Many parents are concerned not only with the psycho-emotional development of the child and issues of general health, but also with such particular issues as, for example, the development of the child’s dental system. In many countries around the world, such attention is a common part of the dental culture, combining prevention, hygienic care and regular follow-up with appropriate specialists. Russia, unfortunately, is not in first place in terms of development of dental culture. In this article we will tell you more about the growth of a child’s jaws, possible developmental anomalies, what and at what age you need to pay attention, and which specialists you should contact if you notice any abnormalities.
The human maxillofacial apparatus develops along with the growth of the child and goes through various stages of development. Thus, the growth of the alveolar processes in width ends around 3 years of age. At this time, you can show the child to an orthodontist so that he can determine the presence or absence of any dental anomalies. By the age of 3, children usually finish erupting their baby teeth. From this moment on, the width of the alveolar processes no longer changes. Further, the alveolar processes will only lengthen. This process usually occurs between the ages of 6 and 12 years, when children's molars erupt.
The bite is formed in stages: temporary – replaceable – permanent.
Temporary milk bite
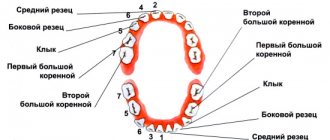
A primary dentition is a dentition made up of baby teeth. These teeth received this name because of their milky white color. The eruption of baby teeth begins around 6-8 months (earlier and later eruption is possible).
The appearance of the last baby tooth occurs at about 2 and a half years of age. There are a total of 20 teeth in the primary occlusion - 10 each on the upper and lower jaws. In the primary dentition, space is prepared for future permanent teeth: thus, at the age of about 5 years, the spaces between the incisors widen.
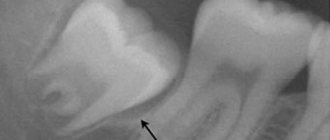
A panoramic image (orthopantomogram) shows not only grown teeth, but also the presence of the rudiments of permanent teeth.
Predicting growth using x-rays of the hand and vertebrae
The development of the dentofacial system correlates with the patient’s age. Skeletal age is determined by the degree of ossification (ossification) of bone structures. During the process of maturation, each bone undergoes changes that are determined radiographically. The sequence of changes is constant for all people.
The degree of growth of the lower jaw can be assessed by the condition of the cervical spine. The assessment is made visually and consists of two parameters: the shape of the vertebra and the presence of concavity at its lower border. The connection between the increase in the length of the lower jaw (body and ramus) and the stage of development of the cervical vertebrae has been scientifically proven.
As a vertebra grows, its shape changes, which makes it possible to assess the degree of maturity. An important point in the analysis is to determine the degree of concavity of its lower surface.
At the very beginning, young immature vertebrae have a rectangular shape. The lower surface of the vertebra is flat or slightly concave. (Fig. 1) Peak growth is expected no earlier than a year after this stage.
As they mature, the vertebrae become increasingly concave on the lower surface, remaining rectangular and horizontal in shape. (Fig. 2) The most active period of growth has already occurred a year or two before this stage.
Upon final maturation, the vertebra acquires a concavity of the lower surface, its shape becomes rectangular, vertical or square. (Fig. 3) This indicates that the peak of growth occurred no later than two years ago before this stage.
The use of this method is relevant when predicting the growth of the lower jaw, for example, when treating with functional devices.
Another method for assessing the degree of growth is an x-ray of the hand. To analyze skeletal maturity up to approximately 9 years of age, the degree of mineralization of the carpal bones, the development of the metacarpal bone and phalanges are used.
The assessment consists of determining the ratio of the sizes of the epiphysis (the widened end of the tubular bone) (Fig. 4) to the diaphysis (the central part of the tubular bone). (Fig.5)
The equal width of the diaphysis and epiphysis is designated as “=” (Fig. 6), the coverage of the diaphysis by the epiphysis in the form of a cap is “cap” (Fig. 7), with complete ossification – “unit(u)” or also “closed (c)” . (Fig.8)
In newborns, signs of carpal bones appear from the 3rd month of life.
