1002
In devices for expanding the upper dentition, screws and springs are used as power elements. The first is usually the Hyrex screw.
The latter have different designs depending on the tasks facing the orthodontist. Maxillary expanders typically use a pin, pear, or Coffin spring.
In mandibular appliances – the Koller design.
Indications for expanding the dentition
If the patient does not have the normal width of the dentition, then with the development of a crossbite, an expander is placed. Expansion is prescribed if the anomaly involves several teeth. Also, surgery will be required for mesial occlusion with a grade 3 slope according to Engle, with micrognathia and protrusion of the incisors.
The use of a device for jaw expansion is a gentle and correct method. Used to correct mixed or permanent dentition. There is a slight impact on the dentition. Therefore, the method can be applied to a child.
Reduced dentition is considered a common disease; it has different clinical manifestations. To treat anomalies, professionals use various installations. For example, a device for breaking the palatal suture is popular. For each indication, special methods have been developed that differ in the mechanism of action. Doctors often combine several methods at the same time.
Varieties
As already noted, the Coffin design can be double-circuit (two wires run parallel to each other) and single-circuit (consists of one wire). Naturally, the double-circuit element creates greater force and is used if there is a need for it.
In addition to the number of circuits, Coffin's designs differ in their relative position. The following options are possible:
- 1st. The open part of a single-circuit or double-circuit element is directed forward. In this case, the jaw will expand in the area of the fangs.
- 2nd. The open part of a single-circuit or double-circuit product is directed backwards. Expansion will occur in the premolar/molar area.
- 3rd. One spring is directed with its open part mesially, the second - distally. Moreover, the products are located closed part to each other, without overlapping one another. This arrangement ensures uniform expansion of the jaw in the distal and anterior segments.
- 4th. A variation of the 3rd option, only the springs overlap and are intertwined with each other. The nature of the action is the same as in the 3rd option, only the products are larger in size and, as a result, are able to move the dentition apart to a greater distance
- 5th. Three single, small-sized springs are located at an angle of 120° degrees with closed parts to each other. The ends of 2 of them are directed towards the fangs, the ends of the third are directed back. This arrangement allows you to simultaneously expand and lengthen the dentition.
Derichsweiler apparatus
The design is a mechanism that consists of main rings and corrective arcs. The support rings are fixed on the back teeth, where there is an attached lock on which the arches are attached.
They converge near the palatal arch, where the activator is located. This is a screw that transmits systematic pressure to the palate. The palatal suture expands, resulting in the jaw becoming wider. The gap that is formed when the palate opens is filled after some time with other soft tissue.
The device is prescribed for narrowing of the jaw arch during the first mixed bite. If the disease has formed in the permanent dentition, then the unit will have the least result, because it cannot cope with the hardened palatal suture. The device has its advantages:
- The dental expander has a plastic effect during correction, and there is no discomfort while wearing.
- The device cannot be removed independently, so correction is carried out in a minimum period of time.
- The device does not damage delicate gum tissue.
Like any device, the design has disadvantages. On the first day of wearing, maximum salivation and impaired pronunciation of words are noticed. Sometimes the surface of the tongue is injured. It is impossible to adjust the device yourself; to do this you need to visit a dentist.
Mechanical elements of orthodontic appliances
Springs for expanding the dentition
To expand the dentition, different types of springs are used. These include Coffin, pear-shaped, pin-shaped, Koller, etc. springs.
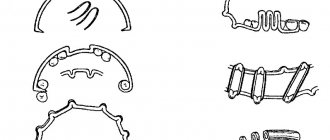
The Coffin spring (Fig. 26) is used to expand the upper dentition (usually sectorally), to lengthen it and mesio-distal movement of the teeth. It consists of a round, oval or pear-shaped bend and two fixing processes. Springs are made single or double. Single springs are made from orthodontic wire with a diameter of 0.7-1.5 mm, double springs are made from wire with a diameter of 0.8-0.9 mm for an external bend and 0.6-0.7 mm for an internal one.
