An orthodontist makes such a diagnosis with code K07.3 according to ICD-10 (International Classification of Diseases, 10th revision) if the tooth has erupted with an inclination or displacement, or has completely appeared outside the dental arch. This mainly happens to the lower eighth molars, incisors and canines.
A companion to dystopia can be other anomalies in the position of the teeth - crowding, displaced or open bite, as well as retention.
Reasons for appearance
- Heredity. If a child inherited, for example, large teeth from his father and a small jaw from his mother, dystopia cannot be avoided. In addition, it can be inherited on its own.
- Atypical formation of dental tissue primordia in the embryo.
- Injuries and bad habits: prolonged use of a pacifier, the habit of biting a pencil, etc.
- Early removal of baby teeth.
- Peculiarities of eruption time. For example, if fangs appear late, that is, after 9 years, there may no longer be room for them in the arch.
- Dystopia is often caused by polyodontia (“extra teeth”), macrodentia (abnormally large teeth), partial absence of teeth or a sharp discrepancy between the size of primary and permanent teeth.
Types of dystopia
Depending on how and where the crown is displaced, several types of pathology are distinguished:
- A tilt towards the vestibule of the mouth means that we are talking about the vestibular position of the dystopic tooth, and if, on the contrary, in the depths of the oral cavity, we are talking about the oral position.
- When the body of the tooth is completely located outside the arch and moves forward or backward, the dentist will note in the chart the presence of a mesial or distal position, respectively.
- Is the newbie cutting higher than the rest? – Such an anomaly will be called supraposition. If lower, infra position.
- Rare anomalies are torto- and transposition. In the first case, the tooth rotates around its axis, in the second, it changes places with its neighbor, for example, a canine takes the place of a premolar.
Depending on which tooth is in the wrong position, dystopia of incisors, canines, molars and premolars or “eights” is distinguished.
Postoperative period - what to do after extraction
Above, we looked at how problem teeth are removed, and now let’s move on to the important question of how to care for the socket and oral cavity after the procedure. This period plays a very important role and requires the patient to responsibly comply with the doctor’s instructions. Otherwise, infection may seep into the wound and cause complications.
So, dental experts provide the following recommendations for oral care after a complex extraction:
- for the first 3-4 hours you will have to give up eating, drinking and smoking,
- when carrying out hygienic procedures, including with rinsing solutions prescribed by a doctor, extreme caution must be observed,
- in the first days it is better to try to chew food on the opposite side,
- preference should be given to a product that is not too hard at room temperature,
- You will have to temporarily limit physical activity, give up a hot bath, visit the bathhouse and sauna.
For the first time after removal, you should avoid exercising and eating.
It is very important to monitor the integrity of the blood clot that forms in the socket after the bleeding stops, a couple of hours after the operation. This clot serves as a protective barrier, eliminating the risk of mechanical injury to tissues or infection. Therefore, in the first couple of days, instead of rinsing, you need to do oral baths with the prescribed antiseptic solution. Too intense rinsing and anything that can create a vacuum in the mouth should be banned in the near future.
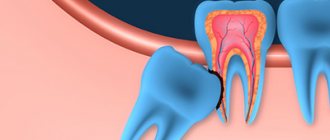
Dystopic wisdom tooth
The eighth molars are the last to appear, and that is why they are associated with the greatest risk of dystopia.
The bone tissue has already been formed, and often there is no longer room for a newcomer in the dental arch. In addition, any indigenous is preceded by a dairy pioneer who “breaks” the path. The “wise” molar does not have such an assistant, just as there are no neighboring teeth that determine the correct position on the arch.
Dystopic wisdom tooth
Possible complications
A dystopic tooth can injure the oral mucosa, tongue and cheeks, resulting in decubital ulcers.
Anomalies in the position of crowns and malocclusion are a common cause of caries: oral hygiene becomes more complicated, and it is difficult to completely remove plaque and food debris from the interdental spaces.
Another complication is problems with diction and chewing food.
Also, inflammation often occurs above the part of the crown that has not yet erupted - pericoronitis. And in the most difficult cases, the “problem” tooth erupts outside the alveolar arch, which, of course, entails not only serious discomfort, but also diseases of other organs.
ICD-10 (Dentistry)
The article presents the international classification of diseases, tenth revision, relating to the dental profile.
