The upper and lower jaw system has a very complex anatomical structure. The bone structure is characterized by a high dependence on effective blood supply and necessary nutrition for full growth and development. The full functioning of the skeletal system is directly related to the presence of all elements of the dentition. Due to the removal or long-term absence of molars, various pathological processes of the alveolar process of the upper and lower jaw develop.
In accordance with the anatomical features and existing pathologies, correction or augmentation is carried out, bone tissue is built up for successful prosthetics. Appropriate periodontal treatment makes it possible to securely fix the implant in the oral cavity without the risk of possible complications. Augmentation is often done using bone-replacing biomaterials of artificial or natural origin. An integrated approach to diagnosing pathology and a highly effective treatment method allows you to achieve the desired result.
What is the alveolar process?
Bone tissue, consisting of the basal layer, spongy tissue and cortical plate, plays an important role in reliable fixation of the dentofacial system. As a result of everyday physical activity, it undergoes morphological and histological changes. The alveolar process (AO) to the anatomical part that holds the elements of the dentition of the upper and lower jaw. It is formed from the moment the teeth erupt and atrophies after their loss.
The process consists of inner and outer cortical plates and cancellous bone tissue. It is permeated with small tubules through which blood vessels and nerves pass. The anatomical structure of the ridge has an unpaired symmetrical structure; the holes may differ in shape and size depending on the placement of the dental units. Alveoli are located in the center of the alveolar ridge; most often they have a cone-shaped shape. As a result of pathology or loss of elements of the dentition, a significant decrease in the volume of bone tissue occurs, which will require restoration of the alveolar process for subsequent implantation.
Treatment
The treatment method is selected depending on the established severity of the fracture. Before any manipulation, the doctor performs anesthesia. Torn tissues are treated with antiseptics to prevent infection. Then reconstruction is carried out (if there are fragments) and fixation of the jaw.
If there is displacement, the doctor opens the gums in the area of the fracture (revision) to eliminate the sharp edges of the fragments, after which he manually puts the displaced part in place. This must be done in such a way that it corresponds to the correct bite. After this, the gum is sutured and an iodoform dressing is applied to the wound.
To fix the alveolar process, a smooth splint-bracket is used, which is attached to three healthy teeth on both sides of the chipped part. If this is not possible, that is, if the teeth on one side are not stable or are completely absent, then I use five additional teeth for fixation. For greater immobilization of the dentition, wearing a chin sling may be indicated.
If the injury occurs in the anterior part of the upper molars, then fixation occurs through the installation of a single-jaw bracket, which is fixed on the damaged area (attached with ligatures to healthy teeth).
In case of complete absence of teeth, a splint made of quickly hardening plastic is installed.
After all surgical procedures, the patient is prescribed antibacterial therapy and medications to accelerate healing and prevent the development of inflammation in the injured area.
Structure of the alveolar ridge
Taking into account the anatomical structure, the following parts are distinguished:
- Lateral. The outer wall located in close proximity to the cheeks and lips.
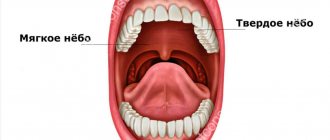
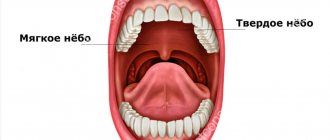
- Medial. The inner wall, which is directed towards the tongue and hard palate, has a compacted structure.
- Central. The location of the tooth sockets, the area has a large number of blood channels. This is where the molars and incisors are attached.
The alveoli and dental sockets are separated from each other by special bone partitions. In the alveolar part there are also interradicular septa. In the absence of functional loads on the ridge area, deformation of the alveolar process, changes in the anatomical structure and its reduction begin to be observed. The development of pathological processes in the upper and lower jaw often leads to a fracture of the alveolar process, which may require correction of this anatomical part.
Functions of the alveolar process of the upper and lower jaw
- Fixation and maintenance of elements of the dental system.
- Active participation in chewing food.
- Makes it easier to bite into hard foods.
The state of AO is reflected in a person’s external data. The development of pathologies often leads not only to a deterioration in the performance of molars and incisors, but also affects the anatomy of the facial skeleton. Over the years, the oxygen supply to bone tissue is disrupted, which leads to various defects of the alveolar process. As a result, this can cause loss of teeth, the development of traumatic injuries, periodontal disease, periodontitis and other dental problems.
Composition
[4]
Inorganic matrix
Alveolar bone consists of 67% inorganic material. The inorganic material consists mainly of calcium and phosphate minerals. Minerals are mainly represented by crystals of calcium hydroxyapatite.
Organic matrix
The remaining alveolar bone is organic material (33%). Organic material consists of collagen and non-collagenous material. The cellular component of bone consists of osteoblasts, osteocytes and osteoclasts.
