Advantages and disadvantages
For simple surgical interventions, local anesthesia is indispensable; it has advantages over other types of sensitivity suppression. The drug that is used, an anesthetic solution, acts strictly at the injection site, which helps to avoid severe complications and adverse reactions.
The blockade of pain sensitivity develops on average in 10-15 minutes. The effect lasts for an hour or more, so local anesthesia can reduce pain in the area of the postoperative wound. The patient’s consciousness does not suffer from the action of the local anesthetic, so after the manipulation he can leave the clinic and not be in the ward.
But local anesthesia has its drawbacks. Just a few years ago, it was widely used for operations on superficial tissues and extremities; methods for intravenous administration of drugs with simultaneous application of a tourniquet were developed. Intraosseous anesthesia was widely used. But due to the large number of adverse reactions and complications, these methods began to be used less frequently. And after receiving high-quality drugs for anesthesia, dangerous methods of pain relief were practically abandoned.
The disadvantage of the local method is its limited scope of application. It is effective for anesthesia of mucous membranes, skin and superficial tissues, but is not used for operations on the abdominal and pelvic organs, neck and head.
The infiltration type of local anesthesia cannot be used when operating on malignant tumors due to the possibility of tumor cells entering beyond the wound into other tissues. This increases the risk of developing metastases.
Lidocaine (Lidocaine)
2-diethylamine-2′, 6′ acetoxylide hydrochloride. Synonyms: baicaine, dentacaine, xicaine, xylodont, xylocaine8, xylestesin, xylonest, lignocaine, lignospan, lidestin, luan, octocaine, solcaine. Local anesthetic of the amide group, acetanilide derivative. The drug is superior to novocaine in anesthetic activity and duration of action, and is less likely to cause allergic reactions. The drug is compatible with sulfonamides. Lidocaine has antiarrhythmic and sedative effects. The drug affects the conduction system of the heart and suppresses ectopic foci of excitation, which makes it possible to use it as an antiarrhythmic agent.
Indications for use Lidocaine is used for all types of local anesthesia in dental surgery. Contraindications • Hypersensitivity to lidocaine and other components of the drug (adrenaline, sulfates). • Sick sinus syndrome in the elderly. • Atrioventricular block. • Severe bradycardia. • Cardiogenic shock. • Severe liver dysfunction. • History of epileptiform seizures induced by lidocaine. • Pregnancy. • Myasthenia gravis. It should be used with caution in diseases of the nervous system, septicemia, hypertension and in childhood. Cautions : Caution should be used for diseases of the nervous system, septicemia, hypertension, children and elderly patients. When using an ampoule solution of lidocaine, you should check the concentration of the drug, since as an antiarrhythmic drug it can be produced in the form of a 10% solution, the use of which is completely unacceptable for injection anesthesia in dentistry. Side effects Allergic reactions (urticaria, angioedema, anaphylactic shock) to lidocaine are rare. Possible headache, dizziness, drowsiness, anxiety, tinnitus, blurred vision, convulsive twitching, tremor, decreased blood pressure, bradycardia, disorientation. Cases of idiosyncrasy to lidocaine have been described. Method of administration and dosage Lidocaine is used for all types of anesthesia: in the form of a 2% solution for infiltration and conduction anesthesia; in the form of a 10% aerosol solution, 5% gel, 2-5% ointment - for topical anesthesia of the oral mucosa. The drug dilates blood vessels and is used in dentistry in combination with vasoconstrictors.
The maximum total dose for injection is 4.4 mg/kg, but not more than 300 mg. For superficial anesthesia of the mucous membranes, use no more than 2 ml of a 10% lidocaine solution (200 mg).
