Purpose of the dental system
The biological mechanics of the dental system and its understanding lead to timely recognition of pathologies of teeth and soft tissues of the oral cavity. The normal functioning of the temporomandibular joint largely depends on the structure and normal functioning of the periodontium - the soft tissues surrounding the tooth cavity.
The anatomy and physiology of the structure of the periodontium determines the biomechanics of the structure and the characteristics of the periodontium. In addition, periodontal biomechanics helps in the functioning of other organs.
Knowledge of the laws of biological mechanics of the jaw and joints helps to design and use features, as fundamental knowledge on the topic of prosthetics and dental implants. Knowledge of the anatomical features of the jaw is necessary in the manufacture of structures and dental materials.
Devices have been developed that almost completely repeat the movements of the jaw and make it possible to reproduce anatomically similar structures to the human jaw. Popular devices include the occluder, facebow, and articulator. The latter design plays an important role in the fitting and creation of individual prostheses.
If disorders of the lower jaw occur, disruptions in articulation, speech, nutrition and swallowing occur. Today, a system of articulation of movements has been developed, led by such authors as Ganau, Gisi, Monson. These authors most accurately described the biomechanics of mandibular movements.
The authors claim that dysfunction of the lower jaw, as well as sore neck muscles, necessarily lead to breathing problems. Different angles of inclination of the lower jaw determine human health.
Occlusion is a condition characterized by full contact of both jaws, which ensures complete chewing of food. Therefore, the contact of teeth is a determining factor for the characteristics of chewing mechanisms.
The work and action of the lower dentition during chewing is due to the synchronous work of all muscles and joints. The work occurs under the influence of the central nervous system. In this case, displacements that occur spontaneously occur under the influence of the neuromuscular structure.
Conscious movements of the dentition include the moment food enters the mouth and swallowing food. The remaining movements that occur after eating food are the result of unconscious motor functions of the body.
The lower part of the human masticatory apparatus is the only moving bone in the human body. However, the connecting and muscle tissue, which sets the mechanism in motion, is of great importance in the structure of the masticatory row and in the normal functioning of the muscles.
In the structure of the lower dentition, there are several muscle groups that are responsible for various movements of the jaw.
Clicking sounds when opening the mouth
The jaw clicks... More precisely, it clicks at the top of the lower jaw... Even more precisely, in the area of the branch of the lower jaw, closer to the ear. Clicks when opening and closing the mouth. How to get rid of clicking jaw?
Of course, the jaw itself cannot click. And such symptoms are a sign of dysfunction of the TMJ (temporomandibular joint), which is located in this area.
This joint is the area of attachment of the lower jaw to the skull (more precisely to the temporal bone of the skull). And ensures mobility of the lower jaw. It is this mobility that allows us to open our mouths for eating (chewing) and talking (singing, screaming). A click in the TMJ area is not a good sign. A sign (symptom) indicating that if left unattended, the same mobility of the lower jaw may, in the long term, be impaired.
Diagnostics is the first and key step in the treatment of clicking when opening the mouth. Do you want to know why it’s impossible to do without diagnostics?
In order to understand the mechanism of occurrence of such clicks, a brief excursion into the anatomy and biomechanics of the temporomandibular joint is necessary.
This joint is formed by the articular head of the lower jaw (10) and the articular fossa of the temporal bone. The fossa and the head are incongruent with each other, i.e. do not match in relief (shape). To “make friends” the surfaces of the fossa and the head (condyle), i.e. make them congruent to each other, at the top of the head there is an articular disc (2). It consists of cartilage tissue. And it has a biconcave shape, i.e. The disc cartilage is wider at its edges and narrowed in the center (this is important to remember!). The articular disc normally “accompanies” the articular head during movement of the lower jaw.
Temporomandibular joint.