- Osteoblasts are usually cuboidal and slightly elongated. They synthesize both collagenous and non-collagenous bone proteins. These cells have high levels of alkaline phosphatase on the outer surface of their plasma membrane. The functions of osteoblasts are bone formation by synthesizing organic bone matrix, intercellular communication, and maintenance of bone matrix.
- Osteocytes are modified osteoblasts that become trapped in lacunae during bone matrix secretion. Osteocytes have extensions called tubules that arise from the lacunae. These tubules deliver oxygen and nutrients to the osteocytes through the blood and remove waste products.
- Osteoclasts are multinucleated giant cells. They are located in the gaps of Howship.
Signs of pathologies of the alveolar ridge
- Predominant swelling of the mucous membrane in the area of the alveolar ridge.
- Pain when chewing food, swallowing saliva.
- Damage to gum tissue, bleeding.
- The appearance of multiple abrasions.
- Sharp expansion of interdental areas due to loss of incisors.
- Development of pathology of occlusion of elements of the dental system.
- The appearance of various speech defects, which can be expressed in a “lisp.”
In addition, hypertrophy of the alveolar process may develop, which is expressed in an increase in the volume of bone tissue due to histological changes. An external examination and x-ray may reveal a crack in the ridge or a complete separation of bone tissue from the fundamental cranial bone.
Sinus lifting – briefly about the method
When implanting in the lateral areas of the upper jaw, in the vast majority of cases, raising the level of bone tissue is required. The upper jaw is an air-bearing organ. It contains the maxillary sinuses, lined with ciliated epithelium, which is responsible for purifying the air we inhale. The sinus lift operation involves carefully lifting the mucous membrane with curettes and performing bone grafting. In fact, a sinus lift is a version of the GBR for the upper jaw in the projection of the maxillary sinuses. The success of bone grafting for alveolar process atrophy depends on the patient's compliance with doctors' recommendations, strict adherence to the postoperative regimen, non-smoking, and of course, on the experience and qualifications of the operating surgeon!
Causes of alveolar process atrophy
- Injuries, mechanical damage to the area.
- Morphological changes associated with significant disruption of blood circulation.
- Formation of uneven edges of the alveoli after the removal of dental units.
- Osteomyelitis of the alveolar process, inflammatory processes of bone tissue.
- Neoplasms, cysts that lead to ridge degeneration.
- Loss of elements of the dental system.
Other causes of the development of pathological processes may include chronic inflammatory processes, fibrous osteitis, which is expressed in the thinning of the bone structure, or tumors of the alveolar process. Pathology may also be associated with hereditary factors and genetic predisposition. In all these cases, correction and immediate intervention by a dental surgeon are required, since the tissue itself does not recover.
Diagnosis of diseases of the alveolar process
In order to correctly select a therapeutic or surgical treatment method, an appropriate set of diagnostic procedures is carried out: blood tests, radiography. Additionally, MRI, CT of the upper jaw, and biochemistry may be prescribed. The last analysis is prescribed if there is a suspicion of metabolic disorders in the body. Densitometry and orthopantomogram are also prescribed as diagnostic procedures. Comprehensive diagnostics allows you to build the correct correction tactics.
Treatment and restoration of the alveolar process
- Split-Control technology. The main purpose of this procedure is to expand the jaw bone to allow subsequent implantation. The procedure is performed as follows. The specialist saws the comb, places biomaterial, a bone tissue substitute, into the cavity, and applies sutures.
- Intercortical osteomia. It involves splitting the alveolar process to correct the bone structure. During the surgical intervention, the ridge is cut to form a movable fragment, which the dental surgeon then moves to another part where there is a lack of bone tissue. The moving part is fixed with special screws, and the cavity is filled with biomaterial.
The rehabilitation time after surgery and resection of the alveolar process can be several months. After this, you can begin to implant the implant. In each case, you must consult directly with your dentist. He will track the dynamics and determine the condition of the alveolar process in which there was a cleft or damage.
Despite the development of dentistry, new methods of treating teeth and periodontal diseases, the number of patients in need of dental prosthetics after tooth loss is growing.
Surgical sanitation of the oral cavity after therapeutic treatment of teeth and diseases of the oral mucosa is an important part of preparation for prosthetics.
Various clinical situations interfere with dental implantation:
- the presence of non-supportable destroyed teeth and their roots;
- the presence of pathologically altered tissues with signs of an inflammatory process;
- defects and atrophy of the alveolar processes of the jaws;
- small vestibule of the oral cavity;
- short frenulum of the tongue and cheeks;
- dystopia of supporting teeth.
All of the above interferes with the production of dentures and therefore must be corrected.
Surgical preparation of the oral cavity for dental prosthetics involves careful planning and implementation of the following general and local activities:
- General therapeutic measures: examination of the patient, identification of somatic contraindications to the selected type of prosthetics, treatment of common diseases to achieve a compensated condition for the patient.