Types of local anesthesia
Several types of local anesthesia are used in surgical practice, but some of them already have historical significance. The main methods of pain relief are the following:
- superficial anesthesia - pain sensitivity is suppressed after the anesthetic comes into contact with the surface of the tissue, most often used to anesthetize the mucous membranes. The anesthetic solution is applied by lubrication or irrigation, the effect lasts for 10 minutes;
- infiltration anesthesia - anesthesia by impregnation, or infiltration of tissue layers with a local anesthetic. The technique allows you to control the depth and width of the drug injection, depending on the intended incision. The medicine is injected carefully first into the subcutaneous area until the lemon peel effect appears, then the needle is gradually moved inward and an additional dose of the drug is injected;
- anesthesia according to Vishnevsky is an improved version of the infiltration method. A weak anesthetic solution is injected layer by layer under high pressure. A tight creeping infiltrate forms in the tissues. It spreads through the interfascial spaces and disrupts the conduction of impulses along the nerves passing through them. After cutting the wound, the liquid gradually flows out of the wound, so there is no risk of its absorption into the systemic circulation and the development of toxic reactions;
- conduction anesthesia is the essence of the method in anesthetizing a specific area of the body innervated by the nerve trunk. An anesthetic drug is injected into the tissue around the nerve; the technique is used for operations on the limbs;
- spinal anesthesia - the analgesic effect is achieved by injecting an anesthetic drug under the choroid of the spinal cord, the main place of drug administration is the lumbar region, and pain sensitivity in the pelvic organs and lower extremities disappears. But tactile sensitivity does not suffer;
- epidural anesthesia is a type of anesthesia in which a local anesthetic is injected into the space over the dura mater of the spinal cord, and a puncture is also performed in the lumbar region. Sensitivity is lost after 15-20 minutes, but the effect lasts for 3-4 hours. The use of this type of anesthesia allows you to resume activity early after surgery;
- bone anesthesia is a type of anesthesia in which an anesthetic solution is injected into spongy bone. Currently, it is practically not used; previously it was used for operations on the limbs.
The demographic situation in the world entails the emergence of a complex of economic and social problems caused by the changing role of older people in society. The creation of new means and techniques that help increase the duration of a person’s active life while maintaining basic physiological functions is one of the pressing problems of aesthetic medicine [1]. Cosmetology primarily involves preserving and improving appearance, preventing aging of the face and body, and rejuvenating programs without surgical intervention. The emergence of high-tech methods that make it possible to correct involutional changes in the skin, and the tendency to move from the use of non-invasive manipulations to more invasive techniques have made it possible for cosmetologists to successfully carry out anti-aging procedures, less often resorting to plastic surgery [2]. Most invasive procedures performed require preliminary anesthesia. Therefore, an urgent problem is the choice of anesthesia method for cosmetic interventions.
As a rule, local anesthesia is used in cosmetology, which includes application (superficial, topical, terminal), infiltration and regional [3]. Superficial anesthesia occurs when the local anesthetic comes into direct contact with tissue. With infiltration anesthesia, a local anesthetic is injected into the surgical area intradermally with a thin needle, which blocks the conduction of nerve impulses in the deeper layers of tissue. Regional anesthesia is based on the administration of a local anesthetic in close proximity to the nerve trunk innervating a specific area, and can be conductive, spinal, epidural or intravascular. More often, cosmetologists use superficial and infiltration anesthesia. The use of injection methods of anesthesia is not always justified, especially when there is a large number of elements to be removed, a large area of the treated surface, etc. Injection of anesthetics leads to rapid swelling and compression of blood vessels, which modifies the clinical picture, disrupting the visualization of blood vessels. These features make it difficult to perform injection contouring, laser and photocoagulation of benign vascular neoplasms and other cosmetic procedures. Also, injection methods are unsafe from the point of view of toxic effects. Severe and sometimes fatal toxic effects on the central nervous (CNS) and cardiovascular systems can occur with significant overdose of anesthetics. This occurs when large doses of anesthetics are inadvertently released into the systemic circulation [4]. Therefore, the safest method in the practice of a cosmetologist is the application method. This method best meets the requirements of a cosmetologist for anesthesia, since it has a minimal traumatic index, causes a small number of visible side effects, and provides the opportunity to carry out a one-step complex correction in a short time.
In cosmetology, any manipulation associated with violating the integrity of the skin barrier is performed with anesthesia to reduce the pain of the procedure. Invasive procedures include laser and radio wave destruction, electrocoagulation of benign neoplasms, mesotherapy, injection contouring, administration of botulinum toxin A, hair removal, especially in areas with thin sensitive skin (bio- and electrolysis, laser and photoepilation), derma-abrasion, skin graft transplantation , puncture biopsy.
Structure and properties of local anesthetics
All local anesthetics have a similar chemical structure. They consist of a hydrophobic (lipophilic) aromatic group, a hydrophilic (secondary or tertiary) amino group, and an intermediate ester or amide chain. Depending on the type of intermediate chain, local anesthetics are divided into esters and amides (Fig. 1).
Rice. 1. The structure of local anesthetics.