K00—K14 Diseases of the oral cavity, salivary glands and jaws (click on the appropriate block to expand subcategories)
K00 Disorders of development and eruption of teeth
Excluding: impacted and impacted teeth (K01)
| K00.0 | Edentia
|
| K00.1 | Supernumerary teeth
|
| K00.2 | Anomalies in the size and shape of teeth
Excluding: Carabelli tubercular anomaly, considered as a normal variant and subject to coding |
| K00.3 | Mottled teeth
Excluding: deposits (growths) on teeth (K03.6) |
| K00.4 | Tooth formation disorders
Excludes: Hutchinson's incisors and mulberry-shaped molars in congenital syphilis (A50.5), mottled teeth (K00.3) |
| K00.5 | Hereditary disorders of dental structure, not classified elsewhere
|
| K00.6 | Teething disorders
|
| K00.7 | Teething syndrome |
| K00.8 | Other dental development disorders
|
| K00.9 | Dental development disorder, unspecified
|
K01 Impacted and impacted teeth
Excluding: impacted and impacted teeth with malposition of them or adjacent teeth (K07.3)
| K01.0 | Impacted teeth An impacted tooth is a tooth that has changed its position during eruption without obstruction from an adjacent tooth. |
| K01.1 | Impact teeth An impact tooth is a tooth that has changed its position during eruption due to an obstacle from an adjacent tooth. |
K02 Dental caries
| K02.0 | Enamel caries
|
| K02.1 | Dentin caries |
| K02.2 | Cement caries |
| K02.3 | Suspended dental caries |
| K02.4 | Odontoclasia
|
| K02.8 | Other dental caries |
| K02.9 | Dental caries, unspecified |
K03 Other diseases of hard dental tissues
Excluding: bruxism, teeth grinding NOS (not otherwise specified) (F45.8), dental caries (K02)
| K03.0 | Increased tooth wear
|
| K03.1 | Grinding of teeth
|
| K03.2 | Tooth erosion
|
| K03.3 | Pathological tooth resorption
|
| K03.4 | Hypercementosis
|
| K03.5 | Ankylosis of teeth |
| K03.6 | Deposits (growths) on teeth
|
| K03.7 | Change in color of hard tissues of teeth after eruption Excluding: deposits (growths) on teeth (K03.6) |
| K03.8 | Other specified diseases of dental hard tissues
If it is necessary to identify the radiation that caused the injury, use an additional code of external causes (class XX). |
| K03.9 | Disease of hard dental tissues, unspecified |
K04 Diseases of the pulp and periapical tissues
| K04.0 | Pulpitis
|
| K04.1 | Pulp necrosis
|
| K04.2 | Pulp degeneration
|
| K04.3 | Improper formation of hard tissue in the pulp
|
| K04.4 | Acute apical periodontitis of pulpal origin
|
| K04.5 | Chronic apical periodontitis
|
| K04.6 | Periapical abscess with cavity
|
| K04.7 | Periapical abscess without cavity
|
| K04.8 | Root cyst
Excludes: periodontal lateral cyst (K09.0) |
| K04.9 | Other and unspecified diseases of the pulp and periapical tissues |
K05 Gingivitis and periodontal diseases
| K05.0 | Acute gingivitis Excludes: acute necrotizing ulcerative gingivitis (A69.1), gingivostomatitis caused by herpes simplex virus (B00.2) |
| K05.1 | Chronic gingivitis
|
| K05.2 | Acute periodontitis
Excluding:
|
| K05.3 | Chronic periodontitis
|
| K05.4 | Periodontal disease
|
| K05.5 | Other periodontal diseases |
| K05.6 | Periodontal disease, unspecified |
K06 Other changes in the gingiva and edentulous alveolar margin
Excluding: atrophy of the edentulous alveolar margin (K08.2), gingivitis: acute (K05.0), chronic, NOS (not otherwise specified) (K05.1)
| K06.0 | Gum recession
|
| K06.1 | Gingival hypertrophy
|
| K06.2 | Lesions of the gums and edentulous alveolar margin caused by trauma. If necessary, identify the cause, use an additional code for external causes (class XX) |
| K06.8 | Other specified changes in the gingiva and edentulous alveolar margin
|
| K06.9 | Changes in the gingiva and edentulous alveolar margin, unspecified |
K07 Maxillofacial anomalies (including malocclusions)
Excludes: atrophy and hypertrophy of the half of the face (Q67.4), unilateral condylar hyperplasia or hypoplasia (K10.8)
| K07.0 | Main anomalies in jaw size
Excludes: acromegaly (E22.0), Robin's syndrome (Q87.0) |
| K07.1 | Anomalies of maxillo-cranial relationships
|
| K07.2 | Anomalies of dental arch relationships
|
| K07.3 | Anomalies of teeth position
Excludes: impacted and impacted teeth with normal position (K01) |
