* The price of endotracheal anesthesia is included in the cost of the operation
Some general information about anesthesia methods. Anesthesia can be local or general. Local anesthesia is used for minor surgical procedures. For example, when removing papillomas, wen and moles, or when reinforcing the face. With local anesthesia, the patient is conscious, but the operation area completely loses sensitivity.
General anesthesia is necessary for long and complex operations. During general anesthesia, the patient is immersed in a state of drug-induced sleep, and vital functions - breathing, cardiac activity - are controlled by an anesthesiologist. Anesthesia is always general anesthesia. The terms “local anesthesia” or “general anesthesia” are meaningless, although they can sometimes be found in publications and in everyday speech.
What is endotracheal anesthesia?
There are two types of general anesthesia - intravenous and inhalation anesthesia. In the first case, medications that put a person to sleep are administered intravenously by the anesthesiologist. During inhalation anesthesia, drugs enter the body with inhaled air in gaseous form.
Inhalation anesthesia can be performed using a mask or intubation technique. The mask technique involves the supply of oxygen and anesthesia drugs through a special mask and does not require insertion of a breathing tube into the trachea. With the intubation technique, a tube is inserted into the trachea, through which oxygen and anesthetic substances are supplied, and carbon dioxide is removed.
Endotracheal anesthesia is a technique of inhalation anesthesia, a variant of general anesthesia, in which during surgery the supply of medications and external breathing are carried out through a special tube inserted into the upper respiratory tract, that is, into the trachea.
Combined endotracheal anesthesia is a separate method of general anesthesia, in which anesthesia drugs are administered both intravenously and through the respiratory tract. In other words, it is a combination of intravenous and inhalational anesthesia.
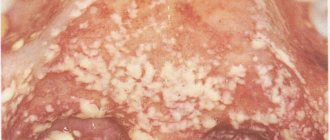
Tonsil hypertrophy
Palatine tonsil hypertrophy is a persistent enlargement of the tonsils that interferes with breathing through the mouth. With hypertrophy, breathing during sleep occurs with episodes of stopping, and snoring intensifies. There may be difficulty swallowing food, and speech becomes difficult.
To determine the degree of enlargement of the tonsils, the pharynx is examined. The doctor focuses on the edge of the anterior arch and the midline of the pharynx (uvula-uvula). The distance is divided into three conventional parts .
There is a classification in which several stages of tonsil hypertrophy are distinguished:
- I degree of hypertrophy - an increase in the tonsil by 1/3 of the distance from the arch to the uvula (the tonsils look behind the arches in the larynx)
- II degree of hypertrophy - tonsils are enlarged by 2/3 of the space from the arch to the uvula
- III degree of hypertrophy - the tonsils are greatly enlarged, reach the uvula and can even touch it
How is endotracheal anesthesia performed?
Preparation for surgery consists of several stages. The preparatory stage is premedication. Before surgery, the patient is given sedatives - tranquilizers, drugs with anxiolytic effect. Taking sleeping pills the evening before surgery is also part of the preparatory phase. Thanks to premedication, a person approaches surgery in a calm and balanced state.
Immediately before the operation, induction anesthesia is performed - intravenous administration of sedatives, which ensures smooth falling asleep before intubation begins. The next stage is muscle relaxation. When the patient falls asleep, he is given a small dose of muscle relaxants - drugs that help relax the muscles. Thanks to muscle relaxants, the tone of the laryngeal muscles is reduced and optimal conditions are created for the insertion of an endotracheal tube.
The fourth stage is the direct insertion of the endotracheal tube and its connection to the ventilator. At this stage, the patient is already sleeping and dreaming, and nothing bothers him.
Why do you still need to remove your tonsils?
According to the results of many different studies, a large number of different pathogens have been identified, including streptococci, staphylococci, Haemophilus influenzae, lymphotropic viruses, etc., which contribute to the development of chronic tonsillitis.
But the leading role in the development of chronic changes in the palatine tonsils, as well as local and general complications of chronic tonsillitis, is played by beta-hemolytic streptococcus from group A (S. pyogenes) - a microorganism that also uses anaerobic respiration for its vital functions. This bacterium is more often found in the deep sections of the recesses (crypts) of the palatine tonsils, since they contain the least amount of oxygen, which is the most favorable environment for the proliferation of anaerobic microorganisms.