Pin spring : Also designed to expand the maxilla. It is made according to the rules described above, but in the form of a part of a safety pin and of a greater length than the Coffin spring.
Pear-shaped spring - designed to expand the upper jaw, made according to the rules described above, but longer than the Coffin spring and pear-shaped.
The Koller spring is designed to expand the lower dentition. There are Koller springs for uniform and uneven expansion.
The Koller spring for uneven expansion of the lower dentition (Fig. 27.1) consists of a hyoid clasp, two semicircular bends and two fixing processes.
At the Department of Propaedeutics, Orthopedic Dentistry and Orthodontics, UMSA, they produce a modified Koller spring for uneven expansion of the lower dentition. It differs from the design described above in that the front part is made in the form of a rounded Coffin spring.
Rice. 27. Koller springs.
The Koller spring for uniform expansion of the lower dentition (Fig. 27.2) has 5 additional semicircular bends. They are made in the frontal section of the clasp, two on the right and left sides of the lingual frenulum and the central one, which goes around the lingual frenulum, in order to prevent injury to it.
Orthodontic screws
In practice, orthodontists more often use orthodontic screws to change the shape and size of dental arches, correct the position of individual and groups of teeth and bite.
An orthodontic screw is a factory-made mechanically acting element that is an integral part of the orthodontic apparatus.
The advantages of using screws are as follows:
1. The screws can be easily activated by both the patient and his parents.
2. The screws act with precisely measured force.
3. Screws can act in one or several planes simultaneously.
4. The two parts of the cut plate appliance with screw are more stable than the expansion spring orthodontic appliance.
5. The screws have different shapes and sizes, which facilitate their fixation in the base of the orthodontic apparatus.
6. Thanks to their design features, screws can move individual teeth, groups of teeth, dentitions and normalize the bite.
Depending on the purpose of use and design features, orthodontic screws are divided into 3 groups:
Group 1 – screws for moving individual or groups of teeth.
Group 2 – screws for normalizing the shape of the dentition:
a) for symmetrical bilateral expansion or contraction,
b) uniform symmetrical elongation,
c) uneven expansion - radial action (expansion of the frontal section is symmetrical and asymmetrical),
d) simultaneous expansion and elongation (uniform and uneven; symmetrical and asymmetrical).
Group 3 – to normalize the bite.
The force that is necessary to move teeth or change the shape and size of the dentition and normalize the bite develops when the screw is activated (unscrewed).
The screw body is usually made of nickel silver (nickel silver), and the drum (working part) of the screw is made of stainless steel.
Screws are classified by size: standard, medium, universal, microscrews and super microscrews.
The direction of activation on domestically produced screws is marked with a red dot, and on foreign ones - with an arrow. In the base of a removable orthodontic appliance, the screw is placed with the activation marking upward, so that activation occurs from bottom to top.
Orthodontic screws consist of a threaded main post and one or two drive pins. The main and driving pins have a common casing. The main pin has left and right hand threads. In the middle part of the screw there is a thickening - a drum - with four holes, which are designed to activate the screw.
The double-guide orthodontic screw (Fig. 28.1) consists of a rectangular body that has two identical halves. Inside the body there are three round longitudinal channels. The outer channels include 2 smooth guide pins, and the middle one has a double-sided thread and contains the screw itself. Either of the two guide pins is rigidly fixed at one end in the opposite halves of the screw body.
The screw with one guide pin is designed in the same way. Its body has 2 channels and 2 pins: one with a double-sided thread (screw), and the second - a guide (Fig. 28.2).
Rice. 28. Orthodontic screws with two guides (1) and one guide (2).
Screws with two guides are used for uniform expansion of the dental arch, and screws with one guide are used for unilateral lengthening of the dental arch, moving one or a group of teeth, etc.
