Tumor of the lower jaw involves complete or partial resection of the lower jaw. If reconstructive surgery is not performed, the person becomes disabled and drops out of society.
Reconstructive surgery is the restoration of the form and function of a body part using a person’s own tissue.
Reconstruction of the lower jaw allows you to completely restore the patient’s appearance, chewing and speech function, without resorting to removable dentures.
Cut options
There are three options for accessing the tumor:
- The classic approach involves an incision along the chin and along the neck fold;
- In most cases, an incision along the chin can be avoided and the operation can only be performed through an “invisible” incision in the neck fold;
- In the case of marginal resection of the lower jaw, the operation can be performed transorally - access through the mouth, without external incisions.
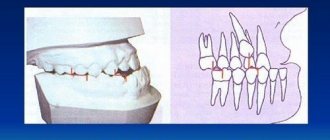
Incision options for resection of the lower jaw
The classical approach is becoming a thing of the past, but in Russia it is still widely used, because Most surgeons do not have the necessary skills to perform an operation only through an incision in the cervical fold.
In my practice, I use all access options depending on the indications.
Malignant tumors of the upper jaw
Clinical manifestations of malignant neoplasms of the upper jaw are diverse, but not pathognomonic and depend on the initial location of the tumor, prevalence, shape and direction of preferential growth, and morphological structure.
Since epithelial malignant tumors originate from the mucous membrane of the maxillary sinus, in stages 1 - 2 they are usually an accidental finding (for example, during gairotomies), because tumors of such prevalence are not available for visual observation, symptoms may resemble ordinary sinusitis, or even absent. This explains the predominant detection of malignant tumors of the upper jaw in stages III-IV. In a significant proportion of patients, the first symptoms are pain of various types in the upper jaw, radiating to the head. Often the disease is manifested by pathological changes in the nasal cavity: one-sided difficulty or complete absence of nasal breathing, serous-purulent or bloody discharge. More rare first symptoms of malignant tumors of the upper jaw are unilateral profuse lacrimation, swelling of the eyelids or soft tissues of the face of the corresponding side, and impaired skin sensitivity. Some patients, as the first sign of disease, note a tumor in the upper jaw that is already visible to the naked eye.
To fully characterize the clinical manifestations of malignant tumors of the upper jaw and accurate topical diagnosis, in 1933 the Swedish oncologist Ohngren proposed a conditional division of the jaw into sectors. It is carried out by drawing an imaginary inclined plane starting from the inner corner of the orbit and going to the corner of the lower jaw. Two sectors or segments are obtained: superior posterior and inferior anterior. The second plane passes sagittally through the center of the maxillary sinus and divides each of the previous segments into lateral and medial parts.
Thus, two lateral and two medial segments arise:
- superoposterior external;
- superoposterior internal;
- inferoanteroexternal;
- inferoanterointernal.
Clinical observations confirm the feasibility and practical significance of the Ongren scheme, since it allows one to accurately determine the location of the tumor, since the lesion of each segment is characterized by certain clinical manifestations. Correct assessment of the symptoms of the disease allows you to timely suspect a malignant tumor and take the necessary measures. The danger hidden in delaying treatment for malignant tumors of the upper jaw is so great that it should be considered justified in all unclear and suspicious cases to resort to a comprehensive examination of the patient.
Neoplasms of the superoposterior outer segment. The main direction of growth of tumors in this localization is the pterygopalatine fossa and the orbit. Neoplasms of this group cause early exophthalmos. In this case, the eyeball shifts inwards, and diplopia appears. Obstruction of lymph and venous outflow associated with tissue germination by a tumor leads to swelling of the eyelids and narrowing of the palpebral fissure on the side of the tumor lesion. As the tumor grows further, facial asymmetry increases.
When a tumor grows into the pterygopalatine and infratemporal fossa, compression of the venous plexuses located here occurs, which impedes the outflow of venous blood and ultimately leads to lymphostasis in the retrobulbar tissue, zygomatic region and lower eyelid. This manifests itself as chemosis in combination with exophthalmos.