But under certain conditions, for example, with distal occlusion, when the lower jaw is located posterior to the norm, the articular disc appears anterior to the articular head. Well, and, accordingly, it becomes an obstacle to its (head) movement. At first (at the beginning of the onset of dysfunction), while the ligament that returns the disc to its place still retains its elasticity, the disc becomes in the correct position when the mouth is opened. This “return” of the disk is accompanied by a noise effect in the form of a characteristic click. Because, as has already been said, the disk is wider at the edges than in the middle. And when the articular head “slips” through the wide edge of the disc, a noise (clicking) is produced.
Deflexion and Deviation. Trajectory of the lower jaw when opening the mouth with TMJ dysfunction.
It should be added that TMJ dysfunction is often accompanied by deviations of the lower jaw when opening the mouth to one side. And in the initial stages of dysfunction, when the articular disc is still capable of self-reduction, the return of the lower jaw to its normal trajectory is precisely accompanied by a click in the joint. This temporary deviation of the lower jaw is called deviation.
In later stages, the wide edges of the cartilage disc wear away, the ligament that returns the disc to its place weakens (loses elasticity) and the disc can no longer return back (to where it should be). Accordingly, the opening of the mouth is sharply limited (up to 2 cm when the norm is 4-4.5 cm). Since the disc, being an obstacle to the movement of the articular head, does not allow the lower jaw to make full-amplitude movement in the temporomandibular joint). At this stage, a persistent deviation in the trajectory of movement of the lower jaw when opening the mouth (deflexion) may already be observed. Which leads to misalignment of the jaw.
Well, then - more. The head (articular condyle), limited in movement and exerting pressure (compression) on the temporal bone (glenoid fossa), begins to collapse. The disk is destroyed too...
Arthrosis of the TMJ.
TMJ is normal.
And this is a completely different story, and different prospects (see “Crunch in the jaw”).
Treatment in installments
The Orto-Artel clinic offers installments for the entire process of treating any disease. Personal conditions are considered on an individual basis.
Find out more
or call 8 (495) 128-11-74
So it turns out that cracks in the jaw when opening or closing the mouth are the first, initial, but very formidable symptom. Indicating a developing pathology in the TMJ. And if there are similar clicks in the jaw, the patient should definitely not “click” and slow down. And it is necessary to contact specialists as quickly as possible.
It is best if these are specialists from the Orto-Artel clinic who have specific knowledge and extensive experience in treating clicking in the jaw when opening the mouth and preventing TMJ dysfunctions.
During a direct examination by a specialist, you will be able to find out your exact diagnosis, as well as receive a referral for diagnosis or a treatment plan.
Sergei Vladimirovich Yashin
author of the article
Dentist-orthodontist, maxillofacial orthopedist
More than 7 years of experience
Directions of movement of the lower jaw
During the movement of the lower jaw, sagittal, vertical and transversal displacement of its heads occurs.
Vertical displacement is necessary to open and close the mouth. In this case, the movement, depending on the force, occurs with varying strength, which determines the degree of movement of the head.
The sagittal axis of displacement is the ability to move the lower jaw back and forth. In this case, the forward movement of the jaw and the biomechanism of the head of the articular part at the moment of movement is called the sagittal path of the joints.
Transverse is the ability of the jaw to move left or right. In this case, certain muscle groups move. For example, the direction of the masticatory apparatus to the right determines the left direction of the lateral muscles, and vice versa.
Without knowledge of how muscles and joints work, the dentist cannot regulate the normal functioning of the masticatory apparatus, which means he will not be able to manufacture and install suitable dentures and implants.
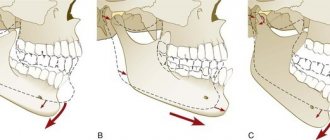
Vertical and sagittal movements of the lower jaw. Articular and incisal gliding path.
Vertical movements of the lower jaw correspond to the opening and closing of the mouth. It is typical for opening the mouth and introducing food into the mouth that at this moment the selected optimal action option is triggered, depending on the visual analysis of the nature of the food and the size of the food bolus. So, a sandwich, seeds are placed in the incisor group, fruits, meat - closer to the canine, nuts - to the premolars. Thus, when the mouth opens, a spatial displacement of the entire lower jaw occurs (Fig. 33).
