Bends, as well as bends of such a structure as the gallbladder, are characterized by a violation of the anatomical structure of the organ with a general decrease in its functional state. The structure of the gallbladder is divided into three components: the neck, the fundus and the body itself. When filled, the properly positioned gallbladder takes on a pear-shaped shape. The bending condition leads to its deformation and partial or complete change in the correct shape of the bubble. This phenomenon is characterized as an inflection or bend of this organ. A kink in the gallbladder is common in children.
What is inflection?
Bend of the gallbladder: ultrasound
Excesses in the gallbladder are both congenital and acquired as a result of a number of environmental factors. If it is congenital, the bend can be detected completely in a newborn baby and corrected. Such natural disorders are diagnosed by computer research using an ultrasound procedure. Since children's organs are formed by interacting with each other, a change in the shape of the gallbladder will not interfere with its normal functioning and will not cause any problems. The acquired nature of excesses in the gallbladder must be treated. Most often, treatment is lengthy and labor-intensive.
Twisting resulting from any reason prevents the patient from leading a full life, due to disruption of the outflow of the bile flow and disruption of the digestive tract.
Why do kinks occur?
As mentioned earlier, this pathology can be congenital or acquired. Birth defects occur under the influence of a person’s genotype and negative factors during intrauterine development. Typically, congenital abnormalities do not cause additional discomfort to a person, and may disappear on their own in childhood. Acquired kinks in the bladder in children can occur for the following reasons:
- prolonged emotional stress in a child;
- excessive physical activity;
- severe obesity;
- violation of proper diet;
- backbreaking physical labor;
- exacerbation of chronic cholecystitis.
In childhood, there is no need to lift excessive weight, as this can provoke prolapse of internal organs and affect the appearance of kinks in the gallbladder. Acquired kinks cause discomfort and must be treated.
Gallstone disease that develops in childhood can also lead to twisting of the bladder. In this case, the gallbladder begins to sag under the influence of gravity of the formed stones and, as a result, an inevitable bend of the cervical part of the organ occurs. In case of this pathology, you should immediately seek advice from a medical institution, otherwise a violation of the outflow of bile formed in the body in most cases leads to problems in the functioning of all digestive organs.
Tongue, nose, throat: everything is interconnected
The inside of a child’s nasopharynx is covered with mucous membrane, which should normally perform a protective function: trap viruses, bacteria, dust particles and other allergens. But if the mucous membrane dries out, it becomes too thin and vulnerable.
Therefore, by the way, the child’s room should be cool and fairly humid.
If the house is hot, the air is dry, the mucous membrane of the nasopharynx dries out, and any virus can easily penetrate through the thinned protective barrier. This causes frequent acute respiratory viral infections associated with a runny nose and swelling of the nose.
Due to these diseases, the child’s nasal breathing is impaired, his mouth is constantly open and his tongue is visible. Gradually, the habit of breathing through your mouth in your sleep arises.
Breathing through your mouth during sleep is a very alarming sign
The mouth opens slightly, expanding space for the tongue. And, of course, the child's tongue begins to take up this additional space in and outside the mouth.
This is how tongue dysfunction arises, then it becomes fixed in the child’s habits.
A vicious circle arises: frequent ARVI - stuffy nose - habit of breathing through the mouth - dry mucous membrane - frequent ARVI, and in addition, tongue dysfunction occurs.
All this can lead to the proliferation of lymphoid tissue, and therefore to adenoiditis and tonsillitis, since it is the nose that filters the air, and when breathing through the mouth, allergens and viruses enter directly into the oropharynx. In this case, the blood is not fully saturated with oxygen and sleep at night is disturbed - in the morning the child gets up sleep-deprived, feels drowsy during the day and cannot concentrate on studies.
Please note: when a child sleeps with his mouth open, this is a very alarming symptom. This habit easily passes into adulthood: snoring, apnea and numerous negative consequences from this occur.
Signs of kinks
Compliance with a diet for gallstone inflection is the main condition for treatment
If there are kinks in the gallbladder, the child feels pain at the site of the twisting of the organ. Pain appears in the right side, back and shoulder blades. If, during the bend, bile enters the peritoneum, then severe abdominal pain is felt, moving to the left region. Over time, the pain may subside and then reappear. The child experiences bloating in the abdominal cavity, pain, as well as sudden changes in body temperature and abnormal bowel movements. These symptoms indicate a bend in the cervical region of the bladder.
