Dental caries is usually classified according to different indicators. One of the most widespread is Vinogradova’s classification, according to which there are compensated, subcompensated and decompensated forms of dental caries. We will tell you more about the symptoms and treatment features of different forms of the disease in this article.
In this article
- How does dental caries occur?
- Three forms of dental caries
- Compensated form of caries
- How is compensated caries treated?
- What is subcompensated caries and what are its features?
- Features of decompensated caries
- How is decompensated caries treated?
- Pulpitis as a complication of decompensated caries
- Periodontitis with decompensated caries
- Is it possible to prevent tooth decay?
- Conclusion
How does dental caries occur?
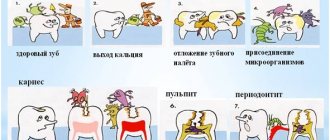
During caries in hard dental tissues, under the influence of organic acids, first areas of enamel demineralization are formed, and then carious cavities. Acids that destroy teeth are produced by cariogenic bacteria. This occurs during the fermentation process of carbohydrates that we consume in food. According to statistics, caries is the most common dental disease; it affects the teeth of people of any age, including the development of baby teeth immediately after teething.
There are different classifications of caries, in particular the Vinogradova classification. According to this division, there are compensated, decompensated and subcompensated caries.
Causes
In the history of dentistry, about four hundred theories of the occurrence of caries are known. Among the recognized ones are chemical-parasitic, physical-chemical, trophic, but none of them fully explains the etiology of the disease. Today it is believed that pathology develops against the background of the interaction of a chain of internal and external factors. This happens when demineralization processes in enamel prevail over remineralization. It is believed that the development of caries is directly related to the microflora in the oral cavity, where streptococci live.
Three forms of dental caries
Vinogradova’s classification is based on the degree of activity of dental caries:
- The compensated course of caries is characterized by the fact that the pathological process develops slowly, carious cavities are hidden under dense dentin, they are rare, and the disease progresses relatively slowly.
- The subcompensated form of the disease develops slightly faster than the compensated form. It is characterized by the appearance of dark areas on the enamel and horizontal spread without penetrating deep into the tooth.
- Decompensated caries is often multiple and spreads very quickly. With such caries, all teeth located near the cheeks are often affected.
The decompensated form is considered the most severe, in most cases accompanied by complications in the form of pulpitis or periodontitis.
Let's talk about all forms of caries in more detail.
Treatment of caries
Treatment of caries in the Lyubertsy dental clinic "VUGI" begins with an examination of the oral cavity by a dentist, a thorough diagnosis of the condition of all teeth with mandatory mechanical treatment of detected carious cavities. Mechanical impact is carried out using special systems using boron. After mechanical treatment of the carious cavities, medications are used, after which the carious cavity is filled with one or another filling material.
It is impossible to overestimate the importance of timely contacting a dental clinic for caries treatment. Patients should know that there is no difference between the extent of dental caries damage and the intensity of pain.
It is because of ignorance of this fact that patients get an appointment with a dentist with already severely advanced caries, when longer and more complex treatment and a large number of repeat visits are already required, which is especially offensive, since visits to a dentist-therapist require a fairly large amount of time ; In addition, this fact always leads to additional monetary costs.
In the initial stage of the disease, if such a possibility exists, non-operative treatment of caries consists of carrying out comprehensive professional oral hygiene; during these manipulations, the dentist removes plaque and restores the affected enamel. Such manipulations are carried out through the use of fluorides in the form of solutions, pastes, gels, and varnishes. Often such doctor’s actions are combined with the use of solutions of calcium salts and restorative drugs.
In acute forms of caries, the patient is prescribed a special diet rich in proteins and mineral salts and vitamins A, C, D. Calcium preparations are also prescribed, such as colecalciferol, calcinova, calcium carbonate, sodium fluoride.
Compensated form of caries
Among all the options for the course of caries, compensated is the most favorable. In this case, the pathological process is sluggish and destroys dental tissue slowly over several years. With compensated caries, remission is possible, which under certain circumstances can result in relapses. According to statistics, compensated caries develops more often than other forms.
It is characterized by smoothed symptoms:
- Acute pain is most often absent;
- the transition of carious lesions from one stage to another occurs smoothly and imperceptibly over several months or even years;
- with compensated caries, a white spot first forms on the enamel, which gradually darkens, becomes rough and less dense. At the dark spot stage, a painful reaction to temperature or taste stimuli is possible;
- The compensated form of caries is characterized by destruction of dentin while often maintaining the integrity of the tooth enamel. Therefore, the characteristic clinical picture is a carious cavity in a seemingly intact tooth crown.
Pathogenesis of caries: mechanism of disease development
Streptococci form colonies in the oral cavity - so-called dental plaques. This process goes through three stages:
- Formation of acellular organic film on the surface of the enamel - pellicles. The process takes up to several hours. The basis of the film is glycoproteins and other proteins in saliva.
- Collection of microorganisms and epithelial cells on the surface of the pellicle with subsequent growth of bacterial colonies. Continues for several days.
- Formation of mature dental plaque.
Dental plaque includes up to 70% microorganisms and has a mesh structure with semi-permeable properties. Carbohydrates easily penetrate into it and have a destructive effect on the tooth.