Depending on the amplitude of mouth opening, one or another movement predominates. With slight opening of the mouth (whispering, quiet speech, drinking), rotation of the head around the transverse axis in the lower part of the joint predominates; with a more significant opening of the mouth (loud speech, biting food), the rotational movement is joined by the sliding of the head and disc along the slope of the articular tubercle down and forward. With maximum mouth opening, the articular discs and mandibular heads are installed on the tops of the articular tubercles. Further movement of the articular heads is delayed by the tension of the muscular and ligamentous apparatus, and again only rotational or hinge movement remains. The movement of the articular heads when opening the mouth can be observed by placing the fingers in front of the tragus of the ear or inserting them into the external auditory canal. The amplitude of mouth opening is strictly individual. On average, it is 4-5 cm. The dentition of the lower jaw describes a curve when opening the mouth, the center of which lies in the middle of the articular head (Fig. 34). Each tooth also describes a certain curve (Fig. 35).
Sagittal movements of the lower jaw. The forward movement of the mandible is carried out mainly due to bilateral contraction of the lateral pterygoid muscles and can be divided into two phases: in the first, the disc together with the head of the mandible slides along the articular surface of the tubercle, and then in the second phase a hinge movement is added around the transverse axis passing through the heads. This movement occurs simultaneously in both joints. The distance that the articular head travels is called the sagittal articular path. This path is characterized by a certain angle, which is formed by the intersection of a line that is a continuation of the sagittal articular path with the occlusal (prosthetic) plane. The latter is understood as a plane passing through the cutting edges of the first incisors of the lower jaw and the distal buccal cusps of the last molars (Fig. 36). The angle of the sagittal articular path is individual and ranges from 20 to 40°, but its average value, according to Gysi, is 33°.
This combined pattern of movement of the lower jaw is found only in humans. The magnitude of the angle depends on the inclination, the degree of development of the articular tubercle and the amount of overlap by the upper anterior teeth of the lower anterior teeth. With deep overlap, rotation of the head will predominate; with small overlap, sliding will prevail. With a direct bite, the movements will be mainly sliding. Moving the lower jaw forward with an orthognathic bite is possible if the incisors of the lower jaw come out of the overlap, that is, the lowering of the lower jaw must first occur. This movement is accompanied by sliding of the lower incisors along the palatal surface of the upper ones until direct closure, that is, until anterior occlusion. The path taken by the lower incisors is called the sagittal incisal path. When it intersects with the occlusal (prosthetic) plane, an angle is formed, which is called the angle of the sagittal incisal path (Fig. 37 and 33).
It is also strictly individual, but, according to Gysi, it is in the range of 40-50°. Since during movement the mandibular articular head slides down and forward, the back part of the lower jaw naturally moves down and forward by the amount of incisal sliding. Consequently, when lowering the lower jaw, a distance between the chewing teeth should be formed equal to the amount of incisal overlap.
11. Transversal movements of the lower jaw. The concept of working and balancing sides. Phases of chewing movements of the lower jaw.
Transverse (lateral) movements of the mandible occur as a result of unilateral contraction of the lateral pterygoid muscle. When moving to the right, the left lateral pterygoid muscle contracts, and when moving to the left, the right muscle contracts.
During the transversal movement of the lower jaw, two sides are distinguished: working and balancing.
Laterotrusion (working movement) is the movement of the lower jaw from the position of central occlusion or central ratio in the direction of the working side, in which it deviates outward from the midsagittal plane.
Working side ( laterotrusive side) – the side towards which the movement of the lower jaw is directed from the position of central occlusion or centric relation.
Mediotrusion (non-working movement) is a movement of the lower jaw in which it deviates towards the midsagittal plane.
Non-working side (balancing, mediotrusive) - the side opposite (contralateral) to the working side when performing a working movement.