If the deformation of the gallbladder is caused by the onset of an inflammatory process, then changes in skin color occur, causing it to acquire an earthy tint. Symptoms of pain are associated with the location of the bend. Let's consider the main areas where defects occur, as well as their symptomatic signs:
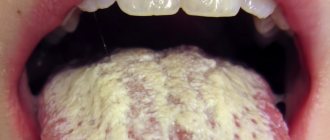
- If the bend occurs in the border area of the body and the bottom of the gallbladder, then the sick child feels pain in the abdominal region, in the collarbone, sternum and under the scapula. Attacks of nausea and vomiting are frequent, usually occurring after meals. A kind of plaque forms on the outer surface of the child’s tongue, and cracks also appear in the outer corners of the oral cavity. This type of pathology most often occurs in childhood.
- If twisting of the gallbladder occurs in its cervical region, then the most common manifestations of pain in the left hypochondrium, accompanied by nausea and increased gas formation, become apparent.
- There are times when the patient even develops a feverish state. A bend in the neck is the most dangerous and life-threatening, since it is possible for the resulting bile to penetrate into the abdominal cavity, accompanied by the formation of peritonitis in the body.
- If a combined type of inflection is observed, which represents numerous deformations of the gallbladder in its different areas, then the patient experiences severe abdominal pain. Sometimes meals are accompanied by nausea and a gag reflex.
Dysarthric speech disorders in children of early and preschool age
Dysarthria (speech motor disorder) is a violation of the pronunciation aspect of speech caused by insufficient innervation of the speech muscles. Dysarthria is a consequence of organic damage to the central nervous system, in which the motor mechanism of speech is disrupted. With dysarthria, it is not the programming of speech utterance that is impaired, but the motor implementation of speech. The leading defects in dysarthria are disturbances in the sound-pronunciation aspect of speech and prosody, as well as disturbances in speech breathing, voice and articulatory motor skills.
Speech intelligibility in dysarthria is impaired, speech is blurred and unclear. Main disorders (structure of the defect) in dysarthria
Impaired tone of articulatory muscles (facial muscles, tongue, lips, soft palate) such as spasticity, hypotension or dystonia. 1. Spasticity - increased tone in the muscles of the tongue, lips, face and neck. With spasticity, the muscles are tense. The tongue is pulled back “lumpy”, its back is spastically curved, raised upward, the tip of the tongue is not pronounced. The tense back of the tongue raised towards the hard palate helps soften consonant sounds (palatalization). Sometimes the spastic tongue is pulled forward with a “sting.” An increase in muscle tone in the orbicularis oris muscle leads to spastic tension of the lips, tightly closing the mouth (voluntarily opening the mouth is difficult). In some cases, with a spastic condition of the upper lip, the mouth may, on the contrary, be slightly open. In this case, increased salivation (hypersalivation) is usually observed. Active movements with spasticity of the articulatory muscles are limited. (Muscle spasticity is noted with spastic-paretic dysarthria.) 2. Hypotonia - decreased muscle tone. With hypotonia, the tongue is thin, spread out in the oral cavity; lips are flaccid and cannot close tightly. Because of this, the mouth is usually half-open, and hypersalivation may be expressed. Hypotonia of the muscles of the soft palate prevents the velum from moving sufficiently upward and pressing it against the back wall of the pharynx; a stream of air exits through the nose. In this case, the voice acquires a nasal tint (nasalization). (Hypotonia of articulatory muscles occurs with spastic-paretic and ataxic dysarthria.) 3. Dystonia is a changing nature of muscle tone. At rest, low muscle tone may be noted; when attempting to speak and at the moment of speech, the tone increases sharply. Dystonia significantly distorts articulation. A characteristic feature of sound pronunciation in dystonia is the inconstancy of distortions, substitutions and omissions of sounds. (Dystonia is noted with hyperkinetic dysarthria.)