Chronic tonsillitis becomes a focus of infection, a chronic infectious-allergic disease with a local inflammatory reaction in the palatine tonsils - all this is a consequence of the activity of not only beta-hemolytic streptococcus, but also its antigens and various pathogenicity factors, namely streptolysins.3
As a source of infection, chronic tonsillitis causes intoxication of the body. A separate problem is caused by various complications of chronic tonsillitis, for example paratonsillitis and paratonsillar abscess are quite common.
The treatment of such complications may require not only outpatient care, but also inpatient treatment with surgical intervention.
Common complications of chronic tonsillitis are: tonsillogenic sepsis (life-threatening condition), rheumatoid arthritis, endocarditis, glomerulonephritis. These conditions significantly reduce the quality of life of patients and can lead to disability.4
In connection with the above, the main treatment tactic is sanitization of the source of infection, in other words, elimination of the pathogen. There are two treatment methods - conservative or surgical.
The choice of method is currently clearly regulated and based on the classification of B.S. Preobrazhensky and V.T. Palchuna.5
This classification is based on the symptoms of chronic tonsillitis, as well as the presence and severity of toxic-allergic reactions and the presence of complications. The classification identifies 2 forms of chronic tonsillitis:
- simple (characterized by the presence of only local signs of chronic tonsillitis and tonsillitis no more than 1–2 times a year)
- toxic-allergic: toxic-allergic form I and toxic-allergic form II6
Advantages of endotracheal anesthesia
Maximum safety and complete control over the depth of drug-induced sleep are the main advantages of endotracheal anesthesia. The risk of “waking up during surgery” is eliminated, as is the slightest possibility of disruption of the respiratory and cardiovascular systems. In other words, this is the safest and most reliable type of general anesthesia, during which the anesthesiologist has everything under control!
The advantages of endotracheal anesthesia are explained by the fact that, thanks to intubation, continuous monitoring of respiratory function is carried out. The anesthesiologist constantly monitors adequate ventilation of the lungs, accurately doses the amount of oxygen entering the lungs, and carefully controls the carbon dioxide content in the exhaled air.
From a safety point of view, one more point is important - the risk of tongue retraction, which is present with intravenous and mask anesthesia techniques, is eliminated. In addition, the endotracheal tube completely isolates the respiratory tract from the esophagus, which eliminates the possibility of saliva and stomach contents entering the pulmonary system.
Other features and advantages of endotracheal anesthesia are the possibility of active use of muscle relaxants, the possibility of performing long-term operations with artificial ventilation, and minimizing the risk of postoperative complications from the respiratory and cardiovascular systems.
Exercise stress
These exercises will help prevent your ability to swallow from deteriorating during radiation therapy. They will also help you maintain your ability to swallow over time. Your swallowing specialist will tell you when to start these exercises. Exercises will not be beneficial if you start them too soon after surgery or too early before radiation treatment.
Perform each exercise 10 repetitions 3 times a day. If your swallowing specialist tells you to do them more often or less often, follow these recommendations.
Exercises to improve swallowing
Tongue holding exercise (Masako exercise)
- Place the tip of your tongue between your front teeth.
- Swallow. While swallowing, hold your tongue between your front teeth.
Between swallows, you can relax and return your tongue to its normal position.
Forceful swallowing exercise
- Swallow as usual, but tense the muscles of your throat and tongue.
Imagine swallowing something large (like a spoonful of peanut butter). This will help you tighten your muscles a lot.
Mendelssohn swallowing exercise with maneuver
- Swallow as normal, but when you feel your throat and Adam's apple rise, pause for 2 seconds before relaxing your muscles at the end of the swallow.
To pause, you can imagine holding your breath as you take a sip for 2 seconds before relaxing. You can also touch your hand to your throat to feel when the muscles rise or tense as you swallow.
Swallowing exercise for the supraglottic area
- Inhale and hold your breath.
- Hold your breath and swallow.
- Forcefully exhale or cough out any trapped air.
Shaker exercise
- Lie down on the floor or bed.
- Raise your head as if you were looking at your toes.
- Lower your head to the starting position.
- Repeat this movement 30 times.
- After this, raise your head. Hold it in this position for 60 seconds, or as long as you can. Then relax.
