I. K. Lutskaya Head of the Department of Therapeutic Dentistry BelMAPO (Minsk)
HIV infection is a disease caused by the human immunodeficiency virus, which occurs with damage to the immune and nervous systems and is manifested by the development of severe infectious (parasitic) diseases and/or malignant neoplasms, as well as signs of encephalomyelopathy. AIDS (acquired immunodeficiency syndrome) is the final (terminal) stage of HIV infection.
The infectious process in the human body (from the moment of infection with the human immunodeficiency virus until the death of the patient) is characterized by a long incubation period (from several months to 5 or more years), a slow course, and selective damage to T-lymphocytes and neuroglial cells.
Epidemiology
The only source of infection is a person infected with this virus. The most dangerous are those who do not have any clinical manifestations: virus carriers are the main source of the spread of HIV infection among the population.
During a dental appointment, infection can occur in the following cases:
- when using medical instruments contaminated with blood or other biological fluid that have not been disinfected (various devices, discs, burs, probes, needles, syringes, cutting and piercing instruments, etc.);
- in the presence of wound surfaces and ulcerations in the oral cavity;
- in case of extensive contamination of the skin of healthcare workers with blood, blood getting into the eyes;
There are known examples of infection during acupuncture treatment.
(There is no airborne transmission of infection.)
The immunodeficiency virus is found in the highest concentration in the blood. Next in descending gradation are sperm, vaginal and cervical secretions of the glands, breast milk, and saliva. Blood and other specified biological fluids are factors in the transmission of HIV from an infected person to other persons.
The virus is moderately resistant outside the human body. In the external environment (biosubstrates), its infectious effect lasts up to 2 weeks, in a dried state (discharge on linen, objects, etc.) - up to 1 week. Radiation exposure and ultraviolet rays do not affect it. When boiled, the virus dies within 5 minutes; when heated to 56°C, inactivation occurs after 30 minutes. Disinfectants used in the practice of medical institutions (chloramine, calcium hypochloride, hydrogen peroxide, alcohol, etc.) in concentrations provided for the disinfection of hepatitis viruses are guaranteed to destroy HIV upon direct contact of the disinfectant with contaminated blood or other human biological fluid on the surface of an object, including a hollow one ( internal surfaces of the syringe, needles, capillaries, probes, etc.).
Transmission of infection and its development
The source of infection is a person in whose body the immunodeficiency virus is present. The virus is transmitted through biological fluids (blood, semen, vaginal secretions, breast milk). There are several routes of transmission: sexual, from mother to child and parenteral (during medical interventions, for example, during operations, blood transfusions, organ transplants and others).
In the early stages, HIV infection is asymptomatic or similar to other diseases. Later, due to weakened immunity, it is joined by multiple secondary infections, which the body of healthy people can usually resist. These are sore throat, pneumonia, candidiasis, herpes virus infection, stomatitis and other diseases that often accompany HIV. Cardiovascular, neurological, endocrine and osteoarticular pathologies gradually develop.
The final stage of infection is acquired immunodeficiency syndrome (AIDS). If left untreated, the syndrome develops on average within 2–15 years. AIDS is characterized by multiple severe infections and cancers that affect all organ systems. These are, for example, lymphomas, Kaposi's sarcoma, tuberculosis, meningitis and other diseases.
It is currently impossible to cure HIV infection. However, so-called antiretroviral therapy makes it possible to curb the development of the disease, significantly improving the quality and increasing the life expectancy of patients.
Clinic
The incubation period for HIV infection is 1–3 months, but can be longer. After this, the initial stage of the disease develops, called acute HIV infection.
Only 20% of infected people develop clinical signs in the form of a general infectious syndrome of an undifferentiated nature (mononucleosis-like manifestations, serous meningitis, encephalopathy, myelopathy or neuropathy).
A clinically favorable outcome of the acute stage of the disease does not mean either the acquisition of immunity or recovery, despite seroconversion. The disease progresses to a chronic stage, which occurs either subclinically or in the form of persistent generalized lymphadenopathy with a constant subtle transition to the AIDS-associated syndrome.
Patients remain active, productive and in good health. There are no signs of immunosuppression yet.
Prognostically unfavorable is a decrease in the size of the lymph nodes, which means involution of the follicles - a morphological sign of immunosuppression.
Clinical symptoms of the AIDS-associated stage of the disease consist of signs of initial immune deficiency. They are manifested by local infections of the skin and mucous membranes caused by low-pathogenic representatives of microflora of an opportunistic nature (viral and bacterial stomatitis, pharyngitis, sinusitis, oral, genital, perianal herpes, recurrent herpes zoster, candidal stomatitis, genital and perianal candidiasis, dermatomycosis of the feet, legs, impetigo , acne folliculitis, hairy leukoplakia of the tongue, etc.).