How does enamel destruction occur?
When eating carbohydrate foods, the microflora of the dental plaque instantly absorbs saccharides. This leads to a “metabolic explosion” and a sharp increase in acidity. After half an hour, the acidic environment is neutralized by saliva, but when carbohydrates are reintroduced, the pH level under the plaque decreases again, which leads to damage to the enamel due to increased permeability.
Against the background of the formation of organic acids on the enamel, demineralization increases, and the microspaces between the crystals of enamel prisms increase. This promotes more intensive penetration of microorganisms and their metabolic products into enamel microdefects. A cone-shaped lesion is formed, which spreads into the depths of the tooth. After some time, the surface layer of enamel dissolves - caries progresses and can lead to the removal of a baby tooth if no action is taken.
How does tooth resistance affect pathological processes?
Resistance is the ability of a tooth to withstand external influences. It depends on many factors:
- type of enamel hydroxyapatite, correctness of the protein matrix, degree of mineralization of the matrix, interaction of mineral phases and protein;
- the presence of defects in the enamel, the regularity of its structure, an electrical charge on the surface that prevents or promotes the adsorption of microorganisms;
- relief of the enamel surface, depth and shape of fissures, nature of the pellicle;
- type of structure of the skull, jaws, bite, proximity of teeth and the size of the spaces between them, etc.;
- functioning of the salivary glands;
- nutritional characteristics and somatic health.
The structure of enamel is formed at the genetic level and depends on mineralization processes.
Saliva
Saliva is the environment in which teeth are constantly present. Under favorable conditions, the processes of demineralization and remineralization occur harmoniously in it. If its composition is violated, a failure occurs. In combination with other cariogenic factors, changes in the composition of saliva provoke the formation of new lesions.
A change in the composition of saliva in an unfavorable direction occurs after taking sugar and easily digestible carbohydrates. To avoid this process, it is necessary to eliminate carbohydrates from the diet or get rid of dental plaque.
Other pathological causes contributing to the development of caries
The condition of the mother during pregnancy is of decisive importance for the health of the enamel. With toxicosis, carbohydrate metabolism disorders, gastrointestinal and thyroid diseases, chronic hypoxia, the mineralization of primary teeth in a child in the womb slows down.
Especially often, caries occurs immediately after teething in premature babies who are bottle-fed, as well as those who have suffered serious illnesses during the first year of life. The hardness of dental tissue depends on the state of the child’s digestive tract, the amount of fluoride in drinking water, and concomitant diseases during the first years of life.
Even the condition of the pulp affects the solubility of enamel. If the latter retains high functional activity, the enamel will remain hard. In turn, the condition of the pulp worsens after infectious diseases. In such children and adults, caries develops more often and more intensely, which is associated with a decrease in the immunological reactivity of the body.
How is compensated caries treated?
The method of treating compensated caries depends on the stage at which it is detected and, accordingly, on the degree of tooth destruction.
At the initial stage of a carious stain on the enamel, non-invasive methods that do not require drilling a dental crown can be effective.
- Remotherapy (remineralization).
Using special pastes, gels, and solutions, tooth enamel is saturated with calcium and fluoride ions - the main components of its mineral composition. They normalize the structure of the enamel, increase its protective properties and resistance to the corrosive effects of acid.
- Deep fluoridation.
It is similar to the remineralization procedure with the difference that the composition of medicinal preparations necessarily includes fluoride. It penetrates deep into the enamel, makes it stronger, has an antiseptic effect, and prevents the teeth from losing calcium and other minerals.
- Fissure sealing.
Fissures are natural grooves on the surface of chewing teeth. They can be of different shapes and depths, and due to their anatomical features, food debris easily accumulates in them. In addition, the enamel in the fissure area is thinner compared to other areas of the dental crown. The sealing method is often used to prevent caries in the chewing teeth of children and adults with deep grooves on their teeth. The essence of the method is that the dentist seals the natural recesses of the dental crown with a special sealant, so that food debris no longer accumulates in them and bacteria cannot multiply.
- Filling.
This method treats a compensated form of caries in the later stages, when cavities have formed in the dentin of the tooth. Most often, the dentin treatment process is painful, so the procedure is performed under local anesthesia. After the anesthetic injection takes effect, the doctor prepares the affected tooth with a drill, removes carious tissue, and then covers the cured tooth with high-quality filling material. The best treatment option is without drilling or filling. Methods of remineralization and deep fluoridation are safe, painless, and do not cause discomfort in the patient. But they are effective only at the initial stages of the carious process.
Therefore, it is important to regularly check the condition of your teeth with a dentist (for compensated forms of caries, a visit once a year is recommended) in order to notice the beginning of caries as early as possible.
Caries
4059 16 August
IMPORTANT!
The information in this section cannot be used for self-diagnosis and self-treatment.
In case of pain or other exacerbation of the disease, diagnostic tests should be prescribed only by the attending physician. To make a diagnosis and properly prescribe treatment, you should contact your doctor. Caries: causes, symptoms, diagnosis and treatment methods.
Definition
Caries is an infectious lesion of the teeth in which demineralization and softening of the hard tissues of the tooth occurs with the formation of a defect in the form of a cavity. This is the most common disease of the dental system. Caries occurs among all age groups, but more often among adults over 35 years of age, where it accounts for 98-99%.
