Modern terms of formation of temporary and permanent occlusion in children
Teething has a significant impact on the formation of a child’s body and is an indicator of the child’s overall development. With the eruption of primary teeth, the process of eating is transformed: the sucking reflex fades, the mechanism of the act of swallowing changes, and the chewing function begins to form. Developing active chewing promotes jaw growth and changes in the proportions of the brain and facial skull.
Speech development is activated—correct articulation and sound production become possible, which is an integral part of social adaptation and stimulation of the child’s mental development. The physiological norm for the eruption of teeth in the primary dentition can be established based on a number of criteria, such as certain timing, pairing and sequence of eruption [7, 13, 18].
The delay in the eruption of primary teeth, according to domestic and foreign literature, may be due to prematurity, the negative influence of the pathology of the neonatal and postnatal periods of child development [10, 25, 31, 35, 36].
A number of authors note the negative impact of rickets on the physiological course of the eruption of primary teeth. According to N.I. Agapov (1953), the consequences of rickets affect the condition of the upper and lower jaws differently, which contributes to the disruption of the sequence and pairing of the eruption of primary teeth [1]. L.V. Ilyina-Markosyan (1961), in a histological study of the microstructure of the jaw bones in rickets, concluded that the delay in eruption can be explained by a violation of the bone structure of the jaws. These disorders manifest themselves as deposition of osteoid tissue along the periphery of the bone beams, and in some areas as more extensive accumulations of osteoid, which is slowly resorbed. The author believed that the violation of the eruption sequence was due to delayed growth of the lower jaw. As a result, temporary teeth first erupt on the upper jaw, and only then on the lower jaw. Rickets suffered during the first year of a child’s life has a pronounced effect on the timing of the eruption of primary teeth and leads to their delay by 4-5 months. compared to healthy children. In the group of children with rickets, all signs of physiological eruption of primary teeth were disrupted: timing, pairing and sequence [12]. In addition, the timing of the eruption of primary teeth is directly influenced by the type of feeding in infancy and the characteristics of the introduction of subsequent complementary foods, which shape the nature of the chewing load in the future. Early eruption of primary teeth was noted in breastfed children, in comparison with the group of children on artificial and mixed feeding [7].
Dysfunction of the endocrine glands has a negative impact on the formation of the dentofacial apparatus and, in particular, on the process of teething. Thus, with hypothyroidism and hypoparathyroidism, there is a discrepancy between the stage of formation of teeth, jaw bones and the age of the child. Clinically, there is a delay in the eruption of temporary teeth by 1-3 years, the period of their replacement with permanent teeth is delayed by 3-4 years [4, 17, 23]. Osteoporosis and deformations of the jaw bones, adentia, enamel hypoplasia, atypical shapes of tooth crowns and a decrease in their size are observed [17, 21]. With hyperthyroidism, along with changes in the morphological structure of the teeth, dentition and jaws, the work of the masticatory muscles and tongue muscles is disrupted, which together leads to impaired closure of the dentition and earlier teething [23].
In the modern generation of healthy children, the eruption of primary teeth is observed earlier than the generally accepted period, by an average of 1-2 months, which is associated with the urbanization of the population and the global acceleration of human development. The consequence of early eruption of primary teeth in children is the high intensity of the carious process due to insufficient mineralization of hard dental tissues [10, 11].
Knowledge of the timing and patterns of eruption of primary teeth, taking into account the significant role of this process in the formation of the child’s body, can be a diagnostic and prognostic sign of a number of diseases, a criterion for choosing the quality and quantity of complementary foods during the child’s transition to solid food, and a basis for determining the timing of preventive and therapeutic manipulations in dentistry and speech therapy. Nevertheless, the information provided about the timing of the eruption of primary teeth in the domestic reference, educational and scientific literature is contradictory (Table No. 1), which is due to the climatic and geographical zones of the research. In the territory of the Krasnoyarsk Territory and Krasnoyarsk, such studies were of a single, episodic nature [24].
