20.01.2017
Upper micrognathia or underdevelopment of the upper jaw is a rather rare type of deformation of the upper jaw, which can be caused by both endo and exogenous factors. Differential diagnosis of this pathology can be carried out in comparison with the false form, the cause of which is excessive development of the lower jaw.
Visually, underdevelopment of the upper jaw has the appearance of a mesial bite. Externally, true micrognathia is manifested by a sharp forward expression of the nose and retraction of the upper lip, and the expression of the nasolabial furrows. At the same time, functional malocclusion is expressed in difficulties in biting off food due to the lack of antagonists. Speech is often impaired. Diagnosis is carried out using tomography of the maxillofacial area.
Anomalies of dental development
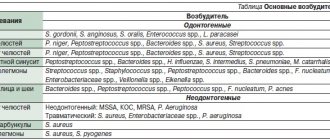
The most common anomalies in the structure of hard tissues are systemic or local hypoplasia of permanent or temporary teeth. Systemic hypoplasia looks like a white or yellow spot with a smooth surface. It is impossible to determine it using x-rays. Pits or grooves appear in the image as areas of clearing.
Local hypoplasia develops most often due to injury to the follicle or against the background of chronic inflammation of the periodontium of a milk tooth - in a permanent tooth. Enamel hyperplasia is rare and appears on an x-ray as a more intense, dense shadow.
Diagnosis of the problem
The presence of mesial occlusion is indicated by characteristic changes in a person’s appearance, which are noticeable already at the stage of preliminary diagnosis during a visual examination of the patient:
Signs of malocclusion:
- The chin and lower lip are pushed forward, the chin is massive, the upper lip is sunken.
- The middle third of the face is sunken; when viewed in profile, the face looks concave.
- The face has an angry expression.
- The mouth gapes (observed in severe cases of the disorder).
- The nasolabial triangle is pronounced.
When assessing the structure and shape of the jaws, the following features can be noticed:
- Reverse incisal overlap (mesial shift of the crowns of the first permanent molars by half the width of the cusp or more is the main diagnostic sign of mesiocclusion).
- Sagittal gap between the upper and lower incisors.
- Anomalies of tooth growth.
In severe forms of the pathology, postural disorders develop (the upper part of the body is tilted back, and the pelvic bones are tilted forward)
To clarify the diagnosis, hardware diagnostic methods are used:
- tomography of the maxillary joint;
- orthopantomography (detailed examination of teeth, adjacent tissues and areas of the facial skeleton);
- rheography (vascular examination);
- electromyography of the muscles of the head and face.
The severity of the mesial bite is determined using special bite ridges.
Anomalies in the number of teeth
The number of teeth may decrease due to the absence or death of rudiments, or increase. Primary adentia occurs mainly in the permanent dentition. With complete teeth, all teeth are missing; with partial teeth, the upper lateral incisors and lower second molars are missing. This happens with ectodermal dysplasia.
Supernumerary teeth are characterized by an irregularly shaped crown. They erupt for a long time and remain in the jaw. An x-ray - panoramic study - allows you to determine this or that anomaly.
Sometimes a tooth is missing from a row due to retention - retention of the tooth in the jaw bone. It is provoked by its incorrect initial position, lack of space or narrowing of the dentition. X-ray examination allows you to determine the position of the impacted tooth and its relationship with the surrounding anatomical formations. For this purpose, special techniques are used - tomography, oblique projections, etc.
Mesial step in primary dentition
When examining the oral cavity and assessing the relative position of the dentition in a child, the presence of a mesial step in the temporary dentition may be observed. This is a vertical ledge that is formed when the second temporary molars are closed. This sign is called Tselinsky’s symptom (a prognostic criterion that indicates the possibility of the formation of a mesial occlusion in a child). The appearance of a mesial step in the primary dentition is normal if the crowns of the lower second molars are no more than 2 mm wider than the crowns of the upper second molars.
The presence of a small mesial step indicates the correct installation of the first permanent molars. As a result, the first permanent molars are able to erupt in a neutral position.
A pronounced mesial step indicates a possible mesial position of the lower molars in relation to the upper ones.
Anomalies of jaw development
These abnormalities may be congenital or occur after illness, injury, endocrine disorders, or radiation therapy.
- Congenital clefts
of the hard palate and alveolar process are recognized in clinical practice and are often caused by genetic causes. The pathology is often accompanied by dental anomalies, delayed development of permanent dentition, and deformation of the nasal cavity. - Cranioclavical dysostosis
is a congenital systemic disease, which is characterized by changes in the dental system. Due to anatomical pathologies, the upper jaw remains underdeveloped, and the hard palate is shortened; permanent teeth erupt by the age of 20-30, and many of them are impacted, supernumerary and dystopic. - Craniostenosis, or craniofacial dysostosis
, is premature synostosis of the sutures in the bones and base of the skull, when the skull is stretched vertically, intracranial pressure changes, and other pathological processes develop. - Maxillofacial dysostosis
- on X-ray images it is indicated by underdevelopment of both jaws, the zygomatic arch and bone, deformation of the orbits, as well as malocclusion and abnormal development of molars.
There are anomalies of the dental system caused by endocrine disorders. For example, in the category of children with incorrect functioning of the thyroid gland, delayed teething is diagnosed, multiple caries often develops, and underdevelopment of the jaws is also observed.