As they spread towards the tubercle of the upper jaw, tumors of this segment cause restriction of mouth opening due to contracture of the internal pterygoid muscle under the influence of tumor infiltration of its fibers and, in part, pressure on the coronoid process of the lower jaw branch. Tumors of the superior posteroexternal segment, earlier than other localizations, may be accompanied by the appearance of pain or paresthesia in the area of innervation of the 2nd branch of the trigeminal nerve of the corresponding side. Pain can radiate to the premolars and molars of the upper jaw. When the Eustachian tube grows, pain occurs in the ear area.
Thus, the deep location of malignant tumors of this segment under the cover of such anatomical formations as the zygomatic bone, the tubercle of the upper jaw, the ramus of the lower jaw with the surrounding muscles, leads to a long-term asymptomatic course of the disease. Only after the destruction of the upper or posterior (infratemporal) walls of the maxillary sinus and the beginning of tumor disintegration do symptoms characteristic of malignant growth appear.
Neoplasms of the inferoanteroexternal segment . They tend to spread to the area of the temporomandibular joint (TMJ), infratemporal fossa, oral cavity, and cheeks. Among the first symptoms of tumors of this localization, pain radiating to the ear should be noted, which is due to the involvement of the II and III branches of the trigeminal nerve in the process. In a later period, contracture occurs due to damage to the internal pterygoid and masticatory muscles. With a tendency to spread inward, the lateral wall of the pharynx and the palatine tonsil are affected. With outward growth, facial asymmetry appears. Invasion of the external carotid artery or its branches can lead to heavy, repeated bleeding, one of which can be fatal.
Malignant tumors of this segment do not manifest themselves for a long time; only after the walls of the maxillary sinus are destroyed, the first symptoms of malignant growth are detected, but they are late.
Neoplasms of the superoposterior internal segment . Tumors of this segment tend to spread towards the cells of the ethmoidal labyrinth and orbit (the incidence of the latter is 20-25%). Tumors of this location are also diagnosed late, because located in an area that is difficult to access for research. Infiltrating the tissue of the orbit, the tumor displaces the eyeball anteriorly and laterally, limiting its mobility. Already in the early stages of the disease, patients notice the appearance of lacrimation on the affected side. Later, swelling and hyperemia appear in the area of the inner corner of the eye due to secondary developing dacryocystitis and tumor growth into the lacrimal sac and lacrimal ducts. At this stage, visual acuity usually does not change.
When the tumor spreads towards the nasal cavity, unilateral, first mucous, then mucopurulent or sanguineous discharge appears from the corresponding nasal passage, and difficulty breathing. Sometimes nasal discharge becomes foul-smelling. During rhinoscopy, you can see bleeding tumor masses covered with purulent plaque, resembling granulations, located in the upper part of the nasal cavity. Sometimes it is possible to find out from the anamnesis that the first manifestation of the disease was a distortion or disappearance of the sense of smell, which is associated with damage to the receptor apparatus of the olfactory nerve. Headaches follow.
If the tumor spreads to the ethmoid labyrinth, then varying degrees of exophthalmos may develop with optic nerve atrophy and decreased visual acuity. Often patients are bothered by pain in the area of innervation of the 2nd branch of the trigeminal nerve. There may be a loss of skin sensitivity in the cheek area.
If the tumor tends to spread to the nasopharynx, then from there it often grows into the body of the main bone. This stage is characterized by pain radiating to the temple. Further development of the tumor process can lead to growth into the cranial cavity with the appearance of signs of damage to a number of cranial nerves (II, III, IV, V, VI). Diplopia, decreased visual acuity, neuralgic pain in the superciliary region appear, and the corneal reflex is absent.
Neoplasms of the inferoanterointernal segment . The tumor spreads into the nasal cavity of the corresponding side, as well as onto the anterior wall of the maxillary sinus and the alveolar process of the upper jaw. Tumors of this location are diagnosed relatively early. Gradually destroying the alveolar process, hard palate, and the anterior wall of the maxillary sinus, the tumor grows into the mucous membrane. Bone destruction leads to gradual loosening and loss of often intact teeth. Involvement of the nerve endings of the alveolar processes in the tumor process leads to gradually increasing pain in the teeth and jaw. The destruction of blood vessels causes bleeding gums. The alveolar process is deformed, becomes thickened, as if swollen. Tumor tissue protrudes from the sockets of fallen or removed teeth, bleeding profusely and resembling granulation tissue. When the tumor process spreads to the anterior wall of the maxillary sinus, the nasolabial fold becomes smoother and progressive facial asymmetry appears.