Table No. 1. Timing of eruption of primary teeth according to various authors
Author / year | Timing of teething, months. | |||||||||
51 | 61 | 52 | 62 | 53 | 63 | 54 | 64 | 55 | 65 | |
81 | 71 | 82 | 72 | 83 | 73 | 84 | 74 | 85 | 75 | |
| V. Shpaltegolts (1909) | 7–8 | 8–12 | 16–20 | 12–16 | 20–30 | |||||
| D. A. Kalvelis (1965) | 6–8 | 8–12 | 16–20 | 12–16 | 20–30 | |||||
| V. Yu. Kurlyandsky (1970) | 6–7,5 | 7–9 | 16–18 | 12–14 | 20–24 | |||||
| A. A. Kolesov (1991) | 6–8 | 8–12 | 16–20 | 12–16 | 20–30 | |||||
| L. S. Persin (1984, 1999, 2006) | 6–8 | 8–12 | 16–20 | 12–16 | 20–30 | |||||
| V. L. Bykov (1998) | 6–8 | 8–12 | 14–20 | 12–16 | 20–30 | |||||
| M. R. Sapin and Z. G. Bryksina (2000) | 6–8 | 7–9 | 16–20 | 12–15 | 20–24 | |||||
| R. E. McDonald and D. R. Avery (2003) | 6–7,5 | 7–9 | 16–18 | 12–14 | 20–24 | |||||
| C. V. Gaivorovsky (2003) | 6–8 | 8–12 | 18–20 | 12–15 | 20–24 | |||||
| M. P. Vodolatsky (2004) | 6–8 | 8–12 | 16–20 | 12–16 | 20–30 | |||||
| O. E. Tkachuk (2006) | 6–12 | 6–12 | 24 | 18 | 30–36 | |||||
| L. L. Kolesnikova and S. S. Mikhailova (2006) | 6–7,5 | 7–9 | 16–18 | 12–14 | 20–24 | |||||
| E. Yu. Simanovskaya (2007) | 6–8 | 7–12 | 16–20 | 12–16 | 20–30 | |||||
| M. G. Prives and N. K. Vasenkov (2009) | 6–8 | 7–9 | 10–20 | 12–15 | 20–24 | |||||
The timing of the eruption of permanent teeth during the physiological development of the child coincides with the timing of complete resorption of the roots of temporary teeth. These processes are associated with the growth and development of the human dentofacial apparatus. Information about the age-related characteristics of the eruption of permanent teeth allows one to judge the general level of physical development and the state of health of the child’s body [26].
R. Almonaitiene, I. Balciuniene and J. Tutkuviene (2010) conducted a detailed analysis of the factors influencing the process of permanent dentition formation. The authors note a more significant relationship between the timing of the eruption of permanent teeth and systemic diseases; genetic factors, gender, constitutional characteristics and socio-economic factors are considered less significant [32]. A. Must et al. (2012), as a result of a long-term survey of US schoolchildren, conclude that there is a relationship between lipid metabolism disorders and the processes of sexual development in children based on the stimulating effect they identified of obesity on the eruption of permanent teeth and the rate of formation of permanent dentition [34]. A paradoxical pattern was revealed by V. Harila-Kaera, T. Heikkinen and L. Alvesalo (2003) when studying the relationship between the timing of the eruption of permanent teeth and the degree of prematurity in children. The results of their study revealed significantly (P<0.05) earlier timing of eruption of the first permanent molars and incisors in the group of children born preterm. This fact leads the authors to believe that the process of eruption of those teeth occurs at an earlier stage, the histogenesis and the beginning of mineralization of which occur in the difficult perinatal period, under the influence of various systemic factors and the phenomenon of catch-up growth [33]. Recently, a few studies have been carried out (mainly within the framework of anthropology) concerning the biological age of a person [5, 27]. For preschool and primary school age, the most informative criteria of biological development are the timing of the eruption of permanent teeth and the dynamics of increasing the height of the clinical crown. The indicator of dental maturity, along with skeletal maturity, more accurately reflects the process of physiological maturation of the body than chronological age. A close relationship has been found between the processes of ossification of the skeleton and teething. At the same time, observation of dental eruption is a non-invasive and economically more feasible procedure in comparison with the x-ray method of examination, which allows identifying many markers of general developmental disorders [14, 26].
The reference, educational, methodological and scientific literature provides conflicting information about the timing of the eruption of permanent teeth (Table No. 2). The reason for this is the peculiarities of the course of this physiological process depending on the climatic and geographical conditions in the research areas [14].