In children with neurological pathology, a mixed and variable nature of tone disturbances in the articulatory muscles (as well as in the skeletal muscles) is often noted, i.e. in individual articulatory muscles, tone can change differently. For example, spasticity may be observed in the lingual muscles, and hypotonia in the facial and labial muscles. In all cases, there is a certain correspondence between tone disturbances in the articulatory and skeletal muscles. Impaired mobility of articulatory muscles. Limited mobility of the muscles of the articulatory apparatus is the main manifestation of paresis of these muscles.
Insufficient mobility of the articulatory muscles of the tongue and lips causes disturbances in sound pronunciation. When the lip muscles are damaged, the pronunciation of both vowels and consonants suffers. Articulation in general is impaired. Sound pronunciation is especially severely impaired when the mobility of the tongue muscles is sharply limited. The degree of impairment of the mobility of articulatory muscles can be different - from complete impossibility to a slight decrease in the volume and amplitude of articulatory movements of the tongue and lips. In this case, the most subtle and differentiated movements are disrupted first (primarily raising the tongue upward).
Specific violations of sound pronunciation : - persistent nature of violations of sound pronunciation, particular difficulty in overcoming them; - specific difficulties in automating sounds (the automation process requires more time than with dyslalia). If speech therapy classes are not completed on time, acquired speech skills often disintegrate; - the pronunciation of not only consonants, but also vowels is impaired (average or reduced vowels); - the predominance of interdental and lateral pronunciation of whistling [s], [z], [ts] and hissing [sh], [zh], [h], [sch] sounds; - deafening of voiced consonants (voiced sounds are pronounced with insufficient participation of the voice; - softening of hard consonant sounds (palatalization); - disturbances in sound pronunciation are especially pronounced in the speech stream. With an increase in speech load, general blurriness of speech is observed and sometimes increases.
Depending on the type of violation, all sound pronunciation defects in dysarthria are divided into two categories: anthropophonic (sound distortions) and phonological (substitutions, confusions). In dysarthric disorder, the most typical violation of the sound structure of speech is sound distortion.
Speech breathing disorders . Breathing disorders in children with dysarthria are caused by insufficient central regulation of breathing. Insufficient depth of breathing. The rhythm of breathing is disturbed: at the moment of speech it becomes more frequent. There is a violation of the coordination of inhalation and exhalation (shallow inhalation and shortened weak exhalation). Exhalation often occurs through the nose, despite the half-open mouth. Respiratory disorders are especially pronounced in the hyperkinetic form of dysarthria.
Voice disorders . Voice disorders are caused by changes in muscle tone and limited mobility of the muscles of the larynx, soft palate, vocal folds, tongue and lips. The most common symptoms are insufficient voice strength (quiet, weak, fading) and deviations in voice timbre (dull, nasal, constricted, hoarse, intermittent, tense, guttural).
In various forms of dysarthria, voice disturbances are of a specific nature. Violations of prosody (melodic-intonation and tempo-rhythmic characteristics of speech). Melody-intonation disorders are often considered one of the most persistent signs of dysarthria. They greatly influence the intelligibility and emotional expressiveness of speech. There is a weak expression or absence of vocal modulations (the child cannot voluntarily change the pitch). The voice becomes monotonous, poorly or unmodulated.
Violations of speech tempo are manifested in its slowing down, less often - in acceleration. Sometimes there are disturbances in the rhythm of speech (for example, chant - “chopped” speech, when there is an additional number of stresses in words).
Lack of kinesthetic sensations in the articulatory apparatus. In children with dysarthria, there is not only a limitation in the range of articulatory movements, but also a weakness in the kinesthetic sensations of articulatory postures and movements.
Autonomic disorders. One of the most common autonomic disorders in dysarthria is hypersalivation. Increased salivation is associated with limited movements of the tongue muscles, impaired voluntary swallowing, and paresis of the labial muscles. It is often aggravated due to the weakness of kinesthetic sensations in the articulatory apparatus (the child does not feel the flow of saliva) and decreased self-control.
Hypersalivation can be expressed to varying degrees. It can be constant or intensify under certain conditions. Even mild hypersalivation (moistening of the corners of the lips during speech, slight leakage of saliva) indicates the presence of neurological symptoms in the child. Less common are vegetative disorders such as redness or pallor of the skin, increased sweating during speech.
