Quick Transition Treatment of Peritonsillar Abscess
A peritonsillar abscess (PTA) is a collection of pus between the tonsil capsule and the pharyngeal muscles.
The anterior PTA is most often diagnosed; it is localized between the upper pole of the tonsil and the anterior palatine arch. They also distinguish between the posterior PTA - between the tonsil and the posterior palatine arch, the lower PTA - at the lower pole of the tonsil, the external PTA - outside the tonsil.
Peritonsillitis is an infectious inflammatory disease of the tissue surrounding the palatine tonsil, without the formation of an abscess (cavity with pus).
Paratonsillitis or PTA is usually preceded by acute tonsillopharyngitis, but in some cases the disease can develop without a previous infection of the pharynx, which is associated with blockage of the salivary glands.
Peritonsillar abscess is the most common infection of the deep tissues of the neck in children and adolescents, accounting for at least 50% of cases. The annual incidence of PTA is 30-40 cases per 100,000 people aged 5 to 59 years.
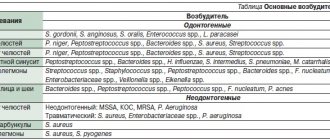
The main causative agents of PTA are Streptococcus pyogenes (beta-hemolytic streptococcus group A, GABHS), Streptococcus anginosus (angios streptococcus), Staphylococcus aureus (Staphylococcus aureus, including methicillin-resistant strains - MRSA) and respiratory anaerobes (including Fusobacteria, Prevotella and Veillon).
Description of the disease
Cellulitis of the maxillofacial area
Phlegmon is a purulent inflammation that occurs in soft tissues.
The pathological process does not have clear boundaries, which is why it quickly spreads to blood vessels, nerve endings and organs.
Phlegmon of the maxillofacial area mainly affects bone tissue and tendons, salivary glands, and muscle tissue.
Cellulitis is a dangerous pathological condition. Due to the purulent-inflammatory process, a large amount of toxic substances enter the bloodstream, which causes general intoxication of the body.
The disease is acute, characterized by the rapid development of symptoms, against the background of which the functions of the masticatory apparatus, swallowing, and breathing are impaired in patients.
Phlegmon in ICD 10
In the international classification of diseases, phlegmon of the maxillofacial area is included in the group of diseases of the skin and skin tissue (L00 - L99). The pathology is included in the block of infectious skin diseases and is designated in the ICD by code value L 03.2.
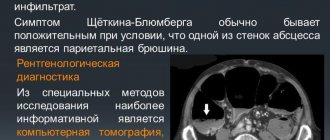
Diagnostics
In the vast majority of cases, the diagnosis of PTA is made clinically, based on the results of pharyngoscopy (examination of the pharynx). It is confirmed by obtaining purulent discharge during drainage of the abscess or by instrumental studies (most often ultrasound).
Pharyngoscopy reveals a swollen and/or fluctuating tonsil with deviation of the uvula in the direction opposite to the lesion, hyperemia (redness) and swelling of the soft palate. In some cases, there is plaque or liquid discharge in the palatine tonsil. There is an increase and tenderness of the cervical and submandibular lymph nodes.
Bilateral PTA is extremely rare and its diagnosis is more difficult due to the lack of asymmetry in the pharynx, as well as the rarely present spasm of the masticatory muscles.
Laboratory tests are not required to make a diagnosis; they are additionally prescribed to determine the severity of the disease and select a treatment method.
Laboratory tests may include:
- general blood test with leukocyte formula;
- study of electrolytes (potassium, sodium, chlorine) for signs of dehydration;
- strepta test to exclude GABHS;
- culture for aerobic and anaerobic bacteria if the abscess was drained (culture is recommended only for complicated PTA, recurrent PTA, or in patients with immunodeficiency conditions).
Instrumental examination methods - ultrasound, computed tomography, lateral neck x-ray, magnetic resonance imaging or angiography - are not necessary and are performed to exclude other diseases if the diagnosis of PTA is not obvious.
Differential diagnosis
Severe course of acute tonsillopharyngitis . Frequent pathogens are Epstein-Barr virus, herpes simplex virus, Coxsackie virus (herpangina), adenovirus, diphtheria, GABHS, gonorrhea. It manifests itself as bilateral swelling in the throat, hyperemia, and plaque may be present on the tonsils.