Lesions of the skin and mucous membranes are initially easily amenable to conventional therapy, but quickly recur and gradually become chronically recurrent in nature. The most important feature of the clinical picture of the AIDS-associated complex is the steady increase in symptoms with the worsening of existing lesions and the appearance of new lesions.
The chronic stage of the disease gradually moves into its final stage - AIDS. By this time, immune functions are suppressed and disturbed to the maximum (CD-4 lymphocytes are reduced to 100 per 1 mm3).
According to available observations, 5 years after infection, from 25 to 50% of people develop AIDS, after 7 years - up to 75%, after 10 years (observations since 1981) - slightly more than 90% of those infected. Can the remaining 10% not get sick? They can if the latent period of the disease turns out to be longer than the remaining years of their life.
Infections - the most common and dangerous manifestation of AIDS - develop in the form of localized, generalized and septic forms. The skin, mucous membranes, and internal organs are affected.
The clinical features of infectious processes in AIDS are their increasing nature, prevalence, severity, atypical symptoms and multiplicity of localizations.
The main diseases that manifest themselves in AIDS on the oral mucosa, depending on the etiotropic factor, are grouped as follows.
1. Fungal infections:
- candidiasis (pseudomembranous, erythematous, hyperplastic - in the form of a plaque or nodes, angular cheilitis);
- histoplasmosis.
2. Bacterial infections:
- fusospirochetosis (ulcerative-necrotizing gingivitis);
- nonspecific infections (chronic periodontitis);
- mycobacteria, enterobacteria.
3. Viral infections:
- herpetic stomatitis;
- hairy leukoplakia;
- herpes zoster (shingles);
- xerostomia caused by cytomegalovirus.
4. Neoplasms:
- Kaposi's sarcoma in the oral cavity;
- squamous cell carcinoma;
- Non-Hodgkins lymphoma.
5. Lesions of unknown etiology:
- recurrent ulcerating aphthae;
- idiopathic thrombocytopetic purpura (ecchymoses);
- lesions of the salivary glands.
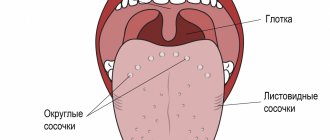
What does a healthy tongue look like?
Note! The tongue of an absolutely healthy person is pink, soft with clearly visible taste buds.
A smooth groove can be seen in the center , dividing the tongue into two equal parts.
Moving your tongue while eating, drinking or talking does not cause discomfort. A small amount of white coating on the tongue is a type of normal .
Its thickness may vary depending on the time of year and the food eaten the day before. As a rule, it can be easily cleaned with a regular toothbrush.
Also, that has just begun to progress in the body can lead to the appearance of a whitish coating
- candidiasis;
- caries;
- gingivitis;
- inflammation of the gums.
Stay up to date! Separately, it is worth mentioning problems with the gastrointestinal tract.
Allergies, lack of nutrients and dietary fiber are often the cause of the appearance of a whitish or yellowish coating.
When the plaque begins to thicken and cannot be removed even with a brush, this is a reason to immediately contact a specialist.
It is likely that in this way the body signals an exacerbation of a chronic disease or infection.
Fungal infections
Candidal stomatitis is diagnosed in the vast majority of AIDS patients (up to 75%) and manifests itself in several clinical forms.
Pseudomembranous candidiasis often begins as acute, but with AIDS it can continue or recur, and therefore is considered as a chronic process. Fungal infection is characterized by the presence of a yellowish coating on the oral mucosa, which may be hyperemic or unchanged in color. Plaque is tightly held on the surface of the epithelium and is difficult to remove. This exposes bleeding areas of the mucosa. The favorite localization of plaque is the cheeks, lips, tongue, hard and soft palate (Fig. 1).
Rice. 1. Pseudomembranous candidiasis. Raid in the sky.
Erythematous, or atrophic, candidiasis develops in the form of bright red spots or diffuse hyperemia, and in AIDS it has a chronic course. The palate is most often affected and acquires an uneven bright red color. The epithelium becomes thinner and erosions may appear. Localization of lesions on the dorsum of the tongue leads to atrophy of the filiform papillae along the midline (in contrast to this picture, age-related changes in the tongue are characterized by diffuse atrophy; in syphilis, atrophy of the filiform papilla takes the form of foci of a mowed meadow) (Fig. 2).
Rice. 2. Erymatous candidal glossitis.
Chronic hyperplastic candidiasis is characterized by the symmetrical arrangement of elements on the mucous membrane of the cheeks in the form of polygonal elevated foci of hyperplasia, covered with a yellow-white, cream, yellowish-brown coating. The hyperplastic form of candidiasis is much less common. Researchers attribute this manifestation to exposure to nicotine from smoking (Fig. 3).