Violation of the act of receiving food. Children with dysarthria often have difficulty, and in severe cases, no chewing of solid food or biting off a piece. Choking and choking when swallowing are often observed. Difficulty drinking from a cup. Sometimes coordination between breathing and swallowing is impaired.
The presence of synkinesis. Synkinesias are involuntary accompanying movements when performing voluntary articulatory movements (for example, additional upward movement of the lower jaw and lower lip when trying to raise the tip of the tongue). Oral synkinesis - opening of the mouth during any voluntary movement or when attempting to perform it. Increased pharyngeal (gag) reflex. Loss of coordination of movements (ataxia).
Ataxia manifests itself in dysmetric, asynergic disorders and in the scantiness of the rhythm of speech. Dysmetria is a disproportion, inaccuracy of voluntary articulatory movements. It is most often expressed in the form of hypermetry, when the desired movement is realized in a more sweeping, exaggerated, slower movement than necessary (excessive increase in motor amplitude). Sometimes there is a lack of coordination between breathing, voice production and articulation (asynergia). Ataxia is noted with ataxic dysarthria.
The presence of violent movements (hyperkinesis and tremor) in the articulatory muscles. Hyperkinesis - involuntary, irregular, violent; There may be pretentious movements of the muscles of the tongue and face (hyperkinetic dysarthria). Tremor - trembling of the tip of the tongue (most pronounced during targeted movements). Tremor of the tongue is observed with ataxic dysarthria.
From the book Prikhodko O. G. “Speech therapy massage for the correction of dysarthric speech disorders in children of early and preschool age.
Treatment options
The inflection of the bile duct does not go away asymptomatically
Treatment of defects formed in the structure of the bile reservoir is carried out mainly by conservative methods. The doctor must prescribe to the patient special medications that have a predominant choleretic effect in the body, as well as various types of antispasmodics that prevent excessive accumulation of bile in the body. Physiotherapeutic methods are also widely used. Special procedures prescribed by the attending physician are aimed at improving blood flow to the organ and restoring the activity of all existing muscles, as well as promoting their normal functioning.
In many cases, the child is prescribed to visit sanatoriums and resorts in order to increase the effectiveness of treatment.
The sick child is prescribed a special diet. Usually, high-fat, fried, and spicy foods are excluded from the daily menu. There is no need to pamper your child with an abundance of sweets and confectionery. Also, do not overuse flour products and various baked goods.
Stopping blood circulation and breathing
Call an ambulance (resuscitation) immediately!
- Ensuring airway patency:
- if a cervical spine injury is suspected, the neck is immobilized
- clean the oropharynx (pear, finger)
- eliminate obstruction caused by retraction of the tongue or compression by soft tissues of the neck, push the lower jaw forward or raise the chin.
- improving airway patency. The head is positioned along the midline. Children, unlike adults, should not throw their heads back too much, because in children this can lead to airway obstruction. A towel folded several times is placed under the back of the head (for adults, a cushion under the shoulders).
- Ventilation is started using the mouth-to-mouth method (mouth to mouth and nose) and indirect chest massage. The effectiveness of ventilation is assessed by chest excursion.
Ventilation is performed so that each breath lasts 1.0-1.5 s. The frequency of compressions on the chest of a newborn is at least 120 per minute, the ratio of the frequency of insufflations and compressions is 1:3. In older children, the frequency of pressure is at least 100 per minute. The child is placed on a hard surface and chest compressions are immediately started. The ratio of the frequency of inflation to the frequency of chest compressions is 1:5.
In infants, indirect massage is carried out in two ways: pressing on the chest with the middle and index fingers of one hand, or clasping the child with both hands so that the thumbs are located on the middle third of the sternum, and the rest support the back.
In both cases, pressure is applied to the lower third of the sternum (about a finger's width below the nipples). In children 1-2 years old, I press on the sternum with the protrusion of the palm of one hand. Older children and adults use two hands. In both cases, pressure is applied to the lower third of the sternum (approximately two finger widths above the xiphoid process). Depth of descent of the sternum: children under one year old: 1.5-2.5 cm, up to 7-8 years old - 3-5 cm, older - 4-6 cm. The effectiveness of indirect massage is assessed by the pulse in the carotid and femoral arteries. Resuscitation measures must be continued until doctors arrive!