When it grows into the nasal cavity, difficulty or complete absence of (one-sided) nasal breathing occurs, bloody or pus-laced discharge with an unpleasant odor appears, but the sense of smell is not impaired.
Characteristics of the origin of the main symptoms of malignant neoplasms of the upper jaw
For convenience, the variety of symptoms of malignant tumors of the upper jaw can be grouped as ocular, nasal and dental.
The leading symptom of tumors in this location is pain. With primary damage to the maxillary sinus, they occur almost simultaneously with the detection of a tumor or precede the appearance of visual signs of a tumor by 1 to 6 months. They are of the most varied nature, irradiating to different areas of the head. The intensity and nature of pain depend on the type and location of the tumor and the extent of the process. With limited tumor damage, constant dull pain in the upper jaw area predominates, intensifying in a horizontal position and when tilting the head, due to a rush of blood and increased pressure on the nerve trunks. As the tumor spreads towards the alveolar process of the upper jaw, toothaches arise with irradiation to the temple and TMJ. In the later stages, painful constant headaches occur.
The occurrence of toothache often leads to diagnostic errors and interventions on intact teeth, which do not eliminate the pain.
With sarcomas of the upper jaw, pain of a very different nature is observed: dull, aching, boring. Their irradiation is the same as in cancer.
The use of thermal procedures, as well as physical therapy, leads to increased pain and accelerated tumor growth.
The persistence of pain in malignant neoplasms of the upper jaw is a characteristic feature that distinguishes them from inflammatory processes.
Nasal symptoms . In most patients, as the malignant tumor grows, unilateral progressive difficulty breathing is observed until it is completely absent. Discharges of various types appear: mucous, bloody, fetid-purulent. In the early stages, reactive inflammation of the mucous membrane of the maxillary cavity around the focus of tumor growth is observed, which leads to irritation and hypersecretion of the epithelium of the mucous membrane. The transparent mucous discharge from the maxillary cavity enters the nasal cavity through the natural opening in the middle meatus. Patients, as a rule, believe that this is the result of a cold and do not consult a doctor, using vasoconstrictor nasal drops or thermal procedures at home. Subsequently, the secretion becomes purulent due to the addition of a secondary infection. Putrid discharge mixed with blood indicates an advanced process, accompanied by the disintegration of the tumor.
It has been noticed that fetid purulent discharge from the nose is more characteristic of cancer, and putrefactive discharge with streaks of blood is more characteristic of sarcoma of the upper jaw.
Difficulty in nasal breathing . It occurs due to the fact that the tumor, having completely filled the maxillary sinus, displaces its medial wall towards the nasal septum, and in later stages grows into the medial wall of the maxillary sinus, fills the middle and lower nasal passages, displaces and then grows into the nasal septum. At this stage, in addition to copious mucous discharge, nosebleeds appear from the growing tumor tissue. The tumor masses, having filled the nasal passages, protrude from the nasal opening. In the later stages of the disease, the nose shifts to the healthy side.
Difficulty opening the mouth . Contracture is rarely observed in the early stages of the tumor process in the upper jaw. The appearance of this symptom is associated with the tumor growing into the pterygoid, masseter or temporal muscles, i.e., when the tumor has already spread beyond the maxillary sinus. This symptom is typical for tumors located in the posterior sinus near the TMJ. When a tumor grows into a joint, first a reactive inflammation occurs in it, and then the tumor directly grows into it. In addition to contracture, pain in the joint is observed, which intensifies while eating and talking.
Ophthalmological symptoms . Pathological changes in the area of the eyelids, orbit and eyeball often indicate the presence of a malignant tumor of the upper jaw. Observed: unilateral lacrimation, swelling of the eyelids and narrowing of the palpebral fissure, exophthalmos or displacement of the eyeball in various directions, limitation of its mobility, diplopia, decreased visual acuity.