Fig.3. Hyperplastic candidiasis.
Fungal infections of the oral mucosa can be combined with candidiasis of the corners of the mouth - angular cheilitis, which is a sign of generalization of the process.
The diagnosis, which is made on the basis of clinical manifestations, must be confirmed by laboratory tests. Active growth of a large number of colonies (hundreds) on a nutrient medium, detection of mycelium during microscopy of samples indicate the pathogenicity of the Candida fungus. In some cases, a biopsy is necessary.
Treatment of candidiasis can be systemic or local, depending on the extent of the process. Etiotropic effects are mandatory, symptomatic effects depend on clinical manifestations.
Bacterial infections
Ulcerative-necrotizing gingivitis develops in HIV-infected individuals both during various periods of clinical manifestations of AIDS, and without them in the presence of antibodies against the virus. Patients complain of pain and bleeding gums while brushing their teeth and eating; bad breath. Upon examination, a gray-yellow plaque (necrotic film) is found covering the gingival margin and interdental papillae. The mucous membrane in the gum area is hyperemic, swollen, and tense.
After treatment, the symptoms disappear, but there is a tendency to relapse. A prolonged course can lead to deep ulcers with damage to bone structures and necrotization of the interdental septum (Fig. 4).
Rice. 4. Herpes simplex on the lip.
The consequence of gingivitis is periodontitis (periodontitis) with irregular generalized destruction of bone tissue and the supporting-retaining apparatus of the tooth. Treatment of patients does not provide lasting results.
What is HIV infection and AIDS
HIV infection is a disease caused by one of the representatives of the group of retroviruses, causing the gradual development of immunodeficiency.
A characteristic feature of the disease is slowly progressive damage to the immune system, AIDS - human immunodeficiency syndrome, up to the development of the terminal (fatal) stage. The human immunodeficiency virus was first isolated in 1983. Since then, the disease has claimed about 32 million lives [2]. According to WHO, HIV is a major global public health problem. This virus is widespread, so many dental specialists may encounter its manifestations when examining the oral cavity of patients carrying HIV. For example, according to 2022 data, over 1 million people live in Russia with only a laboratory-diagnosed diagnosis [3].
The disease is characterized by extensive damage to the immune system. At the same time, the body’s defense against infections and certain types of cancer is significantly weakened, which manifests itself in autoimmune reactions, immune pathologies and metabolic disorders that lead to damage to blood vessels and connective tissue.
Viral infections
In HIV-infected people, the most common manifestations of stomatitis are caused by the herpes simplex virus. Primary infection with the herpes virus occurs in children, adolescents, and, less commonly, young adults. Since the infection is latent, there is a tendency to recur, and manifestations can be both general (fever, pain when swallowing, swollen lymph nodes) and local. Acute herpetic rashes can be localized in any part of the maxillofacial area. Favorite places are lips, gums, hard palate. The initially small bubbles that form then merge into larger ones. After the destruction of the tire, the underlying tissues tend to ulcerate. In the oral cavity, the bubbles burst very quickly, and usually erosion is immediately detected. On the red border of the lips, the vesicles of the blisters shrink, forming dry or weeping crusts.
The herpes virus can cause generalized lesions up to and including herpes encephalitis.
Recurrent herpetic stomatitis is most often localized on the red border of the lips with the involvement of surrounding areas of the skin. The blisters quickly enlarge, merge, and a secondary infection develops. The contents of the blisters suppurate, resulting in the formation of crusts of a dirty yellow color; after their separation, an eroded or ulcerated surface is exposed (Fig. 5).
Rice. 5. Viral wart.
The lesions on the hard palate and gums are represented by small bubbles that quickly burst, leading to ulcerative lesions of the mucous membrane. Clinical manifestations can be triggered by a cold, stress, or respiratory infection (Fig. 6).
Rice. 6. Hairy leukoplakia on the lateral surface of the tongue.
Shingles (herpes zoster) in the oral cavity and on the face is characterized by asymmetry of the lesion according to the area of innervation of one of the branches of the trigeminal nerve. It is also possible that two or three branches of trigeminus are involved, when elements appear on the mucous membrane in the form of small blisters and then an ulcerated surface. The rash is preceded by burning pain, simulating pulpitis of intact teeth, radiating along the maxillary or mandibular branch of the fifth pair of nerves. These pains may persist even after involution of the lesions (up to 1–2 months).
Viral growths come in the form of warts, papilloma, genital warts and frontal epithelial hyperplasia (papules or nodular lesions with filamentous growths).