- Local therapeutic measures: removal of decayed teeth and their roots, periapical granulomas, tumors, jaw cysts, impacted teeth, preparation of the jaws and their alveolar processes.
Preparation of the oral mucosa for prosthetics
All local therapeutic measures are divided into three main categories:
- traditional therapeutic measures for the purpose of sanitation of the oral cavity, which must be carried out taking into account subsequent dental prosthetics;
- plastic surgery of the soft tissues of the oral cavity before using a specific prosthesis;
- plastic surgery of bone structures before prosthetics with a specific type of prosthesis;
- Installation of supports for dentures - this is not necessary in the case of removable plate dentures.
Traditional therapeutic sanitizing measures
These measures include surgical interventions for the purpose of general improvement of the patient. They are designed to provide the form and functionality of the alveolar bone and mucous membrane necessary for prosthetics.
Local prevention of alveolar bone atrophy after tooth extraction:
- when removing teeth and roots, it is necessary to minimally injure adjacent tissues and bone; carry out periodontotomy deeper, and loosen the tooth carefully, do not break the walls of the fossa, immediately compare them and form a rational shape of the alveolar process;
- rationally fill the hole with osteogenic tissues and materials;
- prevent the development of inflammatory and other complications;
- prevent the occurrence of a “dry socket” by filling with the patient’s blood;
- cover the hole with a flap of the mucous membrane.
Shortened frenulums of the lips, cheeks and tongue must be corrected surgically, by dissection or plastic surgery with triangular flaps of the mucous membrane.
Sharp edges of the sockets and interradicular septa of previously extracted teeth, exostoses of the alveolar process and jaws, sharp edges and deformations of the walls of the fossae should be corrected by open alveolectomy and closed transmucosal alveolar compression.
Plastic surgery of soft tissues of the oral cavity
In accordance with the known clinical variations in the structure of the mucous membrane, treatment may include a large number of possible surgical interventions to prepare the mucous membrane for dental prosthetics:
- excision of cicatricial adhesions of the mucous membrane using triangular flaps of the mucous membrane to close the resulting defect;
- deepening the small vestibule of the mouth before using a removable lamellar prosthesis, clasp and bridge prosthesis in an aesthetically significant area;
- the movement of mucomuscular flaps is often performed from the lingual surface of the anterior part of the lower jaw, when the muscles of the floor of the mouth with the mucous membrane are moved down;
- removal of excess mucous membrane of the oral cavity with local hyperplasia, fibromatosis of the alveolar process, tubercle of the upper jaw, fibropapilloma and papillomatosis, which can occur as a result of prolonged injury to the mucous membrane by the edges of removable dentures;
- with a mobile mucous membrane on the crest of the alveolar process, various types of operations are performed: moving the mucous membrane down and suturing it in the lower pole of the wound, moving it to the exposed bone with closure with an iodoform tampon (according to Wassmund), moving the oral mucosa on the lower jaw down simultaneously with the lingual and labial side (according to Rerman).
- Myoplasty of the muscles adjacent to the lower jaw involves moving the m.mentalis, m.genioglossus and m.milohioideus to a new position, significantly deepening the vestibule of the oral cavity and the level of tissues.
After plastic surgery, plastic aligners are needed for the area of reconstruction of the mucous membrane, alveolar processes, and vestibule of the oral cavity.
Plastic surgery of jaw bone tissue
There are different forms of the crest of the alveolar process of the jaw, which are more or less favorable for the manufacture of removable dentures. The most favorable is considered to be trapezoidal, semi-oval, semi-circular shape.
In turn, the triangular shape with a sharp or jagged apex, the pineal and awl-shaped shape are less favorable for treatment and may require osteoplastic surgical correction.
In the toothless areas of the jaws, defects of the alveolar process are noted, which, in accordance with the planned type of prosthesis, require elimination. Highlight:
- Class I: buco-lingual bone loss with normal alveolar height;
- Class II: loss of alveolar process height with normal buco-lingual width;
- Class III: combined loss of height and width of the alveolar process.
Osteoplasty
performed in the presence of bone exostoses, osteomas, an unfavorable shape of the alveolar process for prosthetics, an enlarged torus of the palate or torus of the lower jaw, an enlarged tubercle of the upper jaw. Some of these formations are unilateral, bilateral, or median.
Removal of small exostoses is often performed on an outpatient basis under local anesthesia. The operations are typical - incision, exposure and removal of the formation, followed by suturing of the wound.
Movement of the neurovascular bundle
is performed if it is located under the mucous membrane and can be injured by the base of the prosthesis - a bone bed is created for the beam.
