Detailed description of the study
Salivary gland cancer is a malignant tumor of the salivary gland formed from epithelial cells. Tumors of the parotid salivary glands (PST) are a rare type of neoplasm. They mainly develop between the ages of 20 and 40. More common in men than in women. Tumors are usually located in the soft tissues of the face and often cause serious cosmetic defects, causing paresis of the facial nerve.
The main risk factors for developing salivary gland cancer are:
- Chronic inflammatory diseases of the oral cavity;
- Hormonal imbalances;
- Genetic disorders;
- Smoking;
- Nutritional factors (low vitamin content, high fat content in food).
Most often the tissues of the parotid salivary gland are affected - 80%, less often the tumor develops in the tissues of the submandibular salivary gland - 15%, sublingual or minor salivary gland.
The following options for the development of pathology are distinguished:
- Primary cancer (from the tissues of the gland itself);
- Secondary cancer (metastasis or germination from neighboring organs).
According to histological parameters, tumors of the salivary glands represent the most heterogeneous group of human neoplasms. More than half of them are benign formations.
Benign neoplasms of the parotid salivary glands are detected in more than 30% of patients who complain, malignant ones - in 65%. Among the morphological types of benign tumors of the parotid salivary gland, the most commonly diagnosed are pleomorphic adenoma (a benign formation that forms in the glandular epithelium), adenolymphoma, lipoma and a very rare adenoid cystic tumor (formed by epithelial cells lining the lumen of the gland).
Malignant tumor formations are most often represented by: mucoepidermoid cancer (formed by cells secreting mucus and epithelium) and adenocarcinoma. Acinic cell carcinoma also occurs, which mainly affects the tissue of the parotid salivary gland.
Usually, during examination of patients, palpation reveals a dense, painless formation in the area of the salivary glands, which, according to patients, grows generally very slowly. In approximately a third of cases, pain may be present.
The “gold standard” for diagnosing tumors of the salivary glands is aspiration puncture of the tumor followed by histological examination of the obtained material, carried out before surgery or intraoperatively. The diagnostic value of this method is up to 90%, because the tissue of the affected area is studied directly under a microscope.
Aspiration puncture (biopsy) is performed using a special needle under ultrasound control. The study allows you to confirm or clarify the diagnosis, track the growth dynamics of the tumor and analyze the changes that occurred during tumor therapy.
During histological examination, three indicators are assessed:
- Tumor size and extent of its spread (T);
- The presence of damage to regional lymph nodes by metastases (N);
- Determination of metastases in other organs and tissues (M).
Based on the degree of malignancy, there are three types of tumors:
- High differentiation, when the cells are similar to glandular epithelial cells, such formations grow slowly and often have a favorable prognosis;
- Low differentiation, when cells are very different from normal, is characterized by rapid growth and early metastases;
- Medium differentiation.
Benefits of salivary gland sonography
This diagnostic method is recognized as fast, reliable, reliable, accessible and 100% safe. That is why it is so popular not only in Russia, but also abroad. Moreover, the study has virtually no contraindications. The presence of implants, foreign bodies in the body, or pacemakers in the patient does not in any way affect the procedure.
Among the advantages, one can also highlight the possibility of conducting an unlimited number of examinations, if necessary. Since the study does not cause discomfort or unpleasant sensations, it can be performed even on infants.
References
- Malignant tumors of the salivary glands, Clinical guidelines. Association of Oncologists of Russia, 2022. - 55 p.
- Balkanov, A.S., Bychenkova, O.A., Sipkin, A.M. and others. Combined treatment of parotid salivary gland cancer. Almanac of Clinical Medicine, 2022. - No. 4. - P. 309-313.
- Polyakov, V.G., Shishkov, R.V., Ermilova, V.D. and others. Children's Oncology, 2004. - No. 1. - P. 45-47.
- Carlson, E., Schlieve, T. Salivary Gland Malignancies. Oral and maxillofacial surgery clinics of North America, 2022. - Vol. 31(1). — P. 125-144.
Interpretation of ultrasound results of the salivary glands
Normally, the salivary glands have a clear contour, thanks to which they are clearly visible on ultrasound. The largest in size are the parotid glands. Their normal sizes reach 22-25 mm in thickness, 47-56 mm in length, 25-35 mm in width. For the sublingual glands, the normal length is 19-22 mm, thickness and width - 10-16 mm. The standard size of the submandibular glands: 24-30 mm in length, 14-18 mm in width.
The results of the sonographic examination are interpreted by a functional diagnostics specialist who performs the procedure. He compares the received data with reference parameters. Identification of individual pathologies or complex deviations based on the assessment of various diagnostic factors serves as the basis for writing a conclusion.