| K07.4 | Malocclusion, unspecified |
| K07.5 | Maxillofacial anomalies of functional origin
Excludes: bruxism, teeth grinding NOS (not otherwise specified) (F45.8) |
| K07.6 | Temporomandibular joint diseases
Excludes: current case of jaw dislocation (S03.0), sprain and strain of jaw joint(s) (S03.4) |
| K07.8 | Other maxillofacial anomalies |
| K07.9 | Maxillofacial anomaly, unspecified |
K08 Other changes in teeth and their supporting apparatus
| K08.0 | Exfoliation of teeth due to systemic disorders |
| K08.1 | Loss of teeth due to accident, extraction or localized periodontal disease |
| K08.2 | Atrophy of the edentulous alveolar margin |
| K08.3 | Delayed tooth root (retentive root) |
| K08.8 | Other specified changes in teeth and their supporting apparatus
|
| K08.9 | Changes in teeth and their supporting apparatus, unspecified |
K09 Cysts of the oral region, not elsewhere classified
Including: lesions with histological features of an aneurysmal cyst and other fibro-osseous lesion Excluding: radicular cyst (K04.8)
| K09.0 | Cysts formed during the formation of teeth
|
| K09.1 | Growth (non-odontogenic) cysts of the mouth area
|
| K09.2 | Other jaw cysts
Excludes: occult bone cyst of the jaw, Stafne cyst (K10.0) |
| K09.8 | Other specified cysts of the oral area, not classified elsewhere
|
| K09.9 | Oral cyst, unspecified |
K10 Other jaw diseases
| K10.0 | Jaw development disorders
|
| K10.1 | Giant cell granuloma, central
Excludes: peripheral giant cell granuloma (K06.8) |
| K10.2 | Inflammatory diseases of the jaws
If necessary, identify the radiation that caused the injury, use an additional code of external causes (class XX) |
| K10.3 | Alveolitis of the jaws
|
| K10.8 | Other specified diseases of the jaws
|
| K10.9 | Disease of the jaw, unspecified |
K11 Diseases of the salivary glands
| K11.0 | Salivary gland atrophy |
| K11.1 | Salivary gland hypertrophy |
| K11.2 | Sialadenitis Excludes: mumps (B26), Hereford uveoparotid fever (D86.8) |
| K11.3 | Salivary gland abscess |
| K11.4 | Salivary gland fistula Ex: congenital salivary gland fistula (Q38.4) |
| K11.5 | Sialolithiasis
|
| K11.6 | Salivary gland mucocele
|
| K11.7 | Disorders of the secretion of the salivary glands
Excludes: dry mouth NOS (R68.2) |
| K11.8 | Other diseases of the salivary glands
Excludes: sicca syndrome (Sjögren's disease) (M35.0) |
| K11.9 | Salivary gland disease, unspecified
|
K12 Stomatitis and related lesions
Excluding:
- decaying mouth ulcer, gangrenous stomatitis, noma (A69.0)
- cheilitis (K13.0)
- gingivostomatitis caused by herpes simplex virus (B00.2)
| K12.0 | Recurrent oral aphthae
|
| K12.1 | Other forms of stomatitis
|
| K12.2 | Cellulitis and oral abscess
Excluding:
|
K13 Other diseases of the lips and oral mucosa
Including: changes in the epithelium of the tongue Excluding:
- some changes in the gingiva and edentulous alveolar margin (K05-K06)
- cysts of the mouth area (K09)
- tongue diseases (K14)
- stomatitis and related lesions (K12)
| K13.0 | Lip diseases
Excluding: |
| K13.1 | Biting cheeks and lips |
| K13.2 | Leukoplakia and other changes in the oral epithelium, including the tongue
Excludes: hairy leukoplakia (K13.3) |
| K13.3 | Hairy leukoplakia |
| K13.4 | Granuloma and granuloma-like lesions of the oral mucosa
|
| K13.5 | Submucosal fibrosis of the oral cavity
|
| K13.6 | Hyperplasia of the oral mucosa due to irritation Excludes: hyperplasia of the edentulous alveolar margin due to irritation (denture hyperplasia) (K06.2) |
| K13.7 | Other and unspecified lesions of the oral mucosa
|
K14 Diseases of the tongue
Excluding:
- erythroplakia, focal epithelial hyperplasia, leukedema, leukoplakia of the tongue (K13.2)
- hairy leukoplakia (K13.3)
- congenital macroglossia (Q38.2)
- submucosal fibrosis of the tongue (K13.5)
| K14.0 | Glossitis
Excludes: atrophic glossitis (K14.4) |
| K14.1 | "Geographical" language
|
| K14.2 | Median rhomboid glossitis |
| K14.3 | Hypertrophy of the tongue papillae
|
| K14.4 | Atrophy of the tongue papillae
|
| K14.5 | Folded tongue
Excludes: congenital cleft tongue (Q38.3) |
| K14.6 | Glossodynia
|
| K14.8 | Other tongue diseases
|
| K14.9 | Tongue disease, unspecified
|
Dental diseases from other sections.