Exercises on the range of motion of the tongue
Tongue protrusion exercise
- Stick your tongue out as far as possible until you feel a good stretch.
- Hold it in this position for 5 seconds.
Tongue retraction exercise
- Retract your tongue into the back of your mouth as if you were gargling or yawning.
- Hold it in this position for 5 seconds.
Tongue retraction exercise
- Move your tongue to the left as far as possible until you feel a good stretch.
- Hold it in this position for 5 seconds.
- Move your tongue as far to the right as possible until you feel a good stretch.
- Hold it in this position for 5 seconds.
Exercise for the tip of the tongue
- Press the tip of your tongue against the back of your upper teeth or gums.
- Holding it in this position, open your mouth as wide as possible for 5 seconds.
Exercise for the root of the tongue
- Say the sound “k” or “ka” loudly. To do this, you should move the root of your tongue to the back of your throat.
Jaw Exercises
Range of motion and stretching exercises
Sit or stand. Your head should remain in one position while performing these exercises.
- Open your mouth as wide as possible until you feel a good stretch but no pain (see Figure 2). Hold this position for 10 seconds.
- Move your lower jaw to the left (see Figure 3). Hold this position for 3 seconds.
- Move your lower jaw to the right (see Figure 4). Hold this position for 3 seconds.
- Make circular movements with your lower jaw to the left.
- Make circular movements with your lower jaw to the right.
Figure 2. Open your mouth
Figure 3: Move your jaw to the left
Figure 4: Move your jaw to the right
Passive stretching exercise
Figure 5. Give extra support with your fingers.
- Press your thumb against your upper front teeth.
- Press the index finger of your other hand against your lower front teeth (see Figure 5).
- Open your mouth as wide as possible. Place additional emphasis with your fingers so that your mouth does not close. You should feel a slight stretch, but not pain.
- Hold this position for 15-30 seconds.
If your swallowing specialist notices any changes in your ability to swallow, they may give you other exercises or tell you about other ways to maintain swallowing function during treatment.
to come back to the beginning
Endotracheal anesthesia - indications
In plastic surgery, endotracheal anesthesia is used for many operations.
Examples include rhinoplasty, augmentation mammoplasty, abdominoplasty, mastopexy, circumferential facelift and SMAS platysmaplasty. Liposuction can also be performed using an intubation technique, although local anesthesia may be chosen for smaller cases. Endotracheal anesthesia is indicated for all long-term operations accompanied by a violation of the integrity of deep tissues, not only the skin. This is how a general rule can be formulated. Minor surgical interventions are often performed under local anesthesia. Examples are otoplasty for protruding ears, bullhorn (a type of lip surgery) or lipoma removal.
After endotracheal anesthesia
The final stage of general anesthesia is the removal of the patient from the state of drug-induced sleep. After endotracheal anesthesia, some confusion is observed, which is explained by the residual effect of sedatives on the central nervous system. Possible headaches, mild dizziness and nausea are associated with this. However, the features of modern anesthesia drugs are such that while the patient may be bothered by their residual effect, he is in a state that resembles euphoria. And when the euphoria wears off, the “echoes” of anesthesia also disappear.
A specific phenomenon after endotracheal anesthesia is a slight sore throat, sore throat, and possibly a cough. These consequences are explained by the fact that the endotracheal tube irritates the mucous membrane of the larynx and trachea. As a rule, the discomfort goes away within a day.
How cancer and radiation therapy may affect swallowing
Depending on the size and location of the tumor, radiation therapy may weaken the muscles and organs involved in swallowing. They also may not work as well as they did before radiation therapy began. This may make it difficult for you to eat and drink.
Radiotherapy may cause:
- pain when swallowing;
- wounds (inflammation of the mucous membrane) in the mouth and throat;
- dry mouth.
- unusually thick saliva;
- swelling.
- Change in taste sensations
These symptoms usually appear 1-2 weeks after starting radiotherapy. These symptoms may become worse during treatment. Most symptoms will begin to subside approximately 2 to 4 weeks after treatment ends.
Radiation therapy can also cause permanent tissue scarring. The impact of such scars depends on which area is being treated. Some examples of the effects of scarring are described below.