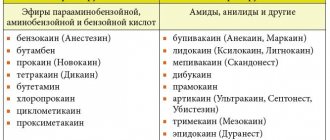
Local anesthetics of the ester group include novocaine (procaine), benzocaine (anesthesin), tetracaine (amethocaine), etc. Amide anesthetics include lidocaine (xylocaine), prilocaine, mepivacaine, bupivacaine, ropivacaine, etc. Between these two groups There are important differences between local anesthetics. Esters are relatively unstable in solutions and are quickly hydrolyzed in the body by cholinesterase and some other esterases. One of the hydrolysis products is para-aminobenzoic acid, which is a common cause of allergic reactions. In contrast, amides are relatively stable in solution and are slowly broken down by liver amidases. In addition, hypersensitivity reactions to anesthetics of the amide group develop extremely rarely [4].
The chemical structure of local anesthetics determines their physicochemical characteristics and clinical properties (Fig. 2, 3).
Rice. 2. Properties of local anesthetics [4].
Rice. 3. Physico-chemical and pharmacological effects of local anesthetics [4].
When working with anesthetics, it is important for cosmetologists to know how quickly a particular drug will act, what the strength of anesthesia will be, how long the effect will last and what risks the presence of a particular component in the composition carries. There is a correlation between the lipid solubility of an anesthetic and its potency, which reflects the ability to penetrate the perineurium and neuronal cell membranes to reach the point of action in the axoplasm.
Binding to tissue proteins affects the duration of action of local anesthetics. For example, procaine binds weakly to proteins and its effect is short-lived. Lidocaine and prilocaine are moderately protein bound and have an average duration of action [4].
The dissociation constant (pKa) is the most important factor affecting the rate of onset of the effect. Low pKa values indicate rapid development of the reaction. For example, a reaction to lidocaine will develop faster than to tetracaine. The closer the pKa is to the physiological pH, the higher the concentration of the non-ionized fraction that penetrates the neuron membrane, the faster the local anesthetic begins to act. Having entered the cell, some of the molecules are ionized until a new equilibrium state is reached between the ionized and non-ionized fractions. Only ionized cation molecules interact with receptors in sodium channels. The degree of ionization of the anesthetic is of great clinical importance. For example, when it enters tissue with a low pH (for example, an inflammatory process at the injection site), the concentration of the ionized fraction of the anesthetic increases, and it takes more time for the effect to develop. However, other factors, such as the dose and final concentration of anesthetic in tissues, can also influence the rate of blockade development [4].
Effects on different sensory modalities
Local anesthetics reversibly block the conduction of nerve impulses in peripheral nerves and nerve endings. After the administration of the anesthetic, pain sensitivity first disappears, then temperature, tactile and proprioceptive [4]. Anesthetics used for topical anesthesia often do not lead to loss of tactile sensitivity, which does not indicate their ability to block pain sensitivity.
Systemic action of local anesthetics and influence on the inflammatory response
Since sodium channel blockade affects the propagation of action potentials throughout the body, it is not surprising that local anesthetics can produce systemic toxic effects. In addition to the side effects that are characteristic of all local anesthetics, there are also individual ones that are characteristic only of certain drugs.
Local anesthetics are characterized by a two-phase effect on the central nervous system. If they are not introduced too quickly, early symptoms appear first, then later, more severe ones. Low doses of lidocaine (2-4 mg/kg) have an anticonvulsant effect and are used to treat status epilepticus, but after administration of large doses, CNS excitation develops. As the concentration of local anesthetic in the plasma increases, numbness of the tongue and mouth, dizziness, blurred vision, slurred speech, muscle twitching and tremors, restlessness and confusion of speech are observed. If the concentration of local anesthetic in plasma exceeds a critical level (for lidocaine - 9 mcg/ml), a grand mal seizure may develop.
The dual effect of local anesthetics occurs when affecting the cardiovascular system. Low doses of lidocaine can eliminate some types of ventricular arrhythmias. An overdose of local anesthetics can cause profound arterial hypotension, bradycardia, bradyarrhythmia, and even cardiac arrest. Typically, cardiovascular complications develop after the onset of neurological syndromes (Fig. 4).
Rice. 4. Systemic effect of local anesthetics [4].