During an ultrasound, a specialist analyzes the size of the glands, their location, blood supply, and assesses the condition of the lymph nodes. In addition, the echogenicity indicator (the ability of organ tissue to transmit sound) is very important for the quality of sonography of the ear glands. Reference echogenicity values for each organ are different. This indicator cannot be neglected, because reduced echogenicity values when making a diagnosis may indicate the presence of an inflammatory process, swelling, and high values – a tumor.
If sonography of the salivary glands reveals neoplasms in a patient, he is referred for additional diagnostics. As a rule, the next procedure for such a patient is contrast magnetic resonance imaging of the soft tissues of the neck. In rare cases, histology, puncture, and biopsy are performed to accurately determine the nature of the formation. In any case, each of these diagnostic methods helps to determine whether the detected tumor is benign or malignant. Material is taken during puncture and biopsy using ultrasound.
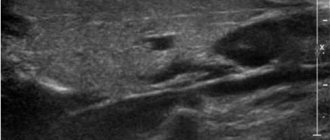
A 26-year-old woman came to our clinic. When collecting anamnesis, it was possible to find out that for 6 months she had periodic pain in the left cheek area, constant swelling of the soft tissues of the left parotid region and the lateral surface of the neck on the left side (Fig. 1). On initial examination, the patient's body temperature is normal, vital signs are stable, heart rate is 70 beats per minute, respiratory rate is 16 times per minute, blood pressure is 110/70 mmHg. Art. Laboratory tests revealed a slight increase in the number of white blood cells.
Before considering the possibility of an odontogenic origin of these symptoms, the patient consulted various specialists. Repeated cycles of antibiotic therapy prescribed by these specialists were ineffective. Subsequent sonographic examination revealed the presence of a small sialolith in the left parotid gland and a diagnosis of sialolithiasis was made. Over the course of one month, the patient underwent 3 cycles of external shock wave lithotripsy in the left parotid region. After the procedures, the symptoms persisted. A few weeks later, swelling of the soft tissues of the lateral surface of the neck transformed into acute purulent lymphadenitis of the corresponding localization. At this point, the patient was referred to the medical institution where the authors work.
An orthopantomogram revealed the presence of a semi-impacted third molar (wisdom tooth, tooth 38) (Fig. 2). Distal from tooth 38, the presence of a focus of bone tissue loss measuring 10 mm, formed as a result of an enlargement of the follicle of tooth 38, is determined.
Magnetic resonance imaging (MRI) revealed the presence of a subcutaneous abscess of the left parotid region, as well as the presence of lymphadenopathy on the left side (Fig. 3).
The decision was made to remove the left lower third molar and perform a cystectomy. Histopathological analysis of the excised cyst membrane revealed the presence of a dense inflammatory cellular infiltrate, consisting mainly of lymphocytes and plasma cells (Fig. 4). 30 minutes before surgery, the patient was administered the drug meropenem in an amount of 2 grams intravenously. After the operation, the symptoms completely disappeared, the patient was discharged from the clinic. She was prescribed amoxicillin/clavulanic acid 875 mg/125 mg orally every 12 hours for 7 days. During the last visit to the doctor, 6 months after the operation, no signs of scarring of the patient’s skin were found.
Rice. 1. Clinical appearance of an abscess in the parotid region. Purulent lymphadenitis of the lateral cervical lymph nodes, which appeared after external shock wave lithotripsy for the treatment of suspected sialolithiasis. Rice. 2. Orthopantomography revealed an anomaly in the eruption of tooth 38 and the presence of a follicular cyst. Rice. 3. Magnetic resonance imaging revealed the formation of a subcutaneous abscess in the left parotid-masticatory region. Rice. 4. Histological analysis of the area of the shell of the removed cyst revealed the presence of a dense inflammatory cellular infiltrate, consisting mainly of lymphocytes and plasma cells (hematoxylin and eosin staining).
Differential diagnosis
The list of clinical conditions in which unilateral parotid enlargement is observed includes sialolithiasis, tuberculosis, parotid actinomycosis, lymphadenitis, parotid cyst, sebaceous cyst and neoplasia.
Sialolithiasis
Salivary stone disease (sialolithiasis) is a disease that, in terms of frequency of damage to the major salivary glands, ranks second after mumps and is the cause of 30% of all sialoadenopathies. The highest incidence was found among men aged 30 to 60 years [1]. Sialolithiasis most often affects the submandibular salivary gland (83-94%), less often the parotid salivary gland (4-10%) and the sublingual salivary gland (1-7%) [2]. There are several hypotheses devoted to the etiology of the formation of stones in the salivary glands: a hypothesis about the role of anatomical and morphological factors (stenosis of the salivary duct, diverticulum of the salivary gland duct, etc.), about the influence of the composition of saliva (severe oversaturation, deficiency of crystallization inhibitors, etc.) and about the significance of inflammatory, chemical or neurogenic factors. The stones are composed of a mixture of calcium phosphates and, during the crystallization process, attract and accumulate an organic matrix.