Swelling of the eyelids - occurs as a result of tumor spreading into the eye socket. Due to compression of the blood and lymph outflow pathways, lymphostasis occurs. Swelling can occur due to inflammatory changes of a reactive nature in adjacent soft tissues. Swelling of the lower eyelid causes a narrowing of the palpebral fissure and its upward displacement. When the tumor spreads towards the nasolacrimal duct, one-sided profuse lacrimation is observed.
As the tumor grows towards the orbit, the contours of its lower wall are disrupted. The orbital margin first becomes dense, lumpy, and later areas of softening appear. Almost simultaneously, swelling of the orbital tissue increases, and purulent conjunctivitis develops. Sometimes malignant tumors of the maxillary sinus first spread to the ethmoidal labyrinth and then grow into the orbit, which leads to displacement of the eyeball. The direction of displacement depends on the location and preferred direction of tumor growth. With sarcomas, displacement of the eyeball is observed earlier than with cancer.
The early stages of exophthalmos are usually detected not by the patient himself, but by those around him. Severe exophthalmos leads to impaired closure of the eyelids. Displacement of the eyeball to one side or another causes diplopia. With direct exophthalmos, diplopia does not occur. When the lower wall of the orbit is destroyed, enophthalmos (retraction of the eyeball) is formed.
If a malignant tumor grows into the motor muscles of the eyeball, its mobility is limited and vision is impaired. Tumor infiltration of the eyeball or optic nerve leads first to partial and then complete loss of vision.
Metastasis of malignant tumors of the upper jaw occurs mainly through the lymphogenous route. With sarcomas, hematogenous spread is possible. The outflow of lymph from the paranasal sinuses and upper jaw is carried out into the retropharyngeal and upper deep cervical lymph nodes. From the anterior sections, lymph flows into the submandibular lymph nodes.
Regional metastasis of malignant tumors of the upper jaw is a fairly rare phenomenon. With the upper internal localization of cancer, it was observed in 7.3%, lower - in 14.9% (Paches A.I., 1983). According to Yu.I. Vorobyov, the frequency of regional metastasis of tumors of this localization is generally 21.4%, and poorly differentiated and undifferentiated forms of cancer metastasize more often than differentiated forms of squamous cell carcinoma.
Distant metastases are observed from 3.4 to 9%.
The general condition of patients with malignant tumors of the upper jaw in the early stages may not be affected. But during the period of tumor imaging, a progressive decrease in body weight is usually observed. This can be expressed to varying degrees and depends not only on the stage of the tumor process, but also on the location, growth rate and spread. Thus, with the appearance of early contracture and pain in the TMJ area, weight loss begins earlier and is nutritional in nature due to difficulty eating. During the period of tumor disintegration and the addition of a secondary infection, patients experience symptoms of anemia due to intoxication from the disintegrating tumor, as well as repeated bleeding. Simultaneously with a decrease in the percentage of hemoglobin, the number of erythrocytes progressively decreases, the number of leukocytes increases, and the ESR sharply accelerates.
In the later stages of the disease, aniso- and poikilocytosis is observed. In the peripheral blood formula, as a rule, there are no sharp changes, only sometimes there is a slight decrease in lymphocytes and an increase in rod-nuclear leukocytes.
The skin of patients is characterized by increasing pallor. In later stages, the skin becomes sallow gray with a jaundiced tint. Many patients complain of general weakness, fatigue, a sharp decrease in appetite, and inability to work.
Operation
When reconstructing the lower jaw, a flap from the leg is usually used - the fibular flap. The operation is planned on a computer: the surgeon determines how to correctly select the flap, how to remove the tumor, and how to implant the flap.
Computer-aided planning of mandibular reconstruction
If the patient plans to install dental implants, then an implant surgeon is involved in planning and performing the operation. Tumor removal, reconstruction and implantation are performed in one operation.
Without nutrition, the transplanted flap dies. To avoid this, the feeding vessels of the flap must be sewn into the bloodstream. Since the feeding vessels are very small and fragile (less than a millimeter in diameter), to work with them the surgeon must have microsurgical equipment - be able to suture microscopic vessels under a microscope so that they do not bleed or become clogged.