Allergic reactions to modern local anesthetics are very rare. Most often, skin reactions are observed with repeated use of ester group anesthetics; anaphylactic reactions occur much less frequently. The role of a hapten is a metabolite - para-aminobenzoic acid, which induces an immunological reaction. The existence of cross-sensitization between ether and amide anesthetics has not been proven. Rare allergic reactions to amide anesthetics in the vast majority of cases are caused by methylarabene, added as a stabilizer to multi-dose vials, or by the presence of preservatives in TMA [4].
The pain that a person experiences due to tissue damage is a consequence of the activation of peripheral and central sensitization mechanisms. These events cause inflammation and are accompanied by the release of a wide range of tissue plasma and neurogenic mediators and algogens in the area of damage. Local anesthetics, by blocking the mechanisms of peripheral sensitization, can significantly reduce catabolic reactions in the post-procedure period, prevent or reduce the development of swelling, redness, and inflammation.
The results of the studies showed the inhibitory activity of local anesthetics in therapeutic concentrations (lidocaine 0.25-4%, tetracaine 0.25-4%) against a number of pathogenic bacteria, herpes viruses and fungi. Thus, local anesthetics have a complex local anti-inflammatory effect, and their use can shorten the patient’s recovery period [5].
History of the use of topical local anesthetics for anesthesia of the skin
The history of the use of topical anesthetics for the skin and mucous membranes goes back more than 130 years. The first local anesthetic, described by A. Niemann (1860) and put into practice by doctors Koller and Anrep in the 70-80s of the last century, was cocaine. Despite its widespread use, this anesthetic had a number of serious disadvantages, such as short duration of action, addiction, and most importantly, high toxicity, which led to many cases of severe and even fatal poisoning.
Methods with low concentrations and the introduction of adrenaline (1892), which ensured slower absorption due to its vasoconstrictor effect, made it possible to somewhat reduce the toxicity of cocaine-based anesthetics.
The discovery of novocaine in 1904 by the German chemist A. Eichhorn ushered in a new era in regional anesthesia. Applications of novocaine solution had a weak analgesic effect for manipulations on the skin.
In 1943, the Swedish scientist N. Lofgren managed to introduce a new class of local anesthetic substances by synthesizing lidocaine. The drug became the “anesthetic of choice”, replacing novocaine as the “gold standard”.
In 1957, S. Monash, and in 1971, J. Adriani, N. Dalili, in search of an ideal drug for local anesthesia of the skin, showed that some local anesthetics, although they had an anesthetic effect on the skin, but none of the proposed drugs was not sufficiently clinically effective. After 10 years, it was proposed to use 5 or 10% amethocaine (tetracaine), dissolved in dimethyl-sulphoxide (DMSO, dimethyl-sulphoxide), which ensures the penetration of the local anesthetic through intact skin. However, the drug was not widely used in clinical practice, since DMSO caused various pathological skin reactions associated with the release of histamine. In the 60s of the 20th century, 30% lidocaine was used for local anesthesia of the skin, but the use of such a high concentration of local anesthetic caused toxic complications without providing sufficient anesthesia.
In the late 70s (L. Оhlsen) [6], ketocaine (a local anesthetic with high lipophilicity) was developed, which was effective for anesthesia of the skin, but later its clinical use was discontinued due to the development of severe local skin reactions with blistering.
The invention of an anesthetic based on an eutectic mixture of lidocaine 2.5% and prilocaine 2.5% made it possible to satisfy two main requirements affecting penetration through intact skin and the provision of local anesthesia. Firstly, it must have a high concentration (in each fat drop the combined concentration of anesthetics reaches up to 80%), which allows it to overcome the lipophilic keratin structures of the skin, and secondly, it must contain a sufficient amount of water to moisturize the skin and improve the absorption of the drug through intact areas of the skin . The low content of anesthetics in the cream allows you to avoid toxic reactions, provided that the recommended doses (no more than 60 g) and areas of treated surfaces (no more than 600 cm2 for adults) are observed [7].
Practicing dermatologists and cosmetologists will be interested in a new drug - Acriol Pro
, which contains 2.5% lidocaine and 2.5% prilocaine (Fig. 5).
Rice. 5. Structure of amide-type local anesthetics lidocaine (a) and prilocaine (b). Note. 1 - hydrophobic aromatic group, providing passive diffusion of compounds through the membrane of nerve cells; 2 - hydrophilic center containing a tertiary (lidocaine) or secondary (prilocaine) nitrogen atom that interacts with the receptor on the inner surface of the nerve fiber membrane; 3 - aliphatic chain connecting the lipophilic and hydrophilic parts of the molecules.