Surgical removal of stones is an effective treatment method, but in some cases it contributes to the development of significant complications in the postoperative period. Currently, there are conservative treatment methods, such as extracorporeal lithotripsy, contact lithotripsy and percutaneous (percutaneous) lithotripsy [3].
Tuberculosis of the parotid salivary gland
Tuberculosis is an infectious granulomatosis with a chronic course, characterized by a variety of clinical manifestations and localization. Despite the fact that lung involvement is a typical symptom of this disease, extrapulmonary forms of the disease are common and account for 20% of all cases of active tuberculosis [4]. Infection of the salivary glands is rare. Damage to the parotid salivary gland and nearby lymph nodes can occur in the presence of a focus of tuberculosis infection in the oral cavity or in the presence of a distant focus in the lung [5]. In this case, the disease is accompanied by acute inflammation and diffuse swelling of the salivary gland. In some cases, the formation of a parotid fistula or abscess occurs [6].
Actinomycosis of the parotid gland
The primary focus of actinomycosis is a granuloma and is characterized by chronic suppuration. The usual cause is Actinomyces israelii, a Gram-positive anaerobic opportunistic oral bacteria. Actinomycosis affects healthy people, in the presence of local conditions conducive to the growth of the pathogen. Often the disease affects soft tissues, salivary glands, bones and skin in the face and neck. Primary actinomycosis of the parotid salivary gland is a very rare disease, the external manifestations of which may be similar to signs of the presence of a neoplasm [7].
The clinical sign of cervicofacial actinomycosis is the presence of a purulent formation and typical yellow-green purulent discharge containing small yellow granules, which have diagnostic value. Initial symptoms include pain, fever, redness of the skin, and swelling of soft tissues. Suppuration may be absent [8].
Other conditions causing unilateral enlargement of the parotid region
Unilateral enlargement of the parotid region may be a consequence of the presence of a palpable mass or diffuse edema. Localization of the formation on the surface of the salivary gland may indicate the presence of lymphadenitis, a parotid salivary gland cyst, a sebaceous gland cyst, or a tumor of an extraparotid location. A formation located deep within the salivary gland may be a benign or malignant tumor or sialoadenopathy.
Clinical symptoms of malignant tumors include rapid growth, facial paralysis, tissue hardening, and pain. Most often, such neoplasms occur in older people [9].
Diffuse swelling of the parotid region, not associated with a pathological process in the parotid salivary gland, may be a sign of hypertrophy of the masticatory muscle, damage to the temporomandibular joint, or osteomyelitis of the ascending branch of the mandible.
Rationale for diagnosis
In the case of unilateral enlargement of the parotid region, when carrying out differential diagnosis, it is necessary to take into account the history of the current disease and the location of the palpable formation or diffuse edema. Sialadenitis can occur in the absence of any formation in the salivary gland. In this case, the presence of diffuse edema is accompanied by sharp pain in the area of the salivary gland, which disappears after 15-20 minutes. Painful swelling may occur after radiation therapy or result from a viral inflammation of the salivary gland, such as mumps. In these cases, a conventional orthopantomogram can be used for a comprehensive assessment of the pathology of the dentition and surrounding bone structures, temporomandibular joints, maxillary sinuses and nasal cavity. In order to determine the volume of inflamed tissue and the amount of accumulated pus, if the spread of infection affects the masticatory muscles or fascia, computed tomography and magnetic resonance imaging are used.
The patient was diagnosed with a rare follicular cyst. The presence of a cyst was accompanied by an inflammatory process that tended to further spread to surrounding tissues. Disruption of the eruption process usually carries the risk of damage to the dental follicle and the formation of a follicular cyst.
The authors suggested the spread of infection along an ascending path, from the follicular cyst and further, between the inner surface of the left branch of the mandible and the internal pterygoid muscle. The infection spread along this path and reached the mandibular notch, forming a subcutaneous abscess in the left parotid region. The virulence of microorganisms and the action of masticatory forces may explain the spread of the abscess in defiance of gravitational forces. Moreover, previously performed external shock wave lithotripsy could contribute to the spread of infection and intensify the process of suppuration.
Third molar extraction is a routine surgical procedure and the oral and maxillofacial surgeon must be aware of the possible complications. Odontogenic infections can spread through various cellular spaces of the maxillofacial region formed by muscles and fascia, causing serious complications such as brain abscess, cavernous sinus thrombosis, inflammatory processes in the temporal region, mediastinitis and severe inflammatory processes in the deep lateral space of the neck [10] . Fortunately, in the case we are considering, the inflammatory process did not spread to the peripharyngeal space, which could lead to obstruction of the airway and the development of a life-threatening condition.