The placement of a screw in the base of an orthodontic appliance made for uniform expansion of the upper jaw depends on the configuration of the palate or alveolar processes and the site of expansion. Most often, the screws are placed so that the first guide is designed between the midpoints of the oral surfaces of the first premolars (first primary molars). Less often - between the middle of the fangs. In this case, the cut of the apparatus passes through the middle of the hard palate (along the palatal suture).
Skeleton screws with one guide are made with a U-shaped straight bracket (Fig. 29.1) (guide) or with a curved one (Fig. 29.2).
Rice. 29. Skeleton U-Bracket Screws.
The latter is more consistent with the shape of the vault of the hard palate and is used on the upper jaw. Such screw designs are used to lengthen the frontal or distal parts of the upper and lower dental arches. The part of the screw with the bracket is located in the stationary part of the device, and the part that moves when it is unscrewed is in a small segment. When the spindle rotates, it slides along the guide along with the plastic sector and moves the tooth or teeth in the mesial, distal or vestibular direction
Radial or fan-shaped screws are used to expand the frontal portion of the upper dental arch. They can be symmetrical (Fig. 30.1) and asymmetrical (Fig. 30.2). When using such screws, the distal border of the base of the orthodontic apparatus ends at the level of the limiter hinge. Domestic and foreign companies produce two types of symmetrical fan-shaped screws. In one design, the drum and limiter are made as a single unit, and in the second design, the limiter is made separately. When inserted into the design of an orthodontic appliance, the stopper arms of such a screw must be moved apart to a width determined by the doctor.
Rice. 30. Fan-shaped (radial) screws.
Screws for simultaneous expansion and lengthening of the upper dentition (three-dimensional) are produced in two types: with two working drums and three. A screw with two working drums ensures uniform expansion and lengthening of the dentition (Fig. 31.1), and when using a screw with three drums, lengthening and uneven expansion of the upper dental arch on the left and right is possible (Fig. 31.2).
Rice. 31. Three-dimensional screws.
The domestic industry produces three-dimensional screws with independent expansion. In such screws, the drum, which lengthens the frontal section of the upper dental arch, is connected to the screw body with a hinge and, if necessary, can be shifted to the left or right side. In this case, there is an expansion of the frontal section of that side of the dental arch under which the screw is displaced (Fig. 31.3).
Push screws are available with a flat working part and a round one. The first are shown for corpus vestibular movement of individual teeth, and the second - with rotation around an axis (Fig. 32).
Rice. 32. Screw pushers.
Intermaxillary screws include the Weise screw, which is used in Wunderer activators for the treatment of mesial occlusion (Fig. 33).
Based on the amount of expansion when the screw is activated a full turn, the following types of screws are distinguished: with an expansion of 0.8 mm, 0.7 mm, 0.4 mm and 0.35 mm and a total expansion of 4 to 10 mm.
Activation of orthodontic screws is carried out by unscrewing the drum. Activation begins after the child has become accustomed (adapted) to the orthodontic apparatus. The activation mode is selected individually - the screw is activated within a period of 14 to 3-4 days.
Activation usually begins on days 7-14, gradually moving to activation on days 3-4.
Vestibular arches
Vestibular arches are used both to correct the position of individual or groups of teeth, and as fixing elements.
A regular vestibular arch can serve as a fixing element and be used to change the inclination of the frontal teeth (moves them in the oral direction) and to delay the growth of the frontal portion of the jaw (Fig. 34).
There are several types of vestibular arches.
Vestibular arch with a pressure loop (horizontal or vertical on one of the teeth) - used when one of the front teeth is in the vestibular position (Fig. 35).
Rice. 35. Vestibular arch with a pressure loop (vertical or horizontal) on one of the teeth.
Multi-link vestibular arch - used for more corpus movement of the front teeth in the oral direction.
A vestibular arch with M-shaped bends in the canine area is used to correct a vestibular canine, provided there is space in the dental arch (Fig. 36).
A vestibular arch with M-shaped bends in the middle is used to treat diastema.