Clinical studies of topical local anesthetics
In Russia, clinical studies using a cream with 2.5% lidocaine and 2.5% prilocaine were conducted by T.I. Zhigultsova et al. [8]. The study involved 382 patients aged from 2 to 60 years. Patients underwent various manipulations that required pain relief: biorevitalization ( n
=30), injection contour plastic (
n
=27), cosmetic tattooing (
n
=37), removal of benign skin neoplasms using diathermocoagulation (
n
=180), removal of hyperpigmentation, pigmented flat benign neoplasms such as Becker’s nevus, Spitz’s nevus using dermabrasion (
n
=22), microcrystalline dermabrasion (
n
=30), electrolysis (
n
=56). The authors noted a good analgesic effect for all manipulations performed. Side effects were observed in 9 patients and manifested as a temporary local reaction of the skin in the form of redness; in 4 patients, itching and burning were observed during application of the cream, which disappeared after removal of the cream.
The effectiveness of a cream with 2.5% lidocaine and 2.5% prilocaine was assessed for patients requiring aesthetic correction using permanent tattooing [9]. A good result of anesthesia and a high level of safety of using this cream have been shown in the category of patients who require one-stage complex correction (interciliary permanent tattooing is carried out simultaneously with correction of the lips with small volumes of contour plastic preparations and elimination/reduction of the depth and severity of wrinkles in the neck area with biorevitalizant preparations. Notes by the author the advantages of this anesthetic in areas of tattooing (eyebrows, eyelids), which have maximum pain during procedures, and the inconvenience of local injection anesthesia by introducing a local anesthetic by changing the shape of the tattoo object, which is also accompanied by the highest risk of possible complications.
All researchers note the availability of anesthesia using a cream with 2.5% lidocaine and 2.5% prilocaine, a sense of comfort, safety, relaxation in the patient and convenience during the procedure. However, pain is not only associated with physical impact - it can be provoked by suggestion. In a study by P. Aslaksen et al. [10] studied the extent to which knowledge of the effect of analgesic therapy influences the reduction of pain. Healthy volunteers ( n
=142) were divided into six groups. Participants in group 1 received anesthesia (2.5% lidocaine and 2.5% prilocaine cream) and were informed about it; in the 2nd group, anesthesia was performed, but they reported the expectation of hyperalgesia; participants in groups 3 and 4 received a placebo with the same information; in group 5 they received pain relief without information; in group 6 they received painful stimulation without anesthesia. Pain was stimulated by heating the skin area to 48 °C and was assessed based on the volunteers' feedback and blood pressure before and after applying the cream and pain stimulation. Results showed that pain was subjectively and objectively less severe in the group receiving positive pain relief information and greater in the hyperalgesia groups, regardless of drug or placebo use. These results indicate that emotional factors can significantly influence the effect of analgesia, so the product should be comfortable for patients to use.
In a double-blind, randomized, placebo-controlled study, 2.5% lidocaine and 2.5% prilocaine cream were used for cryotherapy of warts of the sole of the feet [11]. Cream ( n
=32) or placebo (
n
=32) was applied in a thick layer locally in the wart area under an occlusive dressing for 60 minutes. Anesthesia was well tolerated, but with deep lesions the effectiveness was insufficient.
Topical local anesthetics are used in the treatment of keloids. A cream with 2.5% lidocaine and 2.5% prilocaine showed better efficacy than a cream with a combination of lidocaine/tetracaine in laser treatment of tattoos and keloids in acne [12].
In a study by E. Hernandez et al. [13, 14] it was shown that the effectiveness of a cream with 2.5% lidocaine and 2.5% prilocaine is 2 times higher compared to 40% lidocaine ointment during laser procedures.
Thus, a number of conclusions can be drawn.
An urgent task of modern cosmetology is the selection of optimal anesthesia methods for carrying out invasive cosmetic procedures. Currently, topical local anesthetics with a minimal amount of active anesthetic are the preferred means of reducing procedural morbidity.
The emotional state of the patient significantly influences the effectiveness of anesthesia, so anesthesia should be convenient and comfortable for the patient.