Causes of caries
In the oral cavity of any person there live a large number of microorganisms that are in balance and actively interact with the human body and with each other. This balance may change briefly under the influence of various factors, for example, after a teeth whitening procedure, but then the balance is restored again. If the body's defenses are reduced, the changes can be more significant and lasting.
Various bacteria, fungi and protozoa live on the oral mucosa, in the ducts of the salivary glands and in saliva, in gingival fluid and oral fluid, but most of them live in dental plaque - up to 90% of all microflora.
Dental plaque is a soft sticky deposit on the surface of teeth containing a large number of microorganisms, their metabolic products, epithelial cells, leukocytes, proteins and lipids of saliva. The formation of dental plaque is a natural process, and in the absence of timely and thorough dental care, it forms within 1-2 days. As a result of structural changes in plaque, dental plaques form quite quickly. Bacteria present in dental plaque and plaques actively “exchange information”, build a large number of connections, and then stick together, forming a microbial biofilm. In a biofilm, microorganisms exchange genetic material, nutrients, and remove metabolic products. The creation of such a biofilm protects bacteria from the body's defense cells and from the action of antibiotics. As a result of the vital activity of microbial biofilm, a large amount of organic acids is formed, under the influence of which demineralization of tooth enamel begins. Small defects form, microorganisms penetrate there, destroying the enamel further, resulting in the formation of a cavity in the tooth - caries.
Carbohydrates serve as food for microorganisms, so eating sweet foods contributes to the development of caries.
In addition, predisposing factors are a decrease in the body's defenses, smoking, poor oral hygiene, and taking antibiotics - all this leads to an imbalance in the oral microflora, resulting in the proliferation of streptococci and lactobacilli, which are responsible for the production of organic acids and the development of caries.
Classification of caries
Doctors classify caries depending on the stage and location of the lesion. The stage of initial caries, in which the process does not extend beyond the enamel-dentin boundary, is called the white or chalky spot stage. This is followed by the stage of dentin caries, in which the disease crosses the enamel-dentin boundary without affecting the pulp, and the stage of cement caries with damage to the exposed surface of the tooth root in the cervical region.
Focal demineralization of enamel is characterized by the appearance of a dark pigmented spot within the enamel and is called the stage of suspended caries.
Based on the location of the cavities, there are 6 classes of the disease:
Class I - cavities localized in the area of grooves on the chewing surface of the teeth (fissures) and natural recesses of the incisors, canines, molars and premolars.
Class II - cavities located on the contact surface of molars and premolars.
Class III - cavities located on the contact surface of the incisors and canines without breaking the cutting edge.
Class IV - cavities located on the contact surface of the incisors and canines with a violation of the angle of the crown of the tooth and its cutting edge.
Class V - cavities located in the cervical region of all groups of teeth.
Class VI - cavities located on the cusps of molars and premolars and the cutting edges of incisors and canines.
Symptoms of caries
Symptoms of the disease depend on its stage. A sign of initial caries is a change in the color of the tooth enamel in a limited area and the appearance of a chalky or gray stain, lacking shine - a focus of demineralization. Then an enamel defect develops, and then a cavity. Patients with caries at the stage of cavity formation note increased sensitivity of the tooth to chemical, temperature and mechanical irritants, while the painful sensations disappear immediately after the irritant is eliminated. A defect can be seen on the visible surface of the teeth.
Further, tooth damage spreads to the underlying tissues - to the upper layers of dentin, after which, in the absence of treatment, the process captures the deep layers of dentin and approaches the pulp - soft connective tissue penetrated by blood vessels and nerve plexuses. At this stage, patients also note increased sensitivity to irritants and pain during chewing.
When the dental pulp becomes inflamed – pulpitis – severe toothache begins. If the disease is not treated, the pathological process can spread beyond the tooth into the bone tissue and periodontitis will develop.
Diagnosis of caries
To make a diagnosis, the doctor examines the oral cavity, examining the mucous membrane, establishes the presence of fillings and the degree of their adherence, the presence of defects in the hard tissues of the teeth, and notes the number of teeth removed. The dentist carefully evaluates the condition of all teeth, determines the density of hard tissues, texture and degree of surface uniformity, checks pain sensitivity, and probes the identified carious cavity. If indicated, radiography is performed.
Which doctors should I contact?
Dentists treat caries.
Treatment of caries
The main goals of caries treatment are to stop the pathological process, restore the shape and function of the affected tooth, prevent the development of complications and restore the aesthetics of the dentition. If the carious lesion is limited to the enamel, then patients may be prescribed deep fluoridation of the hard tissues of the tooth to prevent further development of the process.
If a defect occurs in the hard tissues of the tooth, conservative remineralizing treatment does not have an effect; in this case, the altered tissues are removed and the tooth crown is restored using a filling.
Complications of caries
In almost half of patients aged 35-44 years, there is a need for filling and prosthetics of the affected tooth, and doctors have to resort to tooth extraction in almost a quarter of cases. With late treatment of caries, the pathological process can spread deeper into the dental pulp, and from the infected pulp, inflammation through the tooth canal penetrates further into the bone and under the periosteum of the jaw with the development of inflammation of the periosteum - periostitis or gumboil. Tooth extraction as a result of untimely treatment, which leads to complications, causes deformation of the dentition and can even lead to pathology of the temporomandibular joint.