If there is a history of deficits in the functioning of the anterior lobe of the pituitary gland, the roots of baby teeth may not be resolved, but remain for life, interfering with the eruption of permanent ones. In turn, with hyperfunction of the pituitary gland, the roots grow too quickly, the time for eruption is reduced, and hypercementosis develops at the tips of the roots. Children with Down syndrome begin to erupt primary teeth at 4-5 years of age, but they often do not fall out until 14-15 years of age.
Underdevelopment of the upper jaw - a clinical case
A patient with skeletal asymmetry due to underdevelopment of the upper jaw came to us for further planning of orthognathic double-jaw surgery.
Rice. 1. Photo of the patient. Skeletal asymmetry. Underdevelopment of the upper jaw.
Rice. 2. Intraoral photograph of underdevelopment of the upper jaw.
Cone beam computed tomography (CBCT) was performed with further planning for orthognathic bimaxillary surgery.
Fig.3. Planning for orthognathic double-jaw surgery.
Devices for the treatment of mesial occlusion
Treatment of mesial malocclusion is a rather lengthy process and takes from 3 to 5 years. The duration of therapy depends on the patient's age and stage of the disease. At the first and second stages of mesial occlusion, the use of orthodontic appliances has a good effect:
- Dilyar face mask;
- braces;
- veneers.
Dilara face mask
The Dilyar facial mask is used to correct the bite in childhood and adolescence. The structure can be used as an independent means (to stimulate the growth and development of the jaw) or as an auxiliary means (when undergoing a course of treatment with braces). To achieve the effect, the Dilyar mask must be used for a long time.
Correction of mesial bite with braces
Braces are non-removable structures for correcting the position of teeth in various types of malocclusion. Braces are prescribed to correct mesial occlusion in children and adults. There are no age restrictions.
The method is effective when used in the early stages of the disease. The course of treatment is long. The quality and speed of treatment depends on the stage of the disease, the professionalism of the doctor and the discipline of the patient.
The bracket system is adjusted so that the pressure is soft and the movement is smooth. This determines the duration of treatment. The use of orthodontic systems helps eliminate crowding of teeth, normalize the shape of the dentition, and eliminate facial asymmetry. Treatment with braces does not completely solve the problem. Their use cannot change the size of the jaws or excessive inclination of the teeth.
Clinic specialists use several types of modern brace systems:
- plastic;
- metal;
- incognito braces;
- bracket systems from Danon.
Correction with veneers
Veneers are special overlays up to 1.2 mm thick that are attached to the outside of the teeth. They improve the aesthetics of the dentition.
With the help of veneers, you can only slightly reduce crowding of teeth and eliminate minor bite defects. They do not ensure tight closure of the chewing surfaces of the teeth of the upper and lower jaws. Poor closure can cause destruction of decorative overlays.
If there are bite problems, veneers are used only after orthodontic treatment (braces, aligners or aligners), at the stage of restorative therapy.
Treatment of mesial occlusion
Malocclusion is not only an aesthetic problem. If left untreated, mesial malocclusion progresses, causing general deterioration in health and significant changes in appearance.
The sooner correction of mesial occlusion is started, the better results it will bring. After all, in childhood, the dental system is still plastic and continues to form.
In adult patients, treatment is more complex and lengthy. In the initial stages of mesial occlusion, therapy using orthodontic systems is possible. If the disease is advanced, surgery cannot be avoided.
Treatment in adults
In adults, it is more difficult to correct the size of the jaw bones using hardware methods. Orthodontic structures can straighten the dentition, but they cannot change the size and position of the jaw. Complex violations are eliminated surgically, after which ideal contacts between antagonist teeth are achieved using a braces system.
In mild cases, when the anomaly in the structure of the jaws is not clearly expressed and there are no problems with closing the lips and teeth, surgical intervention is not resorted to. In this case, the use of orthodontic systems helps. But to achieve a visible effect, you will have to wear the braces system for 3-5 years.
Surgery to correct mesial malocclusion
At stage 3 of mesial occlusion, when the sagittal gap between the front teeth is more than 10 mm (and between the first molars - from 10 to 18 mm), the patient is indicated for surgical intervention.
Surgery helps eliminate pathological deformation of the temporomandibular joint. As a result, a number of dental problems go away, the general health and appearance of the patient improves. The person becomes calmer and more balanced.
Exercise to correct mesial bite
To consolidate the results achieved during treatment and restore facial symmetry, it is necessary to improve the functioning of the jaw muscles. During the rehabilitation period, the patient is prescribed a therapeutic set of exercises for this muscle group. Myogymnastics are done daily (morning and evening). Each exercise is repeated 5-10 times.
- Rhythmically open and close your mouth.
- Starting position: the tip of the tongue touches the back palate. In this position, open and close your mouth.
- Rest your elbows on the table, place your chin on your palms. Open and close your mouth, but move your head, not your jaw.
- Repeat the first exercise.
- Strongly straining the muscles, press the tip of the tongue on the area of the upper palate until the muscles feel tired.
- Open and close your mouth. In the “mouth closed” position, reach the back palate with the tip of your tongue.
- Smoothly pull the lower lip under the upper jaw and lower it just as smoothly.
- The jaw muscles should be under stress. To do this, it is useful to chew hard vegetables and fruits more often.
Exercises are both therapeutic and preventive in nature. They should be carried out as directed and under the supervision of the treating dentist.