A vestibular arch with one semicircular bend is used for lateral movement of incisors, elimination of asymmetrical diastema (which is caused by the incorrect location of one of the incisors), movement of the lateral incisor to the place of the removed central one, for distal movement of canines or premolars. The free end of the arch ends in a hook that encircles the tooth to be moved.
Oral arches
Oral arches are made, which are also called lingual (on the lower jaw) and palatal (on the upper jaw). They are used both for vestibular movement of anterior teeth and for fixation of orthodontic appliances, and for the purpose of retention of results achieved during active orthodontic treatment (Fig. 37).
Rice. 37. Oral arches.
The oral arch is used for fixing orthodontic appliances in the area of the lower front teeth and as an integral part of the Frenkel function regulators of types I and II.
The oral arch with one semicircular bend - as well as the vestibular arch with one semicircular bend and a free end, is used for lateral movement of the incisors. Its advantage is that it is inconspicuous to others.
An oral arch with three semicircular curves is used to eliminate diastema and three between the incisors.
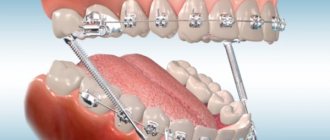
Upper jaw correction device
The device is designed to expand the upper jaw and change the permanent or mixed bite. The typical design consists of main rings that are placed on the sides of the teeth. One pair is placed on the premolars, and the other on the last teeth. The ring is used to solder power arcs arranged in a cross-shaped manner. In the central part of the device, in its middle, there is a special screw. It is necessary to activate the structure and provide continuous pressure on the side of the jaw.
Advantages of the device for expanding the upper jaw:
- It has a pronounced force effect, due to this, expansion occurs in a minimum time.
- Correcting a mixed bite takes about 30 days.
- With a permanent bite, problems are corrected within 4 months.
- The design moves the teeth body-wise.
- In this case, the jaw row spreads out to the sides, but the roots remain in their own holes.
- There is no increase in the depression in the gums.
- You can activate the design yourself. This is done using a special key.
- Activation is done once every 48 hours.
Disadvantages include damage to the tongue and rubbing of the tissues of the palate. To get a quick result, activation is carried out at 1 mm. This causes discomfort during therapy. The mechanism will require auxiliary means to clean the structure. Viscous and fermented foods should not be included in the diet.
Reviews
The design of the Coffin spring is particularly favorable for use in palatal expansion devices. If your child has had this surgery, there is a possibility that their device may have had a Coffin design installed.
If so, tell us what the result of the correction was? Were the hopes placed on it justified? You will find the comment form at the bottom of the page.
If you find an error, please select a piece of text and press Ctrl+Enter.
Tags: bite correction plates for teeth straightening
Did you like the article? stay tuned
Previous article
Expansion of the upper jaw in early mixed dentition using the Marco Ross apparatus
Next article
Instructions for using Pulposeptin paste in dentistry and a brief description of the product
Removable plate
The device is intended for the treatment of pathologies of mixed dentition. Expansion arches are used mainly for children from 6 to 11 years old. Characteristic design features:
- The device is used for uneven narrowing of the teeth line.
- The construction is made on a personal basis; for this purpose, casts of the jaws are made.
Expansion plates are a device that consists of a base plate and a special screw. The plates are made of hard plastic and follow the relief of the palate. The dental expander is formed taking into account sectoral cuts connected by special springs, which increase the pressure on the jaw bone. Depending on the problem, the activator screw is located in the middle of the plate or in the sector lobe.
When a certain area of the jaw is narrowed, a screw is placed on the plate from the side of the pathology. To ensure that the molars are adjusted at the same time, vestibular metal arches are installed on the device. The main advantages of the device:
- The spacer has a complex effect; after use, the arches expand and the frontal section is leveled.
- The design is often used in dentistry because it has affordable care.
- Hygienic cleaning is carried out by the child; if desired, the structure can be removed.
- The adaptation period is painless, because the device is removed with your own hands, the cheeks on the inside are not injured.
- It is easy to insert the structure back.