Epiglottitis . An inflammatory disease of the epiglottis, usually caused by Haemophilus influenzae. More common in young children who have not been vaccinated against Haemophilus influenzae type b. Progresses faster than PTA. Manifested by sore throat, drooling, difficulty swallowing, respiratory failure.
Retropharyngeal abscess (retropharyngeal abscess) . Purulent inflammation of the lymph nodes and tissue of the retropharyngeal space. Most often observed in children aged 2 to 4 years. During pharyngoscopy, minimal changes are noted. Main complaints: stiff neck, pain on movement, especially when extending the neck (as opposed to the increased pain on flexion seen with meningitis), swelling and tenderness of the neck, chest pain, difficulty swallowing, drooling, muffled voice, spasm of the masticatory muscles ( present in only 20% of cases).
Causes of phlegmon of the maxillofacial area
The causative agent of phlegmon is bacterial microorganisms: streptococci, pneumococci, staphylococci, E. coli
Cellulitis of the maxillofacial area is an infectious disease.
The causative agent is predominantly bacterial microorganisms: streptococci, pneumococci, staphylococci, E. coli.
Pathogenic microflora penetrates the subcutaneous fatty tissue through small skin lesions.
Most often the cause is odontogenic, but infection through the lymphatic or circulatory system is possible.
Anaerobic bacteria (clostridia) and non-spore-forming microorganisms (peptococci, poststreptococci) also act as pathogens.
The presented microorganisms are able to reproduce in the absence of oxygen. They cause the rapid development of necrotic processes in tissues.
Factors contributing to the development of the disease:
- Reduced immunity;
- The presence of allergies with severe skin manifestations;
- Acute or chronic tonsillitis;
- Carious lesions of teeth;
- Contact with aggressive substances under the skin;
- Furunculosis;
- Use of low-quality cosmetics;
- Failure to comply with hygiene standards.
Development mechanism
When an infection enters the subcutaneous environment, inflammation rapidly develops. The high intensity of the pathological process is explained by several factors.
These include:
- Rapid development of intoxication;
- Lack of an adequate immune response of the body;
- Decreased local immunity;
- The presence of optimal conditions for the growth of bacteria.
Due to the rapid development, granulation tissue does not have time to form, which should protect the source of inflammation from healthy tissue. Therefore, the pathological process spreads quickly.
Symptoms
Symptoms of inflammation occur quickly, which is explained by the short incubation period of bacteria
The nature of clinical manifestations varies depending on the location of inflammation.
As a rule, the pathology is acute. Symptoms of inflammation occur quickly, which is explained by the short incubation period of the bacteria.
Main features:
- High body temperature;
- Symptoms of general intoxication (nausea, vomiting, dizziness);
- Muscle weakness, tremors;
- Chills;
- Headache;
- Toothache;
- Decreased appetite;
- Pain when swallowing.
Important to remember! Local symptoms, such as swelling, swelling of the skin, redness, do not appear immediately. Therefore, the symptoms of phlegmon are often mistaken for other diseases. A distinctive feature is intense pain at the site of inflammation.
External signs
After symptoms of inflammation appear on the skin at the site of the lesion, local symptoms occur.
These include:
- Swelling;
- Change in skin color;
- Hyperemia;
- Cracks in the skin;
- Pain when moving;
- Formation of a purulent fistula.
Conventionally, the course of phlegmon can be divided into 2 stages. At the first stage, a dense formation appears under the skin, which is easily felt by palpation. At the next stage, the compaction softens, indicating the secretion of pus.
Symptoms of paratonsillar abscess
The typical clinical manifestation of PTA is severe sore throat (usually unilateral), fever, and muffled voice. Patients may also complain of drooling and difficulty swallowing.
Trismus (spasm of the masticatory muscles), associated with irritation and reflex spasm of the internal pterygoid muscle, occurs in almost 2/3 of patients and is an important distinguishing feature of PTA in comparison with severe acute tonsillopharyngitis. Patients may also complain of neck swelling and ear pain on the affected side.
Types of phlegmon
Phlegmons of the maxillofacial area in dentistry are classified depending on the location.