An X-ray of a child’s hand is characterized by the “=” and “cap” stages. (Fig.9)
Rice. 9
An x-ray of an adult’s hand is characterized by the “closed” stage. (Fig.10)
Rice. 10
In modern orthodontic practice, determining height using an x-ray of the hand is performed, for example, before orthognathic surgery.
Changeable bite
Between the ages of 6 and 12 years, a gradual change of teeth occurs when baby teeth fall out and are replaced by permanent ones. Doctors call this condition a mixed dentition. If your child is already being seen by an orthodontist, then changing the bite is an important stage, which should also take place under the supervision of a specialist. The process of changing the bite looks like this: the first molar erupts behind the last milk tooth. It is important that baby teeth are healthy - only in this case the change in bite occurs normally.
It is not recommended to remove baby teeth prematurely without special medical indications. It is also not recommended to ignore the treatment of baby teeth, believing that “they will fall out anyway.” The first large permanent molar—the “six”—erupts behind the baby teeth when baby teeth have not yet begun to fall out.
Using a panoramic photograph of the jaws, the doctor monitors the change of teeth, the presence of the rudiments of permanent teeth and the depth of their location.
The Dial-Dent clinic places great importance on dental treatment for young patients. Healthy baby teeth are the key to healthy permanent teeth. In addition, timely and regular observation of the child by a pediatric dentist will allow his dental and orthodontic problems to be resolved in a timely manner. Unfortunately, it is still not uncommon now for a desperate mother to come to the clinic and ask to have her baby’s bad teeth treated under anesthesia. It is difficult for a dentist to understand why the parents did not pay attention to the child’s condition earlier, when the treatment would not have been so difficult and traumatic for the little patient...
Concept and reasons for origin
The term “small lower jaw” in dentistry and orthodontics has several interpretations with significant differences:
- Micrognathia (also microgenia) is a pathology manifested in the form of defective or delayed development of the entire lower jaw, as well as its individual fragments;
- Prognathia is an intensive growth of the upper part of the jaw apparatus, which results in the visual effect of insufficient development of the lower jaw.
Both pathologies manifest themselves in both infancy and adulthood. Clinical manifestations of the anomaly make it possible to detect the presence of abnormalities at the primary stages of development, which provides the possibility of preventive treatment.
In children
In infancy, improper formation of the lower jaw is caused by various factors, the main one of which is a violation of the uniform process of fetal development in the prenatal period. At this stage, the relationship of jaw proportions is established, which can be influenced by:
- improper maternal diet;
- presence of genetic predisposition;
- consumption of nicotine and alcohol products;
- exposure to serious illnesses with complications.
In the early stages of a child’s life, factors influencing the development of pathology are:
- late formation of bite;
- metabolic disorders in the body;
- early loss of baby teeth;
- bad habits (pacifiers, pacifiers);
- improper feeding.
The primary signs of small lower jaw syndrome in children are recession of the chin and lower lip, abnormal tooth growth and impaired sucking function. Timely identification of symptoms allows the anomaly to be stopped without the use of orthodontic treatment methods.
In adults
In older age, factors provoking the formation of pathology are:
- incorrect or incomplete treatment in childhood;
- receiving severe injuries to the jaw apparatus;
- disorders of the body's metabolic processes;
- pathologies formed in bone tissue (rickets, ostiomyelitis);
- abnormal development of the orbicularis oris muscle.
Characteristic manifestations of small lower jaw syndrome in adulthood are distortion of the patient’s facial features, deformation of the dentition, and problems with eating solid foods.
Permanent bite
After all primary teeth have been replaced and the second molars (“sevens”) have erupted, the formation of a permanent dentition is considered complete. In an ideal permanent dentition, after changing teeth, the upper incisors should overlap the lower incisors by 2 mm. To assess the correct bite, it is also necessary to pay attention to the relationship and contact of the upper and lower teeth. At this age, your child is most likely already visiting a dentist, who, if necessary, will provide a referral for a consultation with an orthodontist. The last stage of teething will occur at the age of 18-20 years, when wisdom teeth appear. Sometimes there is not enough space for them to grow, or they may be in an incorrect position. In these cases, you may need to consult a dental surgeon.