Dental caries can cause problems with chewing function.
Prevention of caries
To effectively prevent the development of caries, it is necessary, firstly, to prevent the creation in the oral cavity of conditions conducive to the emergence of microbial films and the carious process, and secondly, to increase the caries resistance of dental tissues. The main methods of prevention are regular oral care with proper brushing technology, the use of dental floss, the use of fluoride toothpastes, mouth rinses, reducing sugar consumption and regular dental examinations (once every 6 months).
Sources:
- Clinical recommendations (treatment protocols) for the diagnosis of “Dental caries” Approved by Resolution No. 15 of the Council of the Association of Public Associations “Dental Association of Russia” dated September 30, 2014, updated on August 2, 2022.
- A.I. Khavkin, Yu.A. Ippolitov, E.O. Aleshina, O.N. Komarova. Oral microbiota: protective or pathogenic factor? // Issues of practical pediatrics. – 2015. – T. 10. – No. 4. – P. 49-54.
IMPORTANT!
The information in this section cannot be used for self-diagnosis and self-treatment. In case of pain or other exacerbation of the disease, diagnostic tests should be prescribed only by the attending physician. To make a diagnosis and properly prescribe treatment, you should contact your doctor.
What is subcompensated caries and what are its features?
Subcompensated caries occurs in approximately 25% of children with dental caries. This form is characterized by an average rate of spread of the pathological process. Characteristic features are dull enamel and superficial lesions without deep tissue involvement. Most often, subcompensated caries does not cause discomfort or pain, so it can only be detected during an examination by a dentist.
People with this form of caries are recommended to have scheduled visits to the dentist two to three times a year, as well as oral sanitation and preventive measures.
Bitter sweet truth
Of course, people have known for a long time that “sweets spoil teeth,” but it was possible to prove the role of diet in the occurrence of caries only when, in the course of numerous independent experiments, it was established that streptococci are present in dental plaque in people free from caries. The first step in proving the “guilt” of sugar was taken by Danish professor Frederik von der Fehr from the Royal Dental College in Aarhus. In 1970, von der Fehr conducted an experiment in which a group of volunteers with good tooth enamel completely eliminated oral hygiene - they did not brush or rinse their teeth after eating. Half of them also rinsed their mouths with a 50% sucrose solution several times a day. Lack of hygiene increased the number of bacteria in plaque, but when comparing the condition of the teeth of those who rinsed with a sweet solution with the control group, more obvious signs of caries were found - demineralization of the enamel and the appearance of stains on it.
If earlier, for example, in the not so distant 18th century, sugar was an expensive product and not everyone appeared in the diet, but now, according to dental surveys, most people in Russia and many other countries eat sweets every day. As Edith Kuzmina notes, it is not so much the amount of sweets eaten at a time that is important, but the frequency of its consumption.
Ideally, dentists advise eating sweets as little as possible and replacing fermentable sugars - glucose, sucrose and fructose - with sorbitol, mannitol and xylitol. These polyhydric alcohols have a sweet taste and are often used as sweeteners (for example, for diabetes), and carious streptococci simply cannot utilize them. Natural xylitol is found in strawberries and carrots. And if you still can’t give up sweets, then it’s better to eat them not “alone”, but together with other foods - this reduces cariogenicity. The same sour apples, for example, require copious amounts of saliva, and it dilutes and, having an alkaline reaction, partially neutralizes the acid formed in the mouth after the fermentation of sucrose and glucose.
Features of decompensated caries
The decompensated form of caries is the most intensive type of development of dental disease. Decompensated caries is considered the most severe and dangerous. The first signs of the disease are rough matte enamel, darkening of the fissures; when opening the dental crown, a large carious cavity is most often discovered, and severe pain is noted when probing with a dental probe.
This form of caries develops very quickly and in most cases is accompanied by complications (tooth chipping, inflammation of adjacent tissues, complete loss), because the body cannot independently compensate for the pathological process. Against the background of the carious process, inflammation quickly penetrates into the pulp, then into the tissue surrounding the tooth. As a result, pulpitis and periodontitis occur.
Manifestations of caries in children
The appearance of light or dark spots on tooth enamel
The first sign of caries in children is white spots on the enamel, resulting from calcium loss. At this stage, treatment may be minimal; often the doctor prefers minimally invasive methods, for example the ICON technique. The dentist applies a special preparation to the affected tooth tissue, thereby blocking the proliferation of bacteria and the development of the infectious process - caries is “preserved.”
If the white areas darken, dentin, the deep tissue of the tooth, is involved in the pathological process.
Cavity formation
In a child, the caries process develops very quickly, and the next stage is the formation of cavities. Most often they are visible upon examination even with the naked eye, and the child complains of pain while eating.
Reaction to food temperature
With the further development of the carious process, the affected tooth begins to react to hot, cold and sweet foods and drinks.
Pain
Pain occurs while eating - when food gets on a carious tooth. If the infectious process has spread to the pulp, the child will complain of pain constantly. Often unpleasant sensations occur during night sleep.
