This is an acute purulent inflammation of soft tissues and/or internal organs (mediastinum, abdominal cavity, retroperitoneal space, pelvis, etc.).
The name comes from a Greek word meaning inflammation or swelling. Cellulitis can affect internal organs such as the appendix, kidneys, liver, spleen, intestinal vessels, prostate gland, pancreas, or anywhere under the skin. It tends to spread quickly and in some cases can be life-threatening.
General information
What is phlegmon?
Phlegmon (phlegmona) is an acute purulent-necrotic diffuse process that develops in the subcutaneous, interfascial, intermuscular, perivascular/perineural fatty tissue with a tendency to spread. Cellulitis code according to ICD 10: L03. A characteristic feature of phlegmon that distinguishes it from an abscess is the absence of clear boundaries (the absence of a pyogenic membrane from a layer of fibrous fibers/granulation tissue), which contributes to the rapid/extensive spread of the purulent process through the cellular spaces with transition to tendons, muscles, bones and other structures. Cellulitis and abscess can develop as a complication of other purulent processes ( carbuncle , abscess , sepsis ), or be an independent disease. As a rule, phlegmon is localized in those areas where there are sufficient cellular spaces filled with adipose tissue. In general, phlegmons are divided into superficial (subcutaneous/epifascial) and deep (subfascial), however, a number of authors among subfascial phlegmons separately distinguish phlegmons of various cellular spaces, which have special names, for example, paranephritis (phlegmon of the perirenal cellular tissue), mediastinitis (phlegmon of the mediastinal cellular tissue), paraproctitis (phlegmon of peri-rectal tissue), etc. Phlegmon can be an independent disease or a complication of other purulent processes.
Diagnostics
Peritoneal phlegmon is an extremely dangerous disease that requires immