Detailed description of the study
Salivary gland cancer is a malignant tumor of the salivary gland formed from epithelial cells. Tumors of the parotid salivary glands (PST) are a rare type of neoplasm. They mainly develop between the ages of 20 and 40. More common in men than in women. Tumors are usually located in the soft tissues of the face and often cause serious cosmetic defects, causing paresis of the facial nerve.
The main risk factors for developing salivary gland cancer are:
- Chronic inflammatory diseases of the oral cavity;
- Hormonal imbalances;
- Genetic disorders;
- Smoking;
- Nutritional factors (low vitamin content, high fat content in food).
Most often the tissues of the parotid salivary gland are affected - 80%, less often the tumor develops in the tissues of the submandibular salivary gland - 15%, sublingual or minor salivary gland.
The following options for the development of pathology are distinguished:
- Primary cancer (from the tissues of the gland itself);
- Secondary cancer (metastasis or germination from neighboring organs).
According to histological parameters, tumors of the salivary glands represent the most heterogeneous group of human neoplasms. More than half of them are benign formations.
Benign neoplasms of the parotid salivary glands are detected in more than 30% of patients who complain, malignant ones - in 65%. Among the morphological types of benign tumors of the parotid salivary gland, the most commonly diagnosed are pleomorphic adenoma (a benign formation that forms in the glandular epithelium), adenolymphoma, lipoma and a very rare adenoid cystic tumor (formed by epithelial cells lining the lumen of the gland).
Malignant tumor formations are most often represented by: mucoepidermoid cancer (formed by cells secreting mucus and epithelium) and adenocarcinoma. Acinic cell carcinoma also occurs, which mainly affects the tissue of the parotid salivary gland.
Usually, during examination of patients, palpation reveals a dense, painless formation in the area of the salivary glands, which, according to patients, grows generally very slowly. In approximately a third of cases, pain may be present.
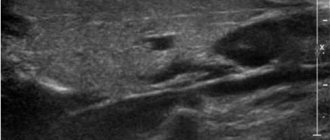
The “gold standard” for diagnosing tumors of the salivary glands is aspiration puncture of the tumor followed by histological examination of the obtained material, carried out before surgery or intraoperatively. The diagnostic value of this method is up to 90%, because the tissue of the affected area is studied directly under a microscope.
Aspiration puncture (biopsy) is performed using a special needle under ultrasound control. The study allows you to confirm or clarify the diagnosis, track the growth dynamics of the tumor and analyze the changes that occurred during tumor therapy.
During histological examination, three indicators are assessed:
- Tumor size and extent of its spread (T);
- The presence of damage to regional lymph nodes by metastases (N);
- Determination of metastases in other organs and tissues (M).
Based on the degree of malignancy, there are three types of tumors:
- High differentiation, when the cells are similar to glandular epithelial cells, such formations grow slowly and often have a favorable prognosis;
- Low differentiation, when cells are very different from normal, is characterized by rapid growth and early metastases;
- Medium differentiation.
Salivary glands
Salivary glands
(lat. gladulae salivales) - exocrine glands that secrete secretions into the oral cavity, called saliva. There are minor and major salivary glands.
Minor salivary glands
The minor salivary glands are located in the oral mucosa and are classified by their location (labial, buccal, molar, lingual and palatal) or by the nature of the secretion (serous, mucous and mixed).
The most numerous of the minor salivary glands are the labial and palatine glands. Serous glands are found mainly among lingual glands; the saliva they secrete is rich in protein. The mucous glands are the palatine and part of the lingual; the saliva they produce is rich in mucus. Mixed - buccal, molar, labial and part of the lingual secrete saliva of mixed composition. The minor salivary glands are located deep in the oral mucosa or in its submucosa. The sizes of small glands are varied, their diameter ranges from 1 to 5 mm.
Major salivary glands
The major salivary glands are three pairs of salivary glands distinguished by their size.
The largest of them are the parotid salivary glands, located below and in front of the auricle directly under the skin.
The excretory duct of the parotid gland (stenon duct) opens on the side wall of the vestibule of the oral cavity at the level of the second upper molar. Medium-sized - submandibular salivary glands. An excretory duct departs from the gland - Wharton's duct, which is located at the bottom of the oral cavity and opens with a small hole at the top of the paired papilla, located near the frenulum of the tongue. The submandibular glands, like the parotid glands, secrete a mixed type of saliva.
The smallest of the major salivary glands are the sublingual glands, located under the mucous membrane of the floor of the mouth, on both sides of the tongue. They produce saliva with a predominance of the mucous component. From each of the sublingual glands, a Bartholin duct emerges, opening either separately on the sublingual papilla, or through one common opening with the Wharton duct. In addition, a number of small ducts depart from the sublingual glands, most of which open on the sublingual fold.
Figure used under CCA3.0 license, taken from “Medical gallery of Blausen Medical 2014”. WikiJournal of Medicine 1 (2). DOI:10.15347/wjm/2014.010. ISSN 2002-4436. Adapted.
Salivary glands in children and adults
The secretion of saliva begins in children immediately after birth. A newborn secretes 0.6–6 ml of saliva per hour, with active sucking - up to 24 ml per hour. Starting from the age of 3 – 6 months, the child’s salivation increases significantly. The weight of the salivary glands also increases (Paikov V.L.):
| Age | Average weight of major salivary glands, g | ||
| parotid | submandibular | sublingual | |
| newborns | 0,9–2,4 | 0,84 | 0,42 |
| 3 months | 1,4–4,8 | 1,54 | 0,84 |
| 6 months | 4,5 (3,1–5,8) | 2,12 | 1,05 |
| 2 years | 8,6 (8,2–9,6) | 4,89 | 2,00 |
| men | 36,6 (26–96) | 13,23 | 5,05 |
| women | 28,8 (22–48) | 9,70 | 4,68 |
Salivary glands in newborns
Features of the salivary glands of a newborn:
- low secretory activity
- secretion of a small amount of thick, viscous saliva (sealing the oral cavity during sucking)
- saliva reaction is neutral or slightly acidic
- amylase concentration is low.
The functional activity of the salivary glands increases at 1.5–2 months; In children aged 3–4 months, saliva often leaks from the mouth. This is due to the immaturity of the regulation of salivation and swallowing of saliva (physiological salivation). The acidity of saliva increases with age. From the first days of life, saliva contains a-amylase and other enzymes necessary for the breakdown of starch and glycogen. In newborns, during the first year of life the content and activity of these enzymes increase significantly (Geppe N.A., Podchernyaeva N.S., 2008).
Diseases of the salivary glands in ICD-10
In the International Classification of Diseases ICD-10, diseases of the salivary glands are classified as “Class XI. Diseases of the digestive system." A separate section “K11 Diseases of the salivary glands” includes the following diseases:
- K11.0 Salivary gland atrophy
- K11.1 Salivary gland hypertrophy
- K11.2 Sialadenitis
- K11.3 Salivary gland abscess
- K11.4 Salivary gland fistula
- K11.5 Sialolithiasis
- K11.6 Salivary gland mucocele
- K11.7 Disorders of salivary gland secretion
- K11.8 Benign lymphoepithelial lesion of the salivary gland
- K11.8 Mikulicz disease
- K11.8 Necrotizing sialometaplasia
- K11.8 Sialectasia stenosis of the salivary duct
- K11.8 Constriction of the salivary duct
Congenital anomalies of the salivary glands and ducts (salivary gland(s) or duct: absence, accessory, atresia; congenital fistula of the salivary gland) belong to “Class XVII. Congenital anomalies [malformations], deformations and chromosomal disorders”, to the heading “Q38.4 Congenital anomalies of the salivary glands and ducts”.
Frame “Methods of functional diagnostics of salivary gland secretion” from a video for medical university students: Khamchiev K.M. (Dr. Kureysh). Video lesson on physiology: Research methods and regulation of digestion. Food center
On the GastroScan.ru website in the “Literature” section there is a subsection “Oral diseases associated with gastrointestinal diseases”, containing publications for healthcare professionals on this topic.
Patient Materials
The GastroScan.ru website also contains materials for patients on various aspects of gastroenterology:
- “Advice from doctors” in the “Patients” section of the site
- “Popular gastroenterology” in the “Literature” section
- “Popular gastroenterology” in the “Video” section
Back to section
References
- Malignant tumors of the salivary glands, Clinical guidelines. Association of Oncologists of Russia, 2022. - 55 p.
- Balkanov, A.S., Bychenkova, O.A., Sipkin, A.M. and others. Combined treatment of parotid salivary gland cancer. Almanac of Clinical Medicine, 2022. - No. 4. - P. 309-313.
- Polyakov, V.G., Shishkov, R.V., Ermilova, V.D. and others. Children's Oncology, 2004. - No. 1. - P. 45-47.
- Carlson, E., Schlieve, T. Salivary Gland Malignancies. Oral and maxillofacial surgery clinics of North America, 2022. - Vol. 31(1). — P. 125-144.
Course of lectures (almost all) / Lecture 21 Salivary glands
3
Lecture 21: Salivary glands.
The surface of the oral epithelium is constantly moistened by the secretion of the salivary glands (SG). There are a large number of salivary glands. There are small and large salivary glands. Small salivary glands are present in the lips, gums, cheeks, hard and soft palates, and in the thickness of the tongue. The large salivary glands include the parotid, submandibular and sublingual glands. Small SGs lie in the mucosa or submucosa, and large SGs lie outside these membranes. All SMs in the embryonic period develop from the epithelium of the oral cavity and mesenchyme. SG is characterized by an intracellular type of regeneration.
Functions of the SJ:
- Exocrine function is the secretion of saliva, which is necessary for:
- facilitates articulation;
- formation of a food bolus and its swallowing;
- cleaning the oral cavity from food debris;
- protection against microorganisms (lysozyme);
- Endocrine function:
- production in small quantities of insulin, parotin, growth factors of epithelium and nerves, and a lethality factor.
- Beginning of enzymatic food processing (amylase, maltase, pepsinogen, nucleases).
- Excretory function (uric acid, creatinine, iodine).
- Participation in water-salt metabolism (1.0-1.5 l/day).
Let's take a closer look at large SGs. All large SGs develop from the epithelium of the oral cavity; they are all complex in structure (the excretory duct is highly branched. In large SGs, a terminal (secretory) section and excretory ducts are distinguished.
The parotid gland is a complex alveolar protein gland. The terminal sections of the alveoli are proteinaceous in nature and consist of serocytes (protein cells). Serocytes are conical cells with basophilic cytoplasm. The apical part contains acidophilic secretory granules. Granular EPS, PC and mitochondria are well expressed in the cytoplasm. In the alveoli, myoepithelial cells are located outward from the serocytes (as if in a second layer). Myoepithelial cells have a stellate or branched shape, their processes encircle the terminal secretory section, and they contain contractile proteins in the cytoplasm. During contraction, myoepithelial cells promote the movement of secretions from the terminal section into the excretory ducts. The excretory ducts begin with intercalary ducts - they are lined with low cubic epithelial cells with basophilic cytoplasm, and are surrounded by myoepithelial cells from the outside. The intercalary ducts continue into the striated sections. The striated sections are lined with single-layer prismatic epithelium with basal striations, caused by the presence of cytolemma folds in the basal part of the cells and mitochondria lying in these folds. On the apical surface, epithelial cells have microvilli. The striated sections on the outside are also covered by myoepitheliocytes. In the striated sections, reabsorption of water from saliva (thickening of saliva) and balancing of the salt composition occurs, in addition, an endocrine function is attributed to this section. The striated sections, merging, continue into interlobular ducts, lined with 2-row epithelium, turning into 2-layer. The interlobular ducts flow into the common excretory duct, lined with stratified squamous non-keratinizing epithelium. The parotid SG is externally covered with a connective tissue capsule, interlobular septa are well defined, i.e. a clear lobulation of the organ is noted. In contrast to the submandibular and sublingual SG, in the parotid SG, inside the lobules the layers of loose fibrous SDT are poorly expressed.
The submandibular fluid is complex alveolar-tubular in structure, mixed in the nature of the secretion, i.e. mucous-protein (with a predominance of the protein component) gland. Most of the secretory sections are alveolar in structure, and the nature of the secretion is proteinaceous - the structure of these secretory sections is similar to the structure of the terminal sections of the parotid gland (see above). A smaller number of secretory sections are mixed - alveolar-tubular in structure, mucous-protein in the nature of the secretion. In the mixed terminal sections, large light mucocytes (poorly accepting dyes) are located in the center. They are surrounded in the form of crescents by smaller basophilic serocytes (protein crescents of Juanizi). The terminal sections are surrounded on the outside by myoepitheliocytes. In the submandibular gland from the excretory ducts, the intercalary ducts are short, poorly defined, and the remaining sections have a similar structure to the parotid gland.
The stroma is represented by a capsule and SDT-tissue partitions extending from it and layers of loose fibrous SDT. Compared to the parotid SG, the interlobular septa are less pronounced (weakly expressed lobulation). But inside the lobules the layers of loose fibrous SDT are better expressed.
The sublingual gland is a complex alveolar-tubular gland in structure; the nature of the secretion is mixed (muco-protein) gland with a predominance of the mucous component in the secretion. In the sublingual gland there are a small number of purely proteinaceous alveolar end sections (see description in the parotid gland), a significant number of mixed mucous-protein end sections (see description in the submandibular gland) and purely mucous secretory sections shaped like a tube and consisting of mucocytes with myoepitheliocytes. Among the features of the excretory ducts of the sublingual SG, the weak expression of the intercalary ducts and striated sections should be noted.
The sublingual SG, like the submandibular SG, is characterized by weakly expressed lobulation and well-defined layers of loose fibrous SDT inside the lobules.