5.Bad breath
Food particles accumulate in carious cavities, bacteria cause rotting, so parents often complain about bad breath.
How is decompensated caries treated?
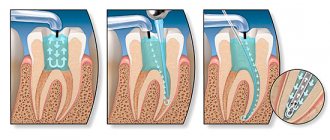
If a hole has already formed in the tooth, treatment will consist of preparing the dental tissue, opening it, cleaning the carious cavity, removing the nerve if necessary, and then filling it.
The decompensated form of caries is characterized by large-scale damage to the dentition, so it is often necessary to treat several teeth at once. Or several visits are scheduled for alternate treatment. This depends on the age of the patient, the extent of the carious lesion, the need for anesthesia and a number of other factors.
After treating all teeth affected by caries, the patient is scheduled for scheduled visits to the dentist at least 3-4 times a year. Also mandatory measures for decompensated caries are recommendations on proper nutrition and oral hygiene, consultation with a doctor, ingestion of anti-caries medications, sanitation of the oral cavity, and local prevention.
Mechanism of destruction
To understand how caries occurs, you first need to know that tooth enamel is approximately 95% composed of the mineral calcium hydroxyapatite Ca10 (PO4)6 (OH)2. Its hexagonal crystals combine into prisms and provide strength to bones and teeth. The enamel of just one incisor contains about 5 million mineral prisms.
Like all hydroxyl (“alkaline”) minerals, hydroxyapatite is destroyed by acids. This happens due to a violation of the notorious acid-base balance, known to everyone from chewing gum advertising. When acid enters the mouth, for example with a sip of wine, our body tries to neutralize it, and calcium from the enamel migrates into saliva. And without calcium, mineral prisms collapse like houses of cards. If the process is repeated, the acids attack the dentin located under the enamel. Then a carious cavity appears in the tooth - a cavity.
Particularly scary are simple organic acids, such as acetic, lactic and citric. Therefore, when we drink wine or eat an orange, the enamel of our teeth is doomed to partial destruction. But acids appear in the mouth even without oranges. Plaque streptococci feed on the carbohydrates we eat, and the by-product of their fermentation is aggressive acids. The simpler the carbohydrate, the faster acid is formed from it. This means that the more often we eat simple carbohydrates (glucose, fructose, sucrose), the more caries progresses.
The enamel that forms the crown of a tooth is the hardest substance in the human body. However, it cannot withstand the chemical attack of the waste products of S.mutans streptococci.
The approximately mechanism of development of this disease was described by the American dental scientist Willoughby Miller at the end of the 19th century, calling it the chemical-parasitic theory. This means that, on the one hand, the appearance of caries is a chemical process, but without parasitic microbes it would not be so large-scale or would be completely neutralized. According to the head of the Department of Caries Prevention at Moscow State University, Edith Kuzmina, three reasons are to blame for the appearance of caries: plaque with bacteria, carbohydrate foods and weak resistance of tooth enamel. This means that there can only be three ways to combat caries: eat as little simple sugars (easily fermentable carbohydrates) as possible, make tooth enamel more resistant to decay, and, finally, rid your teeth of plaque in which streptococci are hidden.
Pulpitis as a complication of decompensated caries
The course of caries in a decompensated form can be complicated by inflammation of the neurovascular bundle - the pulp. The inflammatory process in this area is called pulpitis. It occurs when the infection spreads beyond the tooth
The pulp contains blood vessels, nerves, and nourishes dental tissue. If it becomes inflamed, there is a risk of tooth loss due to loss of vitality. With pulpitis, the patient complains of severe, prolonged pain, which is often pulsating in nature and radiates to the temples and ears. Painful attacks are repeated with a certain frequency, last for five minutes, intensify in a supine position.
Depending on the severity and neglect of the process, pulpitis is treated with a conservative or surgical method. At an early stage, the doctor, if possible, preserves the pulp and root of the tooth, eliminating the inflammatory process with the help of medications. If the inflammation is too strong, there is a risk of it going beyond the pulp, and it is not possible to stop the pathological process with medications, in this case the doctor chooses a surgical treatment tactic, partially or completely removing the pulp. This option is less preferable, because without a neurovascular bundle, the tooth becomes virtually “dead” and serves much less time.
The complications of caries should be taken seriously and at the first symptoms, contact your dentist. If you neglect timely diagnosis and treatment, the infection can spread to other organs and tissues, which can lead to serious disruptions in the functioning of the entire body. In particular, untreated pulpitis is dangerous for the development of gumboil, periodontitis, pulp necrosis and even sepsis.
Demographic and social changes in recent decades have determined the dynamic development of an independent field in medicine - gerontology. Along with social and psychological problems associated with the aging population, medical problems arise in providing care to elderly and older people [1]. The need for an individual approach to treatment planning in the older age group is dictated by several aspects. On the one hand, a number of profound age-related changes in metabolism and various body functions, including significant changes in the activity of the cardiovascular, endocrine systems, and gastrointestinal tract, increase at the age of 70 years and older, which potentially affects the condition of the organs and tissues of the cavity mouth and complicates the provision of effective dental care [2, 3]. On the other hand, the modern concept of healthcare development is based on a preventive approach aimed at preventing diseases, developing and organizing activities that improve oral health in the population [4-6]. Timely use of a set of primary and secondary prevention measures in people of the older age group increases the likelihood of preventing premature aging and improving the quality of life. The achievements of modern dentistry create the prerequisites for higher preservation of natural teeth in older age, which requires expanding the types of dental care in this category of the population [7].