Table No. 2. Timing of eruption of permanent teeth according to various authors
Author / year | Timing of teething, years | |||||||||||||
11 | 21 | 12 | 22 | 13 | 23 | 14 | 24 | 15 | 25 | 16 | 26 | 17 | 27 | |
41 | 31 | 42 | 32 | 43 | 33 | 44 | 34 | 45 | 35 | 46 | 36 | 47 | 37 | |
| D. A. Kalvelis (1965) | 6 –9 | 7 –10 | 9 –14 | 9 –13 | 10 –14 | 5 –8 | 11 –14 | |||||||
| V. Yu. Kurlyandsky (1970) | 6 –8 | 7 –9 | 9 –12 | 10 –12 | 10 –12 | 6 –7 | 11 –13 | |||||||
| T. F. Vinogradova (1982) | 5 –6 | 7 –9 | 12 –13 | 9 –11 | 9 –11 | 4,5 –7 | 12 –13 | |||||||
| L. S. Persin (1984, 1999) | 7 –8 | 8 –9 | 10 –12 | 9 –11 | 11 –13 | 6 –7 | 12 –13 | |||||||
| A. A. Kolesov (1985, 1991) | 6 –8 | 8 –9 | 9 –11 | 9 –10 | 11 –12 | 6 | 12 –13 | |||||||
| T. V. Sharova and G. I. Rogozhnikov (1991) | 7 –7,5 | 8 –9 | 10 –13 | 9 –11 | 12 –14 | 6 –6,5 | 11 –13 | |||||||
| V. L. Bykov (1998) | 7 –8 | 8–9 | 12–13 | 9–11 | 11–12 | 6–7 | 12–13 | |||||||
| M. R. Sapin and Z. G. Bryksina (2000) | 6 –8 | 7–9 | 9–12 | 10–12 | 10–12 | 6–7 | 11–13 | |||||||
| V. G. Khatskevich and I. A. Bogomolova (2002, 2004) | 6–9 | 6–10 | 7–13 | 7–13 | 7–14 | 6–8 | 8–15 | |||||||
| M. R. Sapin and G. L. Bilich (2001, 2008) | 7–8 | 9–10 | 11–12 | 9–10 | 9–11 | 6–7,5 | 11–12 | |||||||
| N. A. Matveeva (2002, 2007) | 6 | 7–8 | 11 | 10 | 11 | 6 | 12–13 | |||||||
| P. A. Zhelezny (2003) | 4,5–7 | 5–8 | 7–12 | 7–12 | 9–12,5 | 4,5–7 | 8–13 | |||||||
| M. P. Vodolatsky (2004) | 6–8 | 8–9 | 10–11 | 9–10 | 11–12 | 6–8 | 12–13 | |||||||
| O. E. Tkachuk (2006) | 7 | 8 | 10 | 9 | 11 | 6 | 12 | |||||||
| L. S. Persin and V. M. Elizarova (2006) | 6–8 | 8–9 | 9–10 | 11–12 | 11–12 | 6 | 12–13 | |||||||
| L. L. Kolesnikova and S. S. Mikhailova (2006) | 6–8 | 7–9 | 9–12 | 9–11 | 11–12 | 5–8 | 11–13 | |||||||
| E. N. Polosukhina (2007) | 6–7 | 7,5 | 10 | 10 | 11 | 6 | 12 | |||||||
| E. Yu. Simanovskaya (2007) | 7–8 | 8–9 | 10–13 | 9–10 | 11–12 | 5–6 | 12–13 | |||||||
| M. G. Gain and N. K. Vasenkov (2009) | 8 | 9 | 11–13 | 10 | 11–15 | 6–7 | 13–16 | |||||||
A few publications provide a more detailed analysis of the timing of the eruption of upper and lower permanent teeth depending on the sex of the child. At the same time, earlier eruption of permanent teeth in girls is noted [3, 10]. However, these data were obtained in different years when analyzing different populations of children in the CIS countries with different ethnic composition and living standards. In Russia, studies, the results of which formed the basis for determining the rate of eruption of permanent teeth, were conducted in the southern and central regions of the country, while similar data in Siberia and the Far East were not taken into account.
N. G. Rusina (2000) studied in the Krasnoyarsk Territory the anthropogenic features of the change of temporary teeth, the order and timing of the eruption of permanent teeth in children [23]. At the same time, over the past years, the structure and composition of the population in this territory has changed due to significant migration activity, the technogenic impact on nature has increased, and the climatic conditions of living have changed.
Thus, the need to use more precise timing for the eruption of primary and permanent teeth in children is currently being determined.