A person needs a correct bite not only for beauty and beautiful speech, but also for the normal functioning of the maxillofacial apparatus. Poorly chopped food can lead to diseases of the gastrointestinal tract and the entire body as a whole. Over time, malocclusion can cause headaches and poor health. An uncomfortable psychological state also plays an important role for a person with malocclusion. That is why we recommend that you pay attention to the condition of your child’s teeth and promptly listen to the advice of doctors. The sooner you start orthodontic treatment, the better the results will be.
The Dial-Dent clinic has a newly created orthodontic department, headed by orthodontist O.A. Baranova. She specializes in correcting bites in adult patients and solves any, even the most complex cases. If you are concerned about your child’s malocclusion, then it is best to contact pediatric specialist E.V. Rada, the owner of numerous diplomas, certificates and certificates.
Dial-Dent specialists, whom you can contact for advice on the condition of your child’s oral cavity:
- Borisova Yulia Aleksandrovna, pediatric dentist.
- Nazarenko Evgenia Yurievna, pediatric dentist.
- Rada Elizaveta Valerievna, dentist-orthodontist, correction of bite in children.
- Selector Olga Nikolaevna, dentist-orthodontist, bite correction in children.
- Sleptsova Maria Pavlovna, dentist-orthodontist, bite correction in children.
- Tsukor Tatyana Borisovna, speech therapist - child psychologist.
- Smirnova Elena, dental hygienist.
Features of the period
The physiological replacement of temporary teeth with permanent ones is completed by the age of 12 years of a child’s life. At this moment, the teenager should have 24 permanent teeth in the oral cavity: canines, incisors, first molar, first and second premolars.
The eruption of the seventh tooth (second molar) begins at age 13. And by the age of 18, the “wisdom” tooth, that is, the third molar, may begin to emerge.
Causes of hyperplasia
(MG) is caused by overdeveloped, aggressive growth of the condyle. This condition causes abnormal jaw growth, which means one side of the jaw stops growing earlier. Juvenile idiopathic arthritis (JIA) and condylar fractures can cause growth and mandibular problems. Inflammatory and/or mechanical damage to the condylar cartilage often causes jaw hyperplasia.
Symptoms of inferior hyperplasia
Symptoms include slowly progressive unilateral growth of the condyle of the head and neck. This results in malocclusion, facial asymmetry, and a shift to the middle of the chin on the unaffected side. Characteristics of condylar hyperplasia may also include: a posterior open bite or tilted occlusal plane, depending on the time at which the hyperplasia develops, and asymmetry of the lower half of the face. Characteristic symptoms of lower hemisphere hyperplasia are asymmetrical facial bones (enlarged lower facial bones on one side).
Surgical treatment of mandibular hyperplasia.
If the height of the mandible is significantly increased, facial symmetry may be improved by surgical reduction of the lower edge of the jaw. High condylectomy surgery effectively stops disproportionate jaw growth while maintaining normal jaw function. Patients with active hyperplasia are treated with high condylectomy, articular disc reduction, and orthognathic surgery. The pathogenesis is most likely related to a disorder of condylar hyperactivity, which can be documented histologically by actively proliferating cartilage. Hyperplasia of the hemimandibular, including the condyle, requires more careful treatment planning compared to these anomalies limited to the ramus and body of the mandible, which require an accurate diagnosis to ensure appropriate treatment.
What can cause hypoplasia of the lower jaw?
Mandibular hypoplasia tends to be a congenital condition, however, it can definitely occur due to trauma or. Mandibular hypoplasia indicates an incomplete jaw. The radiographic appearance of maxillary and mandibular lesions often includes radiolucency with poorly defined or even irregular diffuse borders. Expansion of the orbital border usually creates hypoplasia and poor pneumatization of the ipsilateral maxilla. Possible hypoplasia of the body of the lower jaw, an abnormal coronoid process, as well as a zygomatic arch.
What is mandibular hyperplasia?
Hyperplasia is characterized by a constant or rapidly growing condyle when growth should be slowed or stopped. This condition causes development of the head, neck and jaw, causing significant functional and aesthetic deformities of the face. Disorders of the dental craniofacial structure affect the normal growth of the jaw, which leads to gross changes in the normal morphology and structure of the hard and soft overlying tissues. The result is asymmetry and significant functional deformities, which pose a serious problem for both orthodontists and maxillofacial surgeons.