| A69.0 | Necrotizing ulcerative stomatitis
|
| A69.1 | Other Vincent infections - Fusospirochetous pharyngitis - Necrotizing ulcerative (acute): • gingivitis • gingivostomatitis - Spirochetal stomatitis - Vincent's ulcerative film sore throat: • tonsillitis • gingivitis |
| B00.2 | Herpetic gingivostomatitis and pharyngotonsillitis |
| B26 | Parotitis:
|
| B37.8 | Candidiasis of other localizations Candidiasis: • cheilitis • enteritis |
| D86.8 | Sarcoidosis of other specified and combined localizations:
|
| E22.0 | Acromegaly and pituitary gigantism Excluded:
|
| E53.0 | Riboflavin deficiency
|
| F45.8 | Any other disturbances in sensation, function, and behavior that are not associated with physical disorders and that are not mediated through the autonomic nervous system are limited to specific systems or parts of the body and are closely related in time to stressful events or problems. Psychogenic:
|
| J36 | Peritonsillar abscess
Excluded:
|
| L55—L59 | Diseases of the skin and subcutaneous tissue associated with exposure to radiation
|
| M35.0 | Sicca Sjögren's syndrome Sjögren's syndrome with:
|
| Q38.2 | Macroglossia |
| Q38.3 | Other congenital abnormalities of the tongue
|
| Q38.4 | Congenital anomalies of the salivary glands and ducts:
|
| Q67.4 | Other congenital deformities of the skull, face and jaw |
| Q87.0 | Syndromes of congenital anomalies affecting primarily the appearance of the face
|
| R68.2 | Dry mouth, unspecified Excluded: decreased secretion of salivary glands (K11.7) dry mouth caused by:
|
| S03.0 | Jaw dislocation:
|
| S03.4 | Sprain and strain of the joint (ligaments) of the jaw Temporomandibular joint (ligament) |
| class XX | External causes of morbidity and mortality:
|
Treatment of dystopia
The method of therapy depends on the condition of the dystopic tooth and its useful load. Sometimes it is enough just to polish the sharp edges and give it a shape that will not injure the mucous membrane.
Most often, when a tooth is in an incorrect position, they resort to orthodontic treatment methods. Braces allow you to cope with serious malocclusions. If there is no room for a tooth, and this is, for example, a canine that is important from the point of view of functionality and aesthetics, then you will have to remove its neighbors and only then begin orthodontic treatment.
Treatment of dystopia with braces
When to remove a dystopic tooth
Removal is not a pleasant procedure, and therefore is always a last resort. It is used in the following cases:
- in the presence of pulpitis, periodontitis or cysts;
- if it is a wisdom tooth complicating the treatment of caries of the seventh molars;
- when the anomaly is accompanied by osteomyelitis or periostitis;
- if surrounding tissues are seriously injured.
If there are no such indications, the dentist will do everything possible to save the dystopic tooth. Note that it is optimal to undergo treatment before the end of growth of the facial skeleton, that is, up to 14-16 years. In this case, you will see results faster, and they will be noticeably better than if you consult a specialist later.
Find out what retention is fraught with and how to eliminate it.
Diagnostics
In most cases, pathological tooth root resorption is asymptomatic and is detected during routine radiographic examination. At the present stage, the number of detected resorptions has increased due to the introduction of cone beam computed tomography (CBCT).
In his study, K. Aziz [9] proved that a two-dimensional image often does not reflect the true nature or extent of the resorptive process.
K. Vasconcelos [67] in his report indicates that CBCT helps to determine the presence and topography of the resorptive area of the root, which determines treatment tactics.