The expansion plate has disadvantages. Some clients take a long time to get used to it due to its volume. Some people experience vomiting when wearing orthodontic appliances. The plate is replaceable, so constant monitoring is required when using it. If the product is rarely used, the treatment period will be long.
Coffin, Koller and club spring
Additional accessories in the form of springs are often used with the expansion apparatus. They enhance the effect of the structure and shorten the correction period. Several types of springs are used for this purpose:
- Collera. A spring is often prescribed to adult patients; it allows the lower row of teeth to be expanded. Depending on the design, the palatal device is used for sectoral or uniform correction.
- Coffin's device. Actively used for catarrhal expansion of the jaw and enlargement or movement. The Coffin spring is a round, pear-shaped or oval curve with two parts for fixation on the main apparatus.
- The spring is club-shaped. Used to eliminate narrowing of the upper lobe. Manufactured from wire. The shape of the design resembles a safety pin.
For uniform expansion of the jaw, a spring is used, which is made in the form of a hyoid yoke, with two round bends and parts for fixation. To change the sectoral segment of the jaw, use a design with one semicircular bend in the front part.
Manufacturing technique
Single-circuit models are made from wire Ø 0.7-1.5 mm, double-circuit - 0.8-0.9 mm for the external circuit, 0.6-0.7 mm for the internal circuit.
The production of Coffin structures is carried out on a plaster model in the following order (single-circuit version):
- In the center of the palatal recess of the model, the outline of the product is drawn with a chemical pencil.
- Take a piece of wire Ø 0.7-1.5 mm, 80 mm long, and bend it to the shape of the pattern using pliers.
- A gasket made of metal foil or plaster is placed on the palatal part of the model, and a spring is placed on it. The spacer is necessary to ensure that the device is 0.6-0.7 mm away from the palate.
- The packaging is made with chemically or photopolymerized plastic so that the ends are molded into the polymer mass.
Coffin structures can be made from standard blanks. If a double-circuit structure is made, the distance between the outer and inner contours is 1-1.5 mm.
Design features of a functional fixed telescopic device and the principle of its operation.
In this publication we will talk about the appointment of the Bruxogard trainer.
Here https://orto-info.ru/sistemyi-vyiravnivaniya-zubov/lechebno-profilakticheskie-apparatyi/sustavnaya-shina-tmg.html you will find objective reviews about the TMJ joint splint.
Distractor for the lower jaw
This device stands out among other devices. It consists of a smooth body on which a self-expanding screw and slide are placed, and there are also levers with wedge-shaped ends. With its help, crossbite is corrected.
The device eliminates the anomaly and fills the emerging space in the bone tissue. The design has different types, they are aimed at solving various problems that are associated with a narrowing of the dental arch. This allows the use of a distractor to treat children.
Surgical intervention
Surgical methods are used to narrow the jaws. If there is no positive effect after hardware therapy, the doctor prescribes surgical treatment. The operation occurs in several stages:
- First, the patient is given anesthesia. This is usually general anesthesia because there is a deep injury to the mouth.
- An ultrasonic scalpel is used to make an incision into the mucosa and periosteum. Depending on the nature of the disease, the section is made on one or both sides of the jaw.
- The soft tissue is then peeled away, exposing the cortical part of the jaw.
- Using perforation, the necessary segments are dissected. A special device is installed manually.
- Then the patches are returned to their place and stitched together.
The correction begins three days after surgery. Primary activation is carried out by the dentist, and then the procedure is performed by the client at home. Activation is a painless action that does not cause difficulties for the client.
Duration of treatment
The period of action of the surgical technology varies depending on the client’s age and jaw pathology. Typically, the duration of therapy from surgery to final healing is 30 days. After this, the client undergoes hardware treatment, which corrects the development of some anomalies and restores the required position of the molars.
Therapeutic hardware treatment lasts up to six months. To consolidate the results obtained, a retention course is carried out; the duration of therapy is about 9 months. The total treatment time takes about 1 year.