The combination of 2.5% lidocaine and 2.5% prilocaine is widely used for anesthesia in the practice of dermatologists and cosmetologists throughout the world. In Russia, only this combination has registration status as a medicinal product. The results of Russian and foreign studies allow us to conclude that this combination is highly effective and safe, and a number of advantages, such as the presence of an anti-inflammatory effect, high compliance and long-term effects, allow us to recommend the combination of 2.5% lidocaine and 2.5% prilocaine as the drug of choice among local topical anesthetics.
For dermatologists and cosmetologists, a new drug from Akrikhin JSC - Akriol Pro
(2.5% lidocaine and 2.5% prilocaine). The use of this product meets modern healthcare needs and can be implemented as part of an import substitution program.
The authors declare no conflict of interest.
Preparations for local anesthesia
Local anesthetics are drugs from the group of neurotropic drugs that completely or partially block the flow of signals along nerve fibers from the site of painful manipulation or surgery to the central parts of the nervous system.
The peculiarity of the action of drugs is related to their spectrum of action. They suppress the transmission of signals along myelinated type A nerve fibers, which transmit feelings of pain, smell, and temperature. Tactile sensations are carried out through type B fibers, and anesthetics do not affect them. Therefore, when using local anesthesia, the patient does not feel pain, but feels the touch of the doctor and the surgical instrument.
Local anesthetic drugs are divided into 3 groups depending on the duration of action:
- short-acting - the effect lasts 30-50 minutes, these include Novocain;
- average duration - up to 90 minutes, these are drugs Lidocaine, Trimecaine, Ultracaine;
- long-acting – the effect lasts more than 90 minutes, typical for Bupivacaine.
Local anesthetic drugs affect the electrochemical processes of ion exchange in nerve endings. Medicines work effectively in an alkaline environment and tissues rich in lipids, which include nerves. But the analgesic effect decreases with severe tissue inflammation, which is associated with a transition of pH to the acidic side.
The effect of local anesthetics is enhanced by drugs that affect vascular tone. Therefore, they are often combined with adrenaline to prolong the effect. This allows you to reduce the dose of pain medication and avoid toxic reactions.
Trimecain (Trimecainum)
Synonyms: 2,4,6 - diethylaminoacetic acid anilide trimethylacetylate hydrochloride. Trimecaine is similar in pharmacological action to lidocaine. Its anesthetic activity is 2-3 times higher than novocaine, it acts faster and longer, and does not irritate tissues. Trimecaine is somewhat more toxic than novocaine, especially in higher concentrations. The drug dilates blood vessels and is used in dental practice with vasoconstrictors. Indications for use • Infiltration anesthesia for interventions on the upper jaw. • Conduction anesthesia. • Superficial anesthesia of the oral mucosa. In addition, trimecaine, like lidocaine, can be used for ventricular extrasystoles and tachyarrhythmia. Contraindications Contraindications are hypersensitivity to trimecaine, weakness of the sinus node, AV block, severe bradycardia, cardiogenic shock, liver and kidney pathology. Method of application It is used mainly for conduction and infiltration anesthesia, less often for surface anesthesia. Used for injection in the form of a 2% solution, topically - in the form of a 3-5% ointment. To slow down absorption, add adrenaline to the trimecaine solution (0.1% solution, 1-2 drops per 5-10 ml of trimecaine solution). The maximum total dose for injection is 300 mg. Interaction with other drugs Vasoconstrictors enhance and prolong the effect of trimecaine. Preliminary administration of tranquilizers and sleeping pills increases the effect of trimecaine.
What is operated under local anesthesia in mammology?
The mammary glands are located superficially, they do not have muscles and large nerve trunks. Breast tissue is loosely located; in young women, glandular tissue predominates, which is replaced by fatty tissue with age. Therefore, for numerous manipulations and operations, local anesthesia can be used.
In mammology, anesthesia is used to perform invasive diagnostics, which include breast tissue biopsy. To do this, a local anesthetic is injected with a thin needle into the area of the intended puncture. After 10-15 minutes, the doctor can take breast tissue for examination without fear of causing pain to the patient.
Local infiltration anesthesia in mammology is used for small, minimally invasive operations. A woman can undergo puncture of a breast cyst after preliminary infiltration anesthesia. A similar approach can be used when removing small benign breast tumors.
In men, anesthesia is used during surgery for type 1 gynecomastia, when the size of the gland is still small. Infiltration of tissues increases hydrostatic pressure in them, thanks to which the doctor can easily separate pathological tissues from healthy ones.
The dangers of additives to anesthetics
Many adverse reactions are caused not by the active substance itself, but by additives in the drug. They perform important functions, but at the same time they increase the risks of anesthesia.