In order to ensure adequate planning of the volume and types of dental care based on taking into account psychosomatic and socio-age characteristics, as well as to increase the stability of treatment results, in-depth epidemiological data are required on the characteristics of the dental and general somatic status of this category of patients. This study is devoted to studying the characteristics of the epidemiology of caries in people of the older age group.
Material and methods.
We conducted a comprehensive examination of 100 patients aged from 70 to 86 years (average age in the examined group 78.0±0.16 years), including 40 women and 60 men. All patients received medical and dental care in one of the subordinate medical institutions of the Administration of the President of the Russian Federation.
Pathology of the cardiovascular system (coronary heart disease, hypertension) and endocrine system (diabetes mellitus) was recorded in all examined patients.
Assessment of dental status included registration of caries-affected, restored and extracted teeth. Diagnosis of caries complications was carried out on the basis of clinical and x-ray examination data (including a mandatory survey x-ray examination for all subjects). During the examination, teeth with primary endodontic pathology were identified, as well as teeth after endodontic treatment, including teeth with signs of endodontically caused pathology (chronic periodontitis) after endodontic treatment.
To assess the condition of the teeth we used: caries intensity index KPU; the ratio of the number of teeth with untreated carious cavities to the number of restored teeth (restored with fillings, crowns) - K/R index; the ratio of the number of teeth with complicated forms of caries (including teeth with primary endodontic pathology and teeth with endodontically caused pathology after endodontic treatment) to the number of carious and restored teeth - OK/KP index; the ratio of the number of teeth with untreated carious cavities to the sum of extracted and restored teeth - the K/UR index; the ratio of the number of extracted teeth to the number of restored teeth - U/R index.
To analyze the results, methods of variation statistics were used, including correlation analysis (using the linear Pearson correlation coefficient).
Results.
In both age groups, the majority of those examined had pathologies of the cardiovascular and endocrine systems. There were no statistically significant differences between the selected age groups for any of the studied indicators. In general, in the group of older people examined, a high intensity of caries was established: the average value of the KPU index was 19.50±0.56. Of the total number of teeth affected by caries, most (more than 80%) had restorations (they were restored with fillings or crowns), the average value of the K/R index (the ratio of the number of teeth with untreated carious cavities to the number of restored teeth) was 0.23±0.05, the index K/UR (ratio of the number of teeth with untreated carious cavities to the number of extracted and restored teeth) - 0.11±87. During dental treatment, conservative methods of sanitation were generally used more often than surgical ones: the average value of the U/P index (the ratio of the number of extracted teeth to the number of restored teeth) was 0.96±0.34. An analysis of the ratio of caries complications to dental caries showed the following. The proportion of teeth with complicated forms of caries amounted to almost half of the total CP value (carious and restored teeth): the average value of the OK/CP index (the ratio of the number of teeth with caries complications to the number of carious and restored teeth) was 0.48±0.73. There was no significant difference in data between the two age groups. Analysis of caries intensity indicators in different patients, taking into account the type of somatic pathology, did not reveal significant differences in any of the age groups. There were no significant differences in the average values of the indices KPU, K/R, OK/KP, K/UR, U/P depending on the type of somatic pathology. As a result of the analysis of correlation interactions, a significant direct correlation (0.55) was revealed between the KPU index and the K/P index, as well as an inverse correlation (0.12) between the KPU index and the U/P index.
The examined patients revealed a high rate of caries intensity: the average value of the KPU index was above 19. As a result of data analysis, patterns were discovered: the degree of sanitation was more than 80% for preserved teeth and more than 90% taking into account cured and extracted teeth. It was found that conservative sanitation methods were used in the examined group somewhat more often than surgical methods (tooth extraction). The alarming rate is the high rate of caries complications, which account for 48% of all carious and restored teeth. The identified positive correlation (0.55) between the K/P and KPU indices indicates that the increase in the KPU caries intensity indicator in the examined group of people is associated primarily with the development of new carious cavities or relapses of caries, which are not always sanitized in a timely manner.
The data obtained indicate that currently, when providing dental care to older people in departmental medicine, there is a tendency to increase the preservation of natural teeth through the use of effective tooth-preserving methods of non-surgical treatment. At the same time, caries complications requiring endodontic treatment or surgical sanitation account for almost half of all caries-affected or treated teeth (according to the KP indicator). The data obtained confirm the need for regular dental examinations and clinical follow-up of patients with the mandatory use of not only clinical examination methods, but also radiological diagnostic methods. Plain X-ray examination (orthopantomography or volumetric cone radiation diagnostics) is preferable for patients in the older age group, both in order to minimize radiation exposure and from an ergonomic point of view. The lack of significant differences in the values of the PCI index in patients with somatic pathology in the older age group can be explained by the fact that dental care was provided throughout the patient’s life, and by the age of 70, patients already had high values of the PCI index. At the same time, the high prevalence of cardiovascular system pathology (CHD, hypertension) in the examined group gives grounds for recommendations to introduce a number of therapeutic and diagnostic measures as a standard for examining a dental patient of this age category, such as mandatory measurement of blood pressure and medical history. about drug therapy for cardiovascular pathology and, if indicated, consultation with the attending physician-intern.