On the working side, where the movement of the jaw is directed, the chewing antagonist teeth are installed with identical tubercles, and on the opposite (balancing) side - with opposite ones. On the working side, the head remains in the hole and rotates only around its vertical axis. On the balancing side, the head together with the disc slides along the surface of the articular tubercle down and forward, as well as inward, forming an angle with the original direction of the line of the sagittal articular path. This angle was first described by Bennett and is called the angle of the transversal articular path (LATERAL ARTICULAR ANGLE ( Bennett's angle ), which is 15-20° (Fig. 37). It is depicted as a projection of two straight lines onto the Frankfort horizontal line.
Rice. 38. Angle of the transversal articular path (Bennett's movement).
Transversal movements are characterized by certain changes in the position of the teeth. If you graphically depict the curves of tooth movement during alternate movement of the lower jaw to the right and left, then they intersect at an obtuse angle. The farther the tooth is from the head, the greater the angle. The most obtuse angle is formed from the intersection of curves formed by the movement of the central incisors. This angle is called GOTHIC or TRANSVERSAL (LATERAL) INCISIVE PATH ANGLE and is on average 100 - 110°. It determines the span of the incisors during lateral movements of the lower jaw (Fig. 39).
The gothic angle recording is used to determine the centric relation of the jaws and centric occlusion.
Fig.39. Transversal incisal path.
The full range of movements of the mandible can be illustrated by a diagram showing the spatial movement of the midpoint between the central lower incisors. A three-dimensional image of the trajectory of movement of this point, obtained by U. Posselt by superimposing lateral radiographs of the skull, clearly demonstrates the complexity of the movements of the lower jaw (Fig. 40).
Rice. 40. Three-dimensional image of a complex of functional movements
lower jaw according to U. Posselt.
When chewing, the lower jaw undergoes a cycle of movements accompanied by the appearance of rapid sliding contacts of the teeth on the working side. Maximum chewing forces develop in the position of central occlusion. There are four phases of chewing. In the first phase, the jaw lowers and moves forward. In the second, the jaw shifts to the side (lateral movement). In the third phase, the teeth close on the working side with like-named tubercles, and on the balancing side with opposite ones. However, there may be no contact between the teeth on the balancing side, which depends on the severity of the transversal occlusal curves. In the fourth phase, the teeth return to the position of central occlusion (Fig. 41).
Rice. 41. Cycle of chewing movements according to U. Posselt.
The shape of the chewing cycle can be different depending on the degree of overlap and inclination of the front teeth, the height of the cusps of the chewing teeth, etc. In this regard, horizontal and vertical forms of the chewing cycle are distinguished (Fig. 42). The volume of movements of the lower jaw necessary to carry out the chewing cycle is, as a rule, less than the volume of all possible movements.
a b
a - horizontal form of the chewing cycle; b - vertical form of the chewing cycle.
Rice. 42. Forms of the chewing cycle according to U. Posselt.
Gothic arc . When viewed from above, the movements of the lower jaw in the horizontal plane during its extending right and left lateral movements to the limit, the trajectory of the midpoint of the lower incisors resembles an arrowhead or an arch. The top of this arc corresponds to the position of the central relation. The sides of the arc correspond to the trajectory of rotation of the midpoint of the lower incisors around the vertical axes of the working articular heads during the right and left lateral movements of the lower jaw to the limit.
The relationship between the sagittal incisal and articular tracts and the nature of occlusion has been studied by many authors. Bonneville, based on his research, derived the laws that are the basis for the construction of anatomical aritculators.
Bonneville's triangle is the relationship between the incisal point and the right and left heads of the temporomandibular joint. This is an equilateral triangle with a side length of about 10.5 cm. It is the basis for articulators tuned to average anatomical parameters. Considering the movements of the lower jaw carried out by the muscles of the maxillofacial region, three groups of muscle movements can be distinguished:
- conscious movements - moving the lower jaw forward, consciously opening the mouth;
- reflex movements - mandibular reflex, mouth opening reflex;
- rhythmic movements - chewing, articulation.