Materials and research methods
In order to establish the actual timing of the eruption of temporary and permanent teeth in children and adolescents in modern conditions, a dental examination of 1447 apparently healthy children aged 5 to 28 months was carried out. and 1058 apparently healthy children aged 4 to 13 years. The subjects were divided into groups according to gender and age with a range of 1 month. and 1 year respectively. To ensure the representativeness of the study results, the number of observations in each age and sex group was at least 30 people. Additionally, 267 schoolchildren underwent dynamic observation of the rate of increase in the height of the clinical crown of permanent dentition teeth.
Dental examinations of children were carried out by random sampling in outpatient clinics, preschool and school educational institutions of Krasnoyarsk.
The physiological norm of teeth eruption of temporary and permanent dentition was determined based on a number of criteria, such as certain timing, pairing and sequence of eruption. To establish the timing of tooth eruption, the following provisions were used in the literature: 1) the beginning of eruption was considered the moment of perforation of the alveolar gum by a tooth with exposure of one cusp or incisal edge [20]; 2) the average age of tooth eruption is considered to be the age when 50% of those examined have this tooth [2].
However, in view of individual differences in the rates of growth and development of modern children, in our opinion, it is more rational to designate the age ranges in which the eruption of certain teeth occurs. In this case, the initial boundary of the teething interval is the age at which 5% of the studied children have a given erupted tooth, and the end is the age when 95% of the examined children have this tooth [2].
As a result of the study, it was revealed that the order and timing of the eruption of primary teeth on the right and left are the same, which confirms the position of symmetrical eruption.
Based on a certain frequency of eruption of primary teeth in age and sex groups, the timing of eruption of primary teeth in children in Krasnoyarsk was calculated in the form of age ranges, which are presented in Table No. 3.
Table No. 3. Age ranges for the eruption of primary teeth in children in Krasnoyarsk
Jaw | Floor | Timing of teeth eruption of temporary occlusion (age, months) | |||||||||
51 | 61 | 52 | 62 | 53 | 63 | 54 | 64 | 55 | 65 | ||
81 | 71 | 82 | 72 | 83 | 73 | 84 | 74 | 85 | 75 | ||
| top | boys | 7–11 | 7–13 | 15–22 | 11–17 | 20–27 | |||||
| girls | 6–9 | 7–12 | 14–21 | 11–16 | 19–27 | ||||||
| lower | boys | 6–9 | 8–13 | 15–22 | 12–17 | 19–26 | |||||
| girls | 5–8 | 8–13 | 15–21 | 12–16 | 19–26 | ||||||
From the data presented in Table No. 3, it follows that there are gender differences in the timing of the eruption of primary teeth, characterized by a tendency for earlier eruption in girls (on average by 1 month), as well as differences in the order of appearance of teeth on the upper and lower jaws, which are mosaic character.
The following sequence of eruption of primary teeth was noted: teeth 71 and 81 erupt first, then 51 and 61; 52 and 62; 72 and 82; 54 and 64; 74 and 84; 53, 63 and 73, 83; 75 and 85; 55 and 65.
The indicated timing of the eruption of temporary teeth has features in comparison with the information in the domestic literature - the beginning of the eruption of temporary teeth occurs at an earlier age, in contrast to the data given in classical textbooks (Table No. 1).
At the same time, in comparison with the results of modern studies conducted in the central territories of Russia [10], a later start of eruption of primary teeth was noted in children in Krasnoyarsk. Data characterizing the process of teeth eruption in permanent dentition indicated a symmetrical, pairwise eruption of permanent teeth in children. A certain frequency of eruption of permanent teeth made it possible to calculate the average time for the eruption of permanent teeth in children in Krasnoyarsk in the form of age ranges, which are presented in Table No. 4.