Warty formations are localized in the corners of the mouth. They may have the appearance of a papilloma, ridge, or protrusions (Fig. 7).
Rice. 7. Hairy leukoplakia of the ventral and dorsal surface of the tongue.
Genital warts. Depending on the location, the lesion elements can have different appearances: multiple pointed protrusions or rounded, slightly raised areas with a flat surface. When localized on the gum or hard palate, the lesions appear as multiple pointed projections. When located on the cheeks and lips, the elements have a picture similar to focal epithelial hyperplasia: rounded, slightly raised areas with a diameter of about 5 mm with a flattened surface.
Hairy leukoplakia. The lesion is localized, as a rule, on the tongue, having different sizes and appearance. It is found in limited areas of the lateral, dorsal, ventral surface or covers the entire tongue. The mucous membrane takes on a whitish appearance, but hyperkeratosis does not develop. On palpation, the seals are not detected, which served as the basis for designating this form of lesion: soft leukoplakia (Fig. 8).
Rice. 8. Kaposi's sarcoma on the skin of the face.
On the lateral surface of the tongue, elements can be located bilaterally or unilaterally (Fig. 9). The mucous membrane, over a limited or widespread area, becomes irregular and rises in the form of folds (“corrugated”) or projections above the surrounding surface, which may resemble hair in appearance. Hence the name - hairy leukoplakia.
Rice. 9. Kaposi's sarcoma on the palate.
On the lower surface of the tongue, the focus of epithelial opacification may be smooth or slightly folded. Much less commonly, soft leukoplakia occurs on the cheeks, floor of the mouth, and palate.
There are no subjective sensations other than discomfort.
Hairy leukoplakia can be combined with candidal glossitis, confirmed by laboratory methods. However, treatment of candidiasis does not affect the appearance of the lesion.
Histological, virological, including serological, studies give reason to believe that the cause of soft hairy leukoplakia is the Epstein-Barr virus.
Soft leukoplakia must be differentiated from leukoplakia, lichen planus, chemical or electrical burn, and chronic hyperplastic candidiasis.
Useful video
From this video you will learn about tongue lesions due to HIV infection:
Unfortunately, today there are no specific means to get rid of HIV infection. However, everyone can do everything they can to reduce the likelihood of infection.
Carefully monitor your own health and try to listen to the signals that your body gives you.
Even such a typical and common ailment as a coating on the tongue can occur as a result of HIV infection.
Manifestations of neoplasms in the oral cavity
Kaposi's sarcoma is a vascular tumor (lympho- and hemovascular), which, in the absence of HIV infection, is characterized by a low-grade course, occurring in residents of African countries. In AIDS, Kaposi's sarcoma can appear in young people as red, rapidly turning brown spots that are initially found on the legs, but tend to spread. They differ from the classic version by increased malignancy and dissemination on the skin, mucous membranes, and internal organs.
The characteristic brown spots of Kaposi's sarcoma on the face are the “calling card” of AIDS patients, occurring in 30% of HIV-infected individuals, regardless of country of residence. The lesion elements are initially represented by single, and more often multiple, spotted, papular (nodular) formations of pink, red, purple colors on the skin (Fig. 10).
Rice. 10. Kaposi's sarcoma with ulcerations and hyperplasia.
In the oral cavity, Kaposi's sarcoma is most often localized on the palate; in the early stages of development it looks like a blue, red, black flat spot. In subsequent stages, the lesions darken, begin to rise above the surface, become lobulated, and finally ulcerate, which is especially typical when located in the oral cavity. The entire surface of the hard and soft palate can change, becoming deformed due to the formation of both tuberosity and ulcerative defects. The mucous membrane of the gums may also be involved in the process. Moreover, in some cases, the lesion element looks like epulis (Fig. 11).
Rice. 11. Kaposi's sarcoma in the form of epulis.
The etiological factor of Kaposi's sarcoma is still unclear.
People with AIDS may develop squamous cell carcinoma, which is usually located on the tongue and occurs in young people. Treatment with immunosuppressive drugs reduces the incidence of malignancy in tumors, including intraoral carcinoma.
Diagnosis of rashes on the body
With HIV and AIDS, it is difficult to visually determine the type of rash - the nature of skin inflammation in infected people is different.
To determine the type of rash and its cause, the following diagnostic measures are carried out:
- Clinical analysis of blood and urine.
- Blood test for sexually transmitted viruses.
- Skin scraping. The method is used to detect intradermal mites and fungi that cause skin diseases.
- Blood tests for antibodies to allergens and allergy skin tests.
- Hormonal studies.
- Biopsy of skin lesions. They detect the presence of cancer cells, which is important for diagnosing Kaposi's sarcoma.