What causes complications?
Negative consequences often arise either due to medical error or the fault of the patient during rehabilitation. Causes of resection complications:
- Late filling. This procedure is carried out 1-2 days before the apexectomy, otherwise there is a risk of inflammation occurring after the operation as a negative reaction.
- Poor quality filling. The canals inside the tooth must be sealed, otherwise an inflammatory process will occur if the infection continues to spread.
- Tooth decay. If the treatment is handled incorrectly during surgery, there is a risk of damage to the tooth, which will lead to its loss.
- Unprofessionalism. Sometimes serious damage during surgery is caused by the doctor due to improper use of the instrument or careless handling of it.
- Incomplete resection. If the inflamed tissue and source of infection are not completely removed, then a recurrence of the cyst is possible in the future.
- Tissue infection occurs during surgery due to incomplete sterility or after improper oral care.
- Root destruction. The operation involves removing only the tip of the root, a minimal part of it, but if the dentist makes a mistake, the root can completely collapse, causing the tooth to become loose.
- Failure of the patient to comply with postoperative appointments. Proper care, lack of physical activity, diet and other medical prescriptions speed up the rehabilitation process.
Contraindications for tooth root resection
The operation of resection of the apex of the tooth root is not performed:
- If the patient has a disease such as periodontal disease, which has led to exposure of the neck or root of the tooth;
- If severe tooth mobility is detected;
- For acute periodontitis;
- In case of severe destruction of a diseased tooth;
- In case of an inflammatory process that has damaged most of the root system of the tooth.
The operation of tooth root resection is not prescribed for patients suffering from severe pathologies of the cardiovascular system; other surgical techniques are chosen to remove cysts and granulomas larger than 10 millimeters in size.
Before such a serious and complex operation as resection of the apex of a tooth root, a thorough and high-quality diagnosis is essential, helping to eliminate all possible contraindications to the technique. In our dentistry "Firadent", the highest attention is always paid to the quality of patient diagnostics; all activities are carried out using modern and ultra-precise equipment.
Resection of the apex of the tooth root is an operation carried out in four successive stages, and below we will tell you in detail about all stages of the treatment process.
Removal of upper teeth
The bone of the upper jaw is somewhat softer than the lower jaw.
The units are positioned straighter and are easier for the surgeon to grasp. Therefore, removal of the upper molar in many cases is faster and less painful. Patients are often frustrated by the need to have their front teeth removed. The smile zone is always visible, so the absence of one brings a negative attitude and leads to a decrease in self-esteem. But today such an operation is not scary. There are every opportunity to quickly restore the integrity of the dentition.
Removing the front tooth on the upper jaw is simple - it has only one cone-shaped root and is located conveniently for manipulation. The operation will take about 20 minutes, including waiting for the anesthesia to take effect. If there are no contraindications, then simultaneous implantation is recommended - the destroyed unit is removed and an artificial root is immediately installed in the same hole.
Our clinics employ implantologists who are proficient in advanced techniques and have completed internships in foreign clinics. Only premium implants are used. Therefore, you will quickly gain a new beautiful smile. It is possible to install a temporary plastic crown on the pin on the day of removal. The front teeth will be in place, and no one will notice the changes.
Treatment from world-class doctors cannot be cheap, but we have found an opportunity to make help accessible - we treat immediately, and offer to pay for services in installments in convenient amounts, without charging interest.
Removing the upper root of a tooth is a more complex process. The root branch is drilled into several parts, which are removed step by step. This procedure for intervention is typical for molars and wisdom teeth, when the walls have completely crumbled and the root is also not viable.
Symptoms
Exostosis of the tooth appears in the form of a convex growth that appears for no apparent reason. Main symptoms:
- Sensation of a foreign body in the mouth;
- discomfort when eating, talking (with large osteophytes);
- pain when pressing on the tumor;
- redness, thinning of the mucous membrane in the pathological area.
A small anomaly can only be detected during a dental examination, since visually it does not manifest itself in any way.