Chewing movements are complex, they include movements of the jaws, chewing and facial muscles and tongue, and soft tissues of the face. The lips, cheeks and tongue control the position of the bolus of food in the oral cavity and its retention on the occlusal surface. The following phases of the chewing cycle are distinguished:
1. preparatory phase - formation and preparation of the food bolus for crushing.
2. grinding phase - crushing and grinding the food bolus, mixing it with saliva on the working side (laterotrusive).
3. final formation of the food bolus before swallowing - mixing of the food bolus with saliva.
In all phases of the chewing cycle, the following movements are distinguished: group and working guiding functions, canine guidance.
Working guiding function (teeth-directed lateral movement of the lower jaw from the position of central occlusion) - the lateral movement of the lower jaw from the position of central occlusion with the teeth closed is directed by the contacting surfaces of these teeth on the working side. In natural dentition, two types of working guiding function are most often found: “canine path” and “group guiding function”.
Group guiding function (unilateral protection) - contact of the buccal cusps of molars and premolars in lateral occlusion on the working sides. Occurs in 16.3% of cases.
The canine path is the sliding of the apex or distobuccal slope of the lower canine of the working side along the palatal slope of the upper canine of the working side when the muscles move the lower jaw to the working side. This causes the lower jaw to move sideways, forward, and open the mouth. During the canine-guided working movement, the central and lateral incisors of the working side can simultaneously be in movable contact with the opposing central and lateral incisors. In a canine-guided working movement, the premolars and molars on the working side are opened while the mandible moves away from the centric occlusion position. All teeth on the non-working side open during this movement. The canine tract provides the anterior guide component, and the articular tract constitutes the distal guide component and provides the opening of the teeth on the non-working side. The canine route occurs in 57%.
Canine protection - contact of the canines in lateral occlusion on the working sides.
Anterior guiding function (incisal path) - When the incisors and canines guide both the forward and working movements of the mandible, they constitute the anterior guiding component of its movements.
Group working guiding function - the working guiding function of a group of teeth is carried out by all teeth of the working side. The cutting edges of the anterior teeth of the lower jaw slide along the palatal surfaces of the anterior teeth of the upper jaw. The buccal slopes of the buccal cusps of the lower premolars and immolars slide along the palatal slopes of the buccal cusps of the upper premolars and molars.
Chewing phases:
1) the phase of grasping and cutting food, which is characterized by sliding of the cutting edges of the lower frontal teeth along the palatal surface of the upper ones until their marginal closure and back; in this phase, the forward movement of the lower jaw predominates and, therefore, the teeth are set in anterior occlusion;
2) the phase of crushing food, which is carried out by the vertical movement of the lower jaw and is characterized by maximum contact of the teeth of both jaws; occlusion of the dentition in this phase is called central and is the initial and final moment of all chewing movements of the lower jaw;
3) the phase of grinding food, which is characterized by alternating movements of the lower jaw to the sides, and when the lower jaw moves in any direction on this side, the cusps of the chewing teeth of the lower jaw will contact the cusps of the same name in the upper jaw (buccal with buccal, palatal with lingual).
TMJ functioning problems
| Click to sign up for a FREE consultation |
Disruption of the work and function of the joints and muscles of the lower jaw is called TMJ dysfunction. The pathology is caused by the occurrence of a defect in the teeth, increased wear and tear and an abnormal bite of a person.
The main clinical manifestation of dysfunction is clicking and clattering of teeth when opening the mouth. In more advanced cases, pain occurs in the ears, jaw, and painful sensations begin during chewing and yawning.
The main method for diagnosing TMJ dysfunction is radiography, which reveals dysfunction of the jaw and joint.
Treatment consists of a comprehensive effect on the condition of the jaw, which the dentist carries out based on knowledge of the biomechanics of its work.