orthodontic treatment on braces results in overexpansion, which can lead to recession of the gingival margin, the formation of an open bite and other complications.
Aligners
Jaw expansion with aligners is a completely controlled process. Prediction of changes is carried out at the diagnostic stage, before drawing up a treatment plan.
“A computed tomography scan is performed to determine bone reserve. For example, we expand the vestibular (buccal) side and see that the cortex is 3 mm. Accordingly, we will expand the dentition that much.”
Nana Gezalova, PhD, orthodontist, leading expert at the PROPRICUS clinic
Orthodontic aligners for jaw expansion are created in such a way that each subsequent one is slightly wider than the previous one. There is pressure on the teeth from the inside, and the jaw gradually, from one mouth guard to another, expands to the required parameters.
Need some advice?
Enter your phone number and we will give you a free consultation
I want a consultation
*By making an appointment you consent to the processing of your data
Compared to brace systems, aligners allow you to take into account all the features of the maxillofacial system and achieve the planned result.
The second advantage of aligners is maximum comfort for the patient:
- aligners are transparent trays that are invisible on the teeth;
- mouth guards are removable: they can be removed for an important event, speech or negotiation; they are also removed for eating and brushing teeth, so there is no need to review your diet and change habits, as when using braces;
- mouthguards are easy to use: they do not require complex care, they are easy to wash, put on and take off;
- quick adaptation period;
- autonomy of the patient from the doctor: switching from one set of mouth guards to another does not require a visit to the dentist, so you can go on a business trip or vacation.
Thus, when choosing a method of expanding the upper or lower jaw without surgery, in most cases, aligners are the best option. They are effective, comfortable and aesthetically pleasing.
Indications and contraindications
The only indication for installing a palatal expander is a pathological narrowing of the upper jaw - micrognathia.
It can develop due to:
- genetic conditioning;
- disorders of fetal development in the embryonic period;
- disruption of the endocrine system;
- consequences of rickets;
- disorders of mineral metabolism in the human body.
There are contraindications for using a palatal expander.
These include:
- asymmetrical crossbite;
- open bite of anterior teeth;
- the presence of skeletal jaw asymmetry;
- convex profile;
- inflammatory processes in periodontal tissues.
Will braces be needed?
Before starting treatment with the Marco Ross apparatus, it is impossible to say for sure whether further treatment with braces will be needed or not. This depends on the results of correction of disorders and the direction of development of the child’s dental apparatus.
In some cases, if the anomaly is not completely eliminated, braces will be required. In other circumstances, when the violations are completely eliminated, such a need does not arise.
But even if braces are used, treatment with them after correction with the Marco Ross apparatus will be much faster and easier than without it.
In addition, refusal to treat a narrowed upper jaw in childhood can create a situation in which an adult with fully formed teeth will need surgical intervention and the cost of the issue will be many times higher. If possible, it is better to avoid this.
What does the Bruxogard trainer look like and what is its purpose?
This publication provides instructions for using the TMJ joint splint.
Here https://orto-info.ru/sistemyi-vyiravnivaniya-zubov/lechebno-profilakticheskie-apparatyi/ispolzovanie-bidermana.html all the most important things about the Biderman apparatus.
Preparatory stage and installation of a palatal expander
Having examined the patient and drawn up a plan for correcting the pathology, the orthodontist begins preparing the patient for the installation of an orthodontic product.
For this purpose the following is carried out:
- a thorough examination of the patient’s oral cavity and, if necessary, treatment of carious teeth;
- professional hygienic cleaning;
- increasing the distance between the supporting molars using separation rings installed for 7 days.
The palatal expander is installed using two methods:
- directly in the patient’s oral cavity;
- on a plaster model of the patient's jaw.
Support rings can be standard or custom made.
The orthodontic screw is selected by the doctor in accordance with the therapeutic task.
Installation of wire arches is carried out by fixing closed loops with locks of support rings.
Causes of distal bite (distal occlusion)
They are almost always (in the vast majority of cases) skeletal...
- Posterior position of the lower jaw. This is the most common cause of distal occlusion
- Small (short) lower jaw.
Many people write that the cause of a distal bite may be an overdeveloped (excessively large) upper jaw. They say that this is why there is a “gap” between the front upper and lower teeth (sagittal gap)... Many years of observations and our experience have shown that this is not so. With any anomaly of occlusion, there can be no talk of any OVERdevelopment. Everything, on the contrary, is UNDERdeveloped.
The lower jaw ends up in a posterior position (the first reason) only because the lower teeth bump into the upper teeth while the upper jaw is shortened and narrowed (generally underdeveloped). Or, when the upper incisors are “wrapped” back, into retrusion (second subclass). In addition, with distal occlusion, the upper jaw is always narrower than the lower jaw. Which, by the way, is another reason for blocking the lower jaw in the posterior position. And this same “blocking” does not allow the lower jaw, which is caught in the trap, to develop normally. Here is the second reason for distal occlusion - underdevelopment of the lower jaw.
There is also a “dental” reason for distal occlusion. Or more precisely, the dental cause of closure is “second class”. This is when mesial (front) displacement of the upper lateral teeth occurs. And then, even with a normal relationship of the jaws in the sagittal plane, the closure of the lateral teeth (molars) will also be in the second class. True, this is not a true distal occlusion...
A “dental” cause of the second class may complement or may camouflage true distal occlusion. Therefore, it will not be possible to figure out what is the reason for the closure in class 2 visually (by eye). Diagnostics required.
Oral hygiene when using the device
The presence of any orthodontic structure in the oral cavity requires the patient to pay increased attention to the condition of the teeth and mucous membrane.
To avoid the development of diseases caused by the accumulation and development of pathogenic microbes on the palatal expander and teeth, it is necessary to use the following hygiene products:
- toothbrush and toothpaste (twice a day);
- use of rinse aid;
- removing food debris using toothpicks, floss, brushes;
- The presence of an irrigator will facilitate the care of the orthodontic product.
Changing the size of the jaw is a physiologically and morally very complex process. If it is not possible to avoid it, then strictly follow the orthodontist’s instructions - this will help shorten the active therapeutic period.
Manifestations of distal bite in the mouth
Closing of lateral teeth during distal occlusion.
Distal occlusion is manifested in the mouth by the closure of the upper and lower teeth according to the “second class” (violation of the relationship between the projections of the antagonist teeth of the upper and lower jaw).
In the frontal segment (at the level of the front teeth) there are two closure options (the so-called first or second subclasses).
In the first case, a “sagittal gap” is observed, which reflects the discrepancy between the dentition in the sagittal plane (anterior-posterior direction). And the upper incisors are in protrusion (inclined forward). In the second option, the upper front teeth are tilted back (into retrusion). With the formation of a deep bite (when the lower teeth are not visible from under the upper ones).
Sagittal chain with distal occlusion. 2 class 1 subclass.
Distal occlusion. 2nd class 2nd subclass.