Conclusion.
The obtained data on the trend towards an increase in the preservation of natural teeth in older people receiving dental care in the conditions of departmental medicine determine the feasibility of implementing primary and secondary dental prevention programs for this category of people. In the examined group of people, caries complications requiring endodontic treatment or surgical sanitation accounted for almost half of all caries-affected or restored teeth, which determines the importance of including radiological diagnostic methods in the dental examination protocol for patients in the older age group. The data obtained provide the basis for the conclusion about the advisability of developing special (specialized) standards for diagnosis and treatment in gerontostomatology, taking into account age characteristics and characteristics of somatic status.
Periodontitis with decompensated caries
In addition to pulpitis, with decompensated caries another serious complication often develops - inflammation of the tissues surrounding the tooth root. This disease is called periodontitis.
The periodontium is a ligamentous apparatus that holds the tooth in the jaw and provides shock absorption. If an inflammatory process develops in the periodontal tissues, this can lead to loosening and tooth loss. Against the background of periodontitis, ulcers can form, the removal of which will require surgical opening of the gums.
Periodontal inflammation can be acute or chronic. In the first case, inflammation develops rapidly, accompanied by darkening of the tooth, acute pain, swelling of the affected tissues, and inflammation of the cheek. Chronic periodontitis is characterized by more smoothed symptoms, pain syndrome may be absent. Treatment for the chronic form is long and difficult and can take several months.
Periodontitis greatly weakens the immune system and creates a source of chronic infection in the body.
Is it possible to prevent tooth decay?
The development of any form of caries process is facilitated by a number of factors: poor diet with a large amount of carbohydrates, poor oral hygiene, insufficient intake of vitamins and minerals, rare visits to the dentist for the purposes of prevention and early diagnosis.
Addressing these risk factors helps reduce the risk of developing tooth decay or detect it at an early stage, when treatment can be as simple and effective as possible.
These preventive measures reduce the likelihood of developing any form of caries:
- Reducing the amount of carbohydrate and sweet foods in the diet, rare snacks, avoiding feeding the child at night and before bedtime. This recommendation is due to the fact that cariogenic bacteria feed primarily on carbohydrates. The longer food remains remain in the mouth, the more acid that is destructive to teeth will have time for microorganisms to produce.
- A balanced diet containing plenty of calcium, phosphorus and fluorine-containing foods. These minerals form a healthy and strong enamel structure that can resist the negative effects of cariogenic bacteria.
- Regular proper brushing of teeth using a brush, paste, floss, irrigator. Twice a year, professional teeth cleaning at the dental clinic. These measures help to get rid of dental plaque consisting of bacteria in a timely manner, and thereby reduce their negative impact on the teeth.
- Routine visit to the dentist even in the absence of complaints. With a compensated form of caries, it is recommended to visit a doctor once a year, with a subcompensated form - 2-3 times a year, with a decompensated form - 3-4 times a year. This recommendation is due to the fact that early caries often does not manifest itself with pronounced symptoms. For example, at the spot stage, the only sign of a carious lesion is whitish spots and lines on the enamel. It is quite difficult to notice them with the naked eye, but an experienced dentist will easily detect the beginning of the carious process.
If you miss the onset of the disease, a cavity forms in the tooth and complications develop. The later treatment is started, the more complex and painful it will be.
Publications in the media
Dental caries is a localized lesion of the hard tissues of teeth, manifested by demineralization and progressive destruction of enamel and dentin with the formation of a defect in the form of a cavity.
Epidemiology • Caries occurs at all ages; the prevalence of caries reaches 100%, which, according to WHO experts, makes it possible to classify it as a pandemic • Dental caries damage is assessed by the intensity indicator: “KPU index” - for permanent teeth, “KP index” - for temporary teeth, “KPU+kp index "- in a mixed dentition (the index is the sum of the number of teeth affected by caries [K], filled [P] and removed [U]).
Risk factors • Pathological pregnancy • Acute infectious and chronic systemic diseases • Sensitization of the body • Anti-infectious vaccinations and other conditions accompanied by decreased immunity • Excessive consumption of carbohydrates • Insufficient intake of mineral components and trace elements, in particular fluoride • Inadequate oral hygiene.
Etiology. Dental caries is an infectious disease associated with associated microflora (lactobacillus, veyonella, etc.), where the leading role is played by streptococci (S. mutans, S. sanguis, S. mitis, S. salivarius). The most cariogenic is S. mutans, which produces lactic acid only from glucose.
Pathogenesis. Development is determined by genetic resistance (caries resistance) or predisposition to the disease.
• A decrease in resistance to caries is associated with a decrease in the calcium content in the surface layer of enamel, more precisely with a decrease in the molar ratio “calcium/phosphorus” in hydroxyapatites below the minimum level (1.30).
• Immune disorders are associated with a decrease in the content of secretory IgA in saliva, which normally, by preventing the adhesion of microorganisms to the enamel surface, prevents the formation of soft plaque.