Alveoloplasty
provides for the restoration of the volume of the alveolar process of the jaws, the tubercle of the upper jaw before removable prosthetics is performed using various bone materials and methods. Autologous bone, xenogeneic bone material, hydroskiapatite, and demineralized bone graft are widely used.
Preparatory operations
Before the introduction of dental implants for fixation of prostheses, it is usually necessary to increase the height and width of the alveolar process of the jaws and improve the quality of the existing bone.
Introduction of a dental implant into tissue
performed in various ways, depending on the design of the implant, quantity and specific installation location.
Reconstruction of the supporting bone of the alveolar process
In the 1960s, Brånemark (Sweden) demonstrated that a titanium implant could be firmly in contact with the bone surface through osseointegration. Since then, considerable attention has been paid to the condition of the supporting bone.
Signs of osseointegration are the immobility of the implant, tight contact with the bone without signs of inflammation, the absence of a liquefaction zone between the bone and the implant on radiographs, and the normal state of adjacent tissues.
To increase the height of the alveolar processes of the jaws, perform:
- local osteoplastic operations: planar osteotomy of the alveolar process or body of the lower jaw, open and closed osteotomies, the use of mucoperiosteal bone flaps;
- free autologous bone transplantation (intraoral or extraoral grafts);
- guided tissue regeneration using separation membranes, metal frames and materials for filling bone defects;
- vertical distraction of the alveolar process is performed with special distraction devices, distraction implants and traction - distraction from the socket of the tooth root to be removed.
An increase in the thickness of the alveolar process of the jaws is achieved by:
- dissection and splitting of the alveolar process with chisels, installation of grafts or immediately implants with bone material in the split bone;
- transplantation of a free autologous graft onto various surfaces of the alveolar processes (blocks);
- distraction of the alveolar process in the transverse direction.
Lifting the floor of the maxillary sinus (sinus lift)
An increase in the vertical size of the alveolar process of the maxilla is shown when the bottom of the maxillary sinus is low.
Sinus fitting can be open, carried out through the anterior wall of the maxillary sinus, or closed. It is performed through a tooth socket or a hole in the bone of the bottom of the sinus using balloon technology and special instruments - blunt osteotomes - to detach the mucous membrane of the maxillary sinus and create space with osteogenic materials.
Raising the floor of the nasal cavity
An operation is performed to raise the floor of the nasal cavity if there is bone atrophy in this area and there is a need to introduce endosseous implants here. The operation is performed in an open way along the transitional fold, less often - through access from the nasal cavity or in an open way, through the alveolar process.
Relocation of the mandibular nerve
Surgery is necessary when the mandibular neurovascular bundle interferes with the installation of an intraosseous dental implant. The movement is performed along the entire length of the jaw body. To do this, the mandibular canal is opened, the neurovascular bundle is exposed and moved outward.
Other interventions
Other operations may combine elements of the above interventions and techniques.
Reconstruction, plastic surgery of supporting areas of bones and installation of dental implants can be carried out alternately - first, perform the necessary bone reconstruction, and after 2-6 months, implantation. This is necessary for organotypic restructuring of the bone graft to occur.
Bone reconstruction and installation of a dental implant can also be carried out simultaneously, or the implantation can be performed first, and if problems arise, additional bone reconstruction around the implant can be carried out.
Benefits of bone grafting
- Reliable adhesion of the implant to the bone tissue.
- Minimal trauma. Minor swelling and hematoma.
- High efficiency. Allows you to start prosthetics in a short time.
Before performing correction of the alveolar process, it is necessary to make sure that there are contraindications, for example, the absence of an allergic reaction to biomaterial and drugs. Dental treatment is not carried out for cancer and autoimmune diseases, as well as poor blood clotting. In some cases, surgery may be delayed until the underlying conditions have resolved.
Advantages of the method
The horizontal augmentation method allows you to obtain the optimal bone thickness for implantation of a metal implant. It is considered low-traumatic compared to other types of bone grafting, since it does not require the collection of donor material.
This method allows you to:
- achieve rapid restoration of bone tissue width;
- effectively eliminate atrophy and other jaw defects;
- grow tissue with a density suitable for forming a bed for the implant;
- accelerate the implantation of the titanium rod into the jaw.
Recommendations for rehabilitation
The rehabilitation period is aimed at restoring the functions of the affected area. After surgery it is recommended:
- Follow all doctor's recommendations.
- Avoid eating too cold or hot food.
- Follow the rules of oral hygiene.
- Avoid serious physical activity.
- Follow the recommendations for a gentle diet.
Additionally, oral baths using antiseptic solutions and the use of soft toothbrushes may be recommended to eliminate the risk of damage to the operated area. If you follow the recommendations, there are no risks of possible complications. Successful recovery depends on the skill level of the surgeon. Our AlfaDent clinic employs exclusively professionals who take advanced training courses and regularly improve their skills.