The main types of pathology are presented in the table below:
| Localization | Characteristic |
| Phlegmon of the temporal region | It is an inflammatory formation in the subcutaneous layer in the temple area. Accompanied by throbbing pain, the intensity of which depends on the depth of the lesion. With superficial phlegmon, severe swelling is noted. In some cases, due to temporal phlegmon, the patient cannot open his mouth normally. |
| Orbital phlegmon | The purulent-inflammatory process occurs in the fatty tissue of the orbit. In most cases, the pathology is one-sided. Accompanied by intense headaches, severe swelling of the eyelids, conjunctiva, and protrusion of the eyeball. Eye movement is limited. A significant decrease in visual acuity or its complete absence is possible. |
| Phlegmon of the subtemporal space | A purulent-necrotic process occurring in the infratemporal fossa. Occurs against the background of caries of the upper teeth. It is also possible for phlegmon to spread from the area of the upper jaw and temples. Patients experience pain above the upper jaw, which radiates to the ear, temple or teeth. |
| Phlegmon of the peripharyngeal space | Phlegmon in this area occurs against the background of carious lesions of the lower teeth and infectious diseases. Accompanied by moderate pain that is permanent. There is an increase in local lymph nodes, difficulty swallowing and opening the mouth. |
| Phlegmon of the pterygomaxillary space | The pathology is localized in the area of the pterygomaxillary fold. Phlegmon occurs mainly against the background of carious lesions and other dental diseases. Infection is also possible if antiseptic standards are not observed during torusal anesthesia. There is pronounced facial asymmetry. The patient is unable to open his mouth and swallow food normally. There is hyperemia of the mucous membrane. |
| Phlegmon of the parotid region | It occurs against the background of a purulent form of lymphadenitis, the presence of carious lesions in the upper molars. Accompanied by swelling of the tissues of the parotid region. In this case, the skin color, as a rule, does not change. There is pain when moving the jaw. |
| Phlegmon of the chewing area | Localized in the area of the masticatory muscles (cheeks). Accompanied by severe swelling, facial asymmetry, and pain. Mouth movements when chewing are limited. |
| Cellulitis of the floor of the mouth | Located in the sublingual or submandibular region. Accompanied by swelling under the tongue and pain. The patient has difficulty breathing and increased salivation. The mobility of the tongue decreases due to which speech defects occur. The tissues under the tongue acquire an unhealthy shine and turn red. |
Cellulitis of the jaw space occurs against the background of carious lesions and other dental diseases
Oral abscess - symptoms and treatment
Symptoms of oral abscesses are variable and depend directly on the type and location of the abscess. In acute purulent periostitis, patients complain of pain in the area of the causative tooth or jaw segment, swelling of the soft tissues. The face of such a patient is asymmetrical.
When the causative tooth is localized in the frontal part of the upper jaw, the swelling is located in the upper lip and infraorbital region, the nasolabial fold is smoothed. If the diseased tooth is located in the frontal region of the lower jaw, swelling of the soft tissues is noted in the area of the lower lip and chin. When the causative tooth is located in the lateral part of the dentition, perifocal edema (near the infectious focus) is located in the buccal region.
Acute purulent periostitis is usually not accompanied by restrictions in mouth opening. Palpation of regional lymph nodes often reveals signs of acute lymphadenitis (enlarged lymph nodes). When examining the oral cavity, the causative tooth is identified, which usually reacts sharply to tapping (percussion). This is explained by the presence of a pathological process behind the root apex. When examining the vestibule of the oral cavity, a painful inflammatory infiltrate is determined, over which there is an edematous and hyperemic (red) mucous membrane. According to the literature, periostitis is most often located on the side of the cheek or lips, less often on the palatal and lingual side [5][8].
Often abscesses of the maxillo-lingual groove, buccal region, and pterygomaxillary space are considered as a complication of acute purulent periostitis. However, in some cases these diseases develop independently, so there is no reason not to consider them in this review.