- The muscles that attach to your jaw may tighten, making it difficult for you to open your mouth and chew food. This is called trismus.
- Your salivary glands may not produce enough saliva. This may make swallowing more difficult because your mouth will be too dry.
- The muscles in the tongue and back of the throat may also lose mobility. This may make it more difficult for you to push food or liquid down your throat and open your esophagus.
- The muscles that help protect the airway when swallowing may weaken. They may not be strong enough to prevent food or liquid from entering the airways.
- The esophagus may narrow. For this reason, food may get stuck in the back of the throat.
Not all patients will necessarily have all of these problems. Your treatment will be planned to reduce the likelihood of these problems occurring. Your healthcare team will also teach you techniques that can help you cope with these problems.
Other treatments may also affect swallowing. The surgery may affect areas of the mouth and throat, which may make swallowing difficult. Some chemotherapy drugs can cause sores in the mouth and throat. This can make swallowing painful.
to come back to the beginning
Complications of endotracheal anesthesia
Any surgical intervention is associated with the risk of postoperative complications. The goal of using endotracheal anesthesia is to minimize this risk. Thanks to the intubation technique for administering medications, the risk of aspiration of gastric contents into the lungs is reduced, the risk of respiratory tract infection, and the risk of respiratory or cardiovascular failure is minimized.
Complications of endotracheal anesthesia, that is, complications caused by the insertion of an endotracheal tube, are extremely rare. These include injuries to the tongue or larynx, which occur during intubation “on the go” before urgent (urgent) operations. During planned surgical interventions, which include all plastic surgeries, there are no complications of endotracheal anesthesia.
Endotracheal anesthesia - contraindications
Endotracheal anesthesia has become very widely used in all branches of surgery, largely due to the fact that it has practically no contraindications. Intubation technology allows for complete control of vital functions; it can even be used to perform 16-hour heart surgeries.
In the context of plastic surgery, endotracheal anesthesia has no contraindications. Why? Because intubation cannot be used only for certain conditions in which any operation not related to the elimination of an immediate threat to life is contraindicated. For example, endotracheal anesthesia is contraindicated in case of myocardial infarction or pneumonia, but no one would even think of undergoing plastic surgery.
To learn more about the anesthetic techniques used for a particular plastic surgery procedure, book a free consultation with a Soho Clinic surgeon.
Tonsil removal methods
In modern otorhinolaryngology, there is a wide choice of tonsillectomy techniques.8
Classic method of removing tonsils
Removal of tonsils occurs by bluntly separating the tonsil tissue along with the capsule from the surrounding tissues using a rasp.
The separation of the tonsil is completed using a wire loop. The bleeding is stopped, the vessels are cauterized using an electrosurgical method (electrocoagulation). This operation takes from 15 to 40 minutes.9 Today, this operation is used in ENT practice more often than others. The operation can be performed under general or local anesthesia.
The only disadvantage of this method, unlike others, is the highest risk of bleeding. However, the operation is fairly routine and, relative to the number of operations performed, the risks of complications are low.
Laser method for tonsil removal
When removing tonsils, a laser beam is used to destroy and coagulate tissue. The laser beam coagulates the blood at the incision site and seals the blood vessels, which prevents bleeding. The laser method is less traumatic and has a lower risk of complications. Also, in this way it is possible both complete removal of the palatine tonsils and their partial excision.
Radio wave method for removing tonsils (using the Surgitron device)
Tissue excision occurs using a radio signal, which is transmitted by an electrode and causes the evaporation of intracellular fluid and tissue dissection.
The advantage of this method is that thermal damage to tissue is several times lower than when using laser or electrosurgical methods. There is less tissue injury, as a result of which the patient experiences less pain in the postoperative period; the level of tissue regeneration is maintained. Complete tissue healing occurs without the formation of a rough scar.
Cryodestruction
This method of removing tonsils involves local exposure to liquid nitrogen using a special nozzle.
The nozzle is selected individually, taking into account the peculiarities of the anatomy, since its contact with the palatine tonsil must be especially clear and dense for a more effective effect. Cryotherapy causes microcirculation disturbances, which ensures the absence of bleeding during and after surgery. This method is painless and bloodless, and does not form a rough scar. The method is recommended for patients with an increased risk of bleeding, severe heart failure and pathology of the endocrine system.