This article describes a rare case of inflammation of the subcutaneous tissue and purulent lymphadenopathy, which developed as a result of the presence of a follicular cyst of the lower jaw, accompanied by the formation of a subcutaneous abscess in the parotid region. The threat of developing severe complications, such as sepsis or involvement of the peripharyngeal tissue space in the pathological process, combined with the rapid spread of infection, is an indication for emergency measures necessary to make a correct diagnosis and begin treatment.
Literature
- Grases F, Santiago C, Simonet BM, Costa-Bauzá A. Sialolithiasis: mechanism of calculi formation and etiologic factors.
Clin Chim Acta. 2003; 334(1-2): 131-6. - Lustmann J, Regev E, Melamed Y. Sialolithiasis. A survey on 245 patients and a review of the literature.
Int J Oral Maxillofac Surg. 1990; 19(3): 135–8. - Capaccio P, Torretta S, Ottavian F, Sambataro G, Pignataro L. Modern management of obstructive salivary diseases.
Acta Otorhinolaryngol Ital. 2007; 27(4): 161–72. - Lee IK, Liu JW. Tuberculous parotitis: case report and literature review.
Ann Otol Rhinol Laryngol. 2005; 114(7): 547–51. - Hamdan AL, Hadi U, Shabb N. Tuberculous parotitis: a forgotten entity.
Otolaryngol Head Neck Surg. 2002; 126(5): 581–2. - Sethi A, Sareen D, Sabherwal A, Malhotra V. Primary parotid tuberculosis: varied clinical presentations.
Oral Dis. 2006; 12(2): 213–5. - Ermis I, Topalan M, Aydin A, Erer M. Actinomycosis of the frontal and parotid regions.
Ann Plast Surg. 2001; 46(1): 55–8. - Mullins JE Jr, Ogle O, Cottrell DA. Painless mass in the parotid region.
J Oral Maxillofac Surg. 2000; 58(3): 316–9. - Musani MA, Sohail Z, Zafar S, Malik S. Morphological pattern of parotid gland tumors.
J Coll Physicians Surg Pak. 2008; 18(5): 274–7. - Kinzer S, Pfeiffer J, Becker S, Ridder GJ. Severe deep neck space infections and mediastinitis of odontogenic origin: clinical relevance and implications for diagnosis and treatment.
Acta Otolaryngol. 2009; 129(1): 62–70.
Stages of the disease
Salivary gland cancer, like other malignant tumors, is classified into stages according to the generally accepted TNM system. The letter T in the abbreviation denotes the characteristics of the primary tumor: the size and degree of its growth into surrounding tissues, N - spread to the lymph nodes, M - the presence of distant metastases. Depending on these indicators, the following stages are distinguished during salivary gland cancer:
- Stage 0 is “cancer in situ” (carcinoma in situ). The tumor is located within the layer of cells that form the salivary gland and does not grow into neighboring tissues.
- Stage I is a tumor that is located within the salivary gland and measures no more than 2 cm.
- Stage II - the tumor reaches a size of more than 2 cm, but not more than 4 cm.
- Stage III - a tumor that reaches a size of more than 4 cm and/or spreads into surrounding tissues, or a tumor of any size that has grown into surrounding tissues, has spread to one cervical lymph node on the same side, and the focus in the lymph node is no more than 3 cm and does not extend beyond its borders.
- Stage IV includes substages IVA, IVB or IVC. The first two are characterized by varying degrees of spread of the malignant tumor to the anatomical structures of the head, neck, and lymph nodes. If stage IVC is diagnosed, it means that there are distant metastases.
In addition to stages, there are three degrees of malignancy of salivary gland cancer:
- Grade I - low degree of malignancy. Such tumors are called highly differentiated. Tumor tissue is as similar as possible to normal salivary gland tissue. It grows slowly, and the prognosis for such patients is most favorable.
- Grade II are moderately differentiated tumors. Tumor tissue differs more significantly from normal tissue. This cancer is more aggressive and has a poorer prognosis.
- III degree - poorly differentiated tumors. Cancer cells almost completely lose the features of normal ones. Such tumors behave the most aggressively.
Determining the degree of malignancy helps the doctor predict how the cancer will behave and plan treatment correctly.
Symptoms of the disease
Benign and malignant tumors of the salivary glands present with similar symptoms. One of the main differences is that cancer grows much faster and more often leads to a number of symptoms associated with growth into surrounding tissues and compression of nerves.
You need to visit a doctor if you are bothered by the following symptoms:
- A lump or swelling has appeared in the mouth, cheek, jaw, or neck.
- You have noticed that your face has become asymmetrical.
- I am worried about pain in the mouth, neck, ear, cheek, jaw. It doesn't last long.
- Numbness of part of the face.
- Weakness in the facial muscles, because of this, half of the face may be “lowered,” which becomes especially noticeable when baring teeth or frowning.
- I can't open my mouth wide.
- Difficulty swallowing.