Vasiconstrictors
They slow down the penetration of the painkiller into the blood, thereby increasing its effectiveness. This ability is possessed by:
- adrenalin;
- norepinephrine;
- filipressin.
The following complications are typical for vasoconstrictors:
- rise in blood pressure;
- rapid heartbeat (tachycardia);
- heart rhythm disturbance;
- angina attacks;
- headache.
Preservatives
Thanks to the antibacterial and antifungal action, the drug is protected from microorganisms. However, they can cause sensitization of the body and anaphylactic shock.
Stabilizers
Prevents oxidative processes, increasing the shelf life of the painkiller. They are dangerous due to the appearance of urticaria, edema, nervous and vagal reflexes [2].
Is it painful to do local infiltration anesthesia?
When performing anesthesia, a standard disposable syringe with a thin needle is used. Whether local anesthesia is painful depends on your general pain threshold. The patient feels the moment of the first puncture of the skin and a slight feeling of fullness when the drug is administered. After the medication begins to act, sensitivity disappears. The doctor checks how effective the injection is by tapping the skin. In response, there is a feeling that the injection site has become woody.
After the end of anesthesia, sensitivity gradually increases, and a slight tingling sensation may appear. If anesthesia was performed for surgery, pain in the wound area begins to bother you, which can be reduced with the help of non-steroidal anti-inflammatory drugs.
Bumecaine
Synonyms: pyromecaine. Indications for use
Pyromecaine is used for superficial anesthesia for stomatitis, gingivitis, glossitis, pulpitis, to anesthetize the injection site and relieve an increased gag reflex. Method of administration and dosage Pyromecaine in dentistry is used only for superficial anesthesia: in the form of a 1% solution to suppress the gag reflex when taking impressions; A 1-2% solution and 5% pyromecaine ointment are used to anesthetize the mucous membranes. An ointment containing 5% pyromecaine and 5% methyluracil, which has an anti-inflammatory effect and stimulates regeneration processes, has been developed for dental practice. When treating inflammatory diseases of the oral cavity, the ointment can be used 1-3 times a day. The dose of ointment should not exceed 1 g.
Contraindications for local anesthesia
Local infiltration anesthesia is a relatively safe method of pain relief. But to reduce risks during and after surgery, it is necessary to take into account contraindications to the use of the method. The main ones are the following:
- allergy to anesthetic - if earlier during dental treatment under local anesthesia an allergy to an anesthetic appeared, then during breast surgery the effect will repeat, and may be more pronounced, up to anaphylactic shock;
- psychomotor agitation and mental illness, reaction to the administration of an anesthetic and the surgical procedure itself can cause unpredictable behavior of the patient;
- during operations on malignant tumors - when infiltration anesthesia does not allow compliance with the ablastic rule;
- during long operations that require the use of microsurgical equipment;
- during interventions on areas of the body with a pronounced vascular network, for example, on the neck.
If local anesthesia is contraindicated, general anesthesia is preferred.
Side effects of painkillers
The negative effects of local anesthesia, although rare, can be quite serious. Some of them develop very quickly, and the dentist must be ready to quickly take action in each of the possible cases.
- Toxic effects: convulsions, drop in blood pressure, arrhythmia, drowsiness. This is the most common group of side effects. They develop when an overdose or a needle accidentally gets into a blood vessel.
- Reactions at the injection site: swelling, inflammation, appearance of ischemic zones. Usually occur when injection technique is violated.
- Effect on the central nervous system: nervousness, dizziness, unreasonable fear, double vision, temperature fluctuations, convulsions, loss of consciousness.
- Effect on the cardiovascular system: decreased heart rate, drop in blood pressure.
- Allergic reactions: itching, discharge from the eyes or nose, Quincke's edema [2].
However, local anesthesia is much safer than general anesthesia, which is used in dentistry only in extreme cases.
Allergic reactions to painkillers
Allergies are an example of a side effect of anesthetics that is primarily associated with additives. Occasionally, the reaction is provoked by esters and much more often by preservatives (methylparaben, propylparaben, parabenzoic acid) or the bisulfite stabilizer.
There are two types of allergic reactions:
- Immediate hypersensitivity. It appears within one hour, in severe cases - almost immediately.
- Delayed hypersensitivity. Deterioration of the condition is observed 24–72 hours after injection [3].