Abscess of the maxillo-lingual groove is characterized by a more serious course. The patient complains of pain when swallowing, moving the tongue to the sides, and limited mouth opening. A visual examination reveals swelling of the submandibular area and acute lymphadenitis. Examination of the oral cavity is often difficult and is only possible after blocking the motor branches of the mandibular nerve. When examining the oral cavity, acute or aggravated periodontitis of the chewing tooth of the lower jaw or difficult eruption of the lower wisdom tooth is determined. When examining the maxillo-lingual groove, its bulging is determined; upon palpation, an inflammatory, sharply painful infiltrate can be detected.
With an abscess of the pterygomaxillary space, the patient notes an increase in body temperature, pain in the pharynx, difficulty swallowing, mouth opening is limited, in some cases almost impossible. Visually, perifocal edema is often absent. An examination of the oral cavity can be carried out only after blocking the motor branches of the mandibular nerve. In the oral cavity, difficult eruption of the lower wisdom tooth is usually detected, as well as a hyperemic and edematous pterygomandibular fold.
The clinical picture of an abscess in the buccal region largely depends on the depth of the abscess. With a superficial abscess, hyperemia (redness) of the skin, a local increase in temperature, the skin is tense and does not fold. With a medium and deep location, there is pronounced swelling of the buccal area, the skin is not externally changed, it is difficult to fold into a fold. Local hyperthermia (increased temperature) is usually not observed. When the abscess is deeply located on the mucous membrane of the cheek, marks from teeth are detected.
The condition of patients with these abscesses is usually assessed as moderate. Treatment is usually carried out in a maxillofacial surgery hospital under supervision in order to prevent the development of severe complications. Patients often exhibit symptoms of general intoxication of the body (fever, headaches and muscle pain).
Diagnostic procedures
The diagnosis is made on the basis of anamnesis and external examination of the patient. The presence of acute or chronic infectious diseases is taken into account. Auxiliary diagnostic procedures are prescribed to determine the severity of the pathology.
During diagnosis, it is extremely important to determine the type of infection that provokes the pathology. This will allow further effective antibacterial treatment.
To determine the type of pathogen, a puncture biopsy is performed, during which purulent contents are collected, which are further studied in the laboratory.
Treatment
The nature of therapeutic procedures depends on the severity of phlegmon and its location. The pathology is potentially life-threatening, and therefore requires hospitalization of the patient.
Drug therapy
Treatment involves taking medications in strict accordance with the dosages prescribed by the doctor.
The following groups of drugs are used:
- Treatment involves taking medications in strict accordance with the dosages prescribed by the doctor.
Antibiotics. The action is aimed at destroying pathogenic microflora, thereby stopping the development of inflammation. Antibacterial therapy is most effective at an early stage, before tumor formation. In later stages, antibiotics are used as an adjuvant. Patients are prescribed intramuscular injections of Erythromycin, Cefuroxime and Gentamicin. On average, the duration of therapy is 3-5 days.
- Anti-inflammatory drugs. They are used to reduce tissue swelling, eliminate hyperemia, and pain. Medicines are prescribed by a doctor taking into account pharmacological interactions with antibiotics. In most cases, drugs based on Diclofenac and Nimesulide are used.
- Local antiseptics. Used for local treatment of phlegmon, which is required in the formation of a purulent fistula. For disinfection, a solution of chlorhexidine, Furacilin, and less commonly Boric acid and hydrogen peroxide are used.
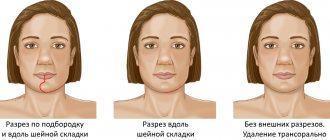
Surgery
The operation can be performed during planned treatment or urgently, if the patient’s condition worsens.
Purulent phlegmon is treated surgically. The operation can be performed during planned treatment or urgently, if the patient’s condition worsens.
The presented treatment option is considered more preferable than drug therapy, as it eliminates the risk of complications and re-development of the pathology.
The main indication for surgery is the presence of an inflammatory focus and elevated body temperature of the patient.
The procedure is performed under general anesthesia. The phlegmon is opened with a wide incision, which allows for the outflow of purulent substance.
After the pus is released, the affected area is washed and disinfected. Bandages containing antibacterial ointments are applied to the incision. If the skin does not heal well, dermoplasty is performed.
Physiotherapy
The use of physiotherapeutic procedures is considered appropriate only at the early stage of pathology. Physiotherapy methods can also be used for symptomatic treatment.