Table No. 4. Age ranges for the eruption of permanent teeth in children in Krasnoyarsk
top | boys | 5–8 | 7–9 | 9–13 | 7–11 | 8–12 | 4–7 | 10–13 |
girls | 5–8 | 6–9 | 9–12 | 7–11 | 8–12 | 4–7 | 10–13 | |
lower | boys | 4–7 | 5–8 | 8–12 | 8–11 | 8–12 | 4–7 | 10–13 |
girls | 4–7 | 5–8 | 8–11 | 8–11 | 8–12 | 4–7 | 9–13 |
From the data presented in Table No. 4, it is clear that there were differences in the sequence of teeth eruption on the lower and upper jaws. So, on the lower jaw, teeth 31, 41 and 36, 46 erupt simultaneously, and on the upper jaw in children, the eruption of permanent teeth begins with teeth 16, 26. In addition, on the lower jaw the canines erupted after the first premolars, and on the upper jaw - after the second premolars. The following sequence of eruption of permanent teeth on the upper jaw is noted: teeth 16 and 26 erupt first, then 11 and 21; 12 and 22; 14 and 24; 15 and 25; 13 and 23; 17 and 27. On the lower jaw, a similar physiological process looked like this: 36, 46 and 31, 41; 32 and 42; 34 and 44; 33 and 43; 35 and 45; 37 and 47. The presented results regarding the sequence of eruption of permanent teeth are consistent with the data of L. B. Leporskaya and E. V. Udovitskaya (1978) [16]. Gender differences were noted in the timing of the eruption of permanent teeth, which are characterized by the fact that girls showed a tendency towards earlier eruption, on average by 6-12 months. The results of dynamic observation of the increase in the height of the clinical crown showed that the period of eruption of each tooth to correspond to the height of the clinical crown height of the anatomical crown takes a long period of time. For central incisors and first molars it was 2.5 years, for lateral incisors - 3 years, for canines, premolars and second molars - 4 years. The data obtained do not agree with the results of a study published by E. I. Goncharova (1976), who determined longer time periods of 1.5 or more years [8]. The intensity of teething in girls is significantly higher than in boys. The results obtained regarding the timing of the eruption of permanent teeth differ from the data given in modern domestic literature, determining regional characteristics and consisting in an earlier formation of permanent dentition by an average of 12 months. Thus, the age-sex and regional characteristics of the eruption of primary teeth consist in the relatively early formation of a temporary occlusion in children in Krasnoyarsk and the advance in the timing of the eruption of primary teeth in girls. These circumstances justify the need to revise organizational technologies for the implementation of caries prevention programs in primary teeth at an earlier date due to insufficient mineralization of their hard tissues.
The study of age-sex and regional characteristics of the eruption of permanent teeth showed a relatively early formation of permanent occlusion in children in Krasnoyarsk and an advance in the timing of the eruption of permanent teeth in girls. These circumstances must be taken into account when determining the biological maturity and general development of the child, to develop age criteria for justifying the feasibility of preventive dental prosthetics in the case of early removal of temporary teeth, during upcoming orthodontic treatment and predicting its results, as well as when planning and implementing schemes and measures of existing prevention programs main dental diseases among the child population.
Literature
- Agapov N. I. Clinical dentistry of children / N. I. Agapov. - M.: Medicine, 1953. - 258 p.
- V. Belyakov Yu. A. Dentofacial system in endocrine diseases / Yu. A. Belyakov. - M.: Medicine, 1983. - 208 p.
- Bogomolova E. S. Modern trends in the growth and development of schoolchildren in Nizhny Novgorod / E. S. Bogomolova, N. A. Matveeva, A. V. Leonov // Almanac “New Research”. - M., 2004. - No. 2. - P. 85-86.
- Bykov V. L. Histology and embryology of human oral cavity organs (2nd ed., revised) / V. L. Bykov. - SPb.: Special. lit., 1998. - 247 p.
A complete list of references is in the editorial office.
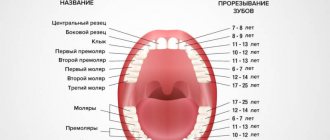
What are baby teeth and how do they erupt?
Temporary teeth are colloquially called baby teeth because they begin to appear when the baby is still breastfed. The rudiments of dental elements are formed during intrauterine development (6–8 weeks of pregnancy). Eruption is the process of teeth emerging onto the gum surface. Mechanism: the tooth root develops, over time it begins to rest against the hard bone tissue of the bottom of the alveoli, pushing the crown part of the tooth onto the surface of the gum. In total, 20 elements appear in the primary occlusion, 10 on each jaw.
Symptoms by which you can determine that your baby is cutting his first teeth
As a rule, an event such as teething does not go unnoticed by parents, as it is accompanied by many symptoms, including pain and severe itching of the gums in the place where the tooth cuts. Due to this, the child may even refuse to eat. In addition, body temperature may increase (but no more than 38° and no longer than 3 days), stools may change (become more liquid, but not to the consistency of water), salivation will increase, and sleep will be disturbed. 3 – 5 days before the tooth appears, the gums swell a little and turn red. After the tooth appears on the surface, all symptoms subside.