• Microorganisms form dental plaque (soft plaque), which is fixed on the surface of the tooth on the polysaccharide stroma.
• The microflora of the plaque damages the organic basis of the enamel, in which, with the loss of the ability to fix the mineral substrate, the process of incipient demineralization begins to predominate. In the resulting carious defect, microorganisms undergo enzymatic breakdown of the organic substances of the tooth.
Classification
• Based on the depth of the lesion, they distinguish •• initial caries •• superficial caries •• medium caries •• deep caries.
• Based on localization, they distinguish •• fissure caries - damage to grooves and natural depressions •• approximal caries - damage to contact surfaces •• cervical caries - damage to a tooth near its neck •• carious defects in other areas are considered atypical.
• According to the course, caries is distinguished as acute, acute, chronic and suspended.
Clinical manifestations. The clinical picture is very diverse and is determined by the nature of the process and the depth of damage to the hard tissues of the tooth.
• Acute forms (acute and acute) of caries are characterized by rapid development of the process, when within a short time (1–1.5 years) most of the teeth are affected; Often two or several foci are found in them. A carious defect is characterized by slight destruction of the enamel and extensive destruction of the underlying dentin. The walls and bottom of the cavity are formed by softened, low-pigmented dentin. When cold, sour or sweet food gets into the cavity, severe pain occurs. Plaque forms quickly. The viscosity of saliva increases, the activity of salivary blood lysozyme decreases, and the content of secretory IgA decreases. Impairments in the functional state of the autonomic nervous system may be detected.
• Chronic dental caries develops unnoticed when one, or less often 2-3, teeth are sporadically affected, and such damage can go unnoticed for a long time. The carious focus is localized on typical surfaces, affecting molars, premolars and rarely the upper incisors •• Initial caries is a focus of demineralization of the enamel in the form of a spot on the labial and cheek surfaces of the teeth, closer to the neck, small in size, matte, whitish or dirty gray in color. Its contours are uneven, but clearly visible after staining with methylene blue solution. The probe glides easily over the surface without detecting a defect. There are no unpleasant or painful sensations. The teeth are usually abundantly covered with soft plaque •• Superficial caries is an enamel defect that does not cause unpleasant subjective sensations and is easily detected. Has clear spherical outlines; no changes are usually noted in the enamel surrounding the defect •• Middle caries is a cavity defect affecting the enamel-dentin junction and dentin layers. It has clear edges, the bottom and walls are dense and pigmented to varying degrees. There are no complaints or food gets stuck •• Deep caries is a cavity defect extending to the area of deep (suprapulpar) dentin: large in size, usually filled with decaying contents of a dirty gray color. There may be complaints of quickly passing pain when cold or sour food gets into the cavity. Cold stimulus causes pain. Probing the cavity floor is sensitive. The electrical excitability of the pulp is reduced to 20 μA.
Diagnosis of caries is based on complaints and the time period during which damage to several teeth occurs.
• An objective examination includes examination, probing and mandatory assessment of the hygienic condition of the oral cavity.
• Additional methods include thermometry (using water at a temperature below 18 °C), vital staining with 2% aqueous methylene blue or electroodontodiagnostics, radiography.
• To identify hidden and initial forms, transillumination, luminescent examination of the enamel surface and determination of the electrical conductivity of hard dental tissues can be used.
• To identify predisposition to caries, the acid resistance of enamel and its ability to remineralize are determined.
Differential diagnosis • Complicated stages of caries • Dental diseases of non-carious nature.
TREATMENT
Diet. In acute forms of caries, a diet rich in proteins and mineral salts is prescribed; vitamins A, C, D, B1, B6.
Drug treatment • General treatment is indicated for acute forms of caries. Combined calcium preparations are prescribed (calcinova, calcium-D3-nycomed); sodium fluoride orally 4–6 mg/day • Local non-operative treatment of initial caries consists of professional hygiene (removal of dental plaque) and remineralization of the affected enamel, which is carried out using fluorides in the form of solutions, pastes, gels, varnishes, often in combination with solutions of calcium salts, or remineralizing drugs (Remodent).
Surgery. Operative and restorative treatment of caries consists of anesthesia, instrumental treatment (necrectomy) of the tissues forming the bottom and walls of the carious cavity, and its subsequent filling with filling material or inlay.
Non-drug therapy. For initial caries, application or physical treatment methods are used: electrophoresis, ultraphonophoresis. For acute caries, UV irradiation is recommended.
Forecast. Without treatment, caries, with the exception of paused ones, necessarily develops into complicated forms.
Prevention. Aimed at increasing the resistance of teeth to caries and combating plaque formation.
• A balanced diet with mandatory consumption of milk and dairy products, sufficient intake of vitamins, limitation of easily digestible carbohydrates (sucrose, glucose). It is extremely important to introduce fluoride preparations into the body with drinking water (1 mg/l) or other fluoridated products (milk, salt).
• Treatment of acute infectious and concomitant diseases, carrying out general health measures.
• Regular and high-quality oral hygiene plays an essential role: twice-daily brushing of teeth using anti-caries pastes is recommended.
ICD-10 • K02 Dental caries