Basic methods:
- UHF therapy;
- Ultraviolet irradiation;
- Light therapy;
- Ultrasonic treatment of opened phlegmon;
- Laser treatment of the wound.
Alternative medicine
Traditional methods are not recommended for use in acute illness. The use of unconventional methods is possible during the period of postoperative rehabilitation.
For better healing of affected skin, it is recommended to apply sea buckthorn or rosehip oil. For general strengthening of the body, medicines made from the herbs Eleutherococcus, Chinese magnolia vine, ginseng, and rose hips are used.
Odontogenic infection
Odontogenic periostitis
Depending on the clinical course, periostitis can be acute (serous, purulent) or chronic (simple, hyperplastic).
In the area of the affected tooth - the probable source of infection - pain is felt, radiating to the ear and temple. Swelling of the cheek and asymmetry of the face due to unilateral swelling of soft tissues are often visually noticeable. Difficulty opening the mouth. With odontogenic periostitis, general health suffers: weakness, febrile temperature, headache, sleep and eating disturbances. Regional lymph nodes are enlarged and painful.
Odontogenic osteomyelitis
It is more often diagnosed in men in the age group of 20-40 years, in 68% of cases it affects the lower jaw. Against the background of a pronounced intoxication syndrome, intense local pain in the tooth or diffuse pain in the entire jaw, which spreads to the corresponding half of the head, is disturbing. The configuration of the face is changed due to swelling on the side of inflammation.
There are difficulties when opening the mouth, pain when chewing and swallowing food, impaired speech function, paresthesia of the upper or lower lip. There may be a putrid odor from the mouth. The temperature curve for odontogenic osteomyelitis ranges from 37.5 to 39-40°C.
Odontogenic sinusitis
Odontogenic sinusitis accounts for 10 to 30% of all cases of infections of the maxillary sinuses. Acute sinusitis manifests itself with headache, temperature reaction, and a feeling of pressure in the projection of the corresponding sinus. Swelling of the nasal cavity increases, breathing becomes difficult, and the sense of smell decreases. After some time, a mucopurulent or purulent secretion begins to separate from the sinus. The soft tissues of the infraorbital region and cheeks look swollen.
Odontogenic abscesses and phlegmons
About 57% of purulent infections of the soft tissues of the head and neck have a dental etiology. Odontogenic abscesses are usually localized in the infraorbital, buccal, submandibular, and parotid regions. Accompanied by the appearance of swelling in the face or neck, hyperemia of the skin over the abscess. With a superficial abscess, a symptom of fluctuation is felt. There is local pain and pulsation in the projection of the abscess. Signs of intoxication are moderate.
Based on localization, odontogenic phlegmons of the floor of the mouth, submandibular, submental, peripharyngeal space, and neck area are distinguished. There is swelling of soft tissues without clear boundaries with the presence of a dense painful infiltrate. The pain is spontaneous, diffuse, and constantly present. Depending on the location of the phlegmon, chewing, swallowing, breathing, and speech are impaired. Characterized by a pronounced deterioration in general health, febrile fever, chills.
Odontogenic lymphadenitis
Usually develops in the area of the submandibular or cervical lymph nodes. They are characterized by local swelling, pain, and dense consistency. Facial asymmetry occurs. When lymph nodes become abscessed, body temperature rises, chills and malaise appear. When palpating a purulent focus, fluctuation is felt.
Forecast
The likelihood of complications increases significantly in the absence of timely assistance
If you seek medical help in a timely manner, the prognosis is favorable.
The pathology can be successfully treated surgically, and with the help of auxiliary drug therapy, the symptoms are eliminated and the general condition of the patient is normalized.
The likelihood of complications increases significantly in the absence of timely assistance.
In such situations, phlegmon can cause conditions that threaten the patient's life.
Possible complications
Possible complications of phlegmon in the maxillofacial area include:
- Blood poisoning and septic shock;
- Impaired brain activity due to intoxication;
- Asphyxia;
- Impaired cerebral circulation due to compression of blood vessels;
- Thrombosis of the neck veins;
- Development of a brain abscess.
Important to remember! In the absence of timely treatment, phlegmon can cause a skin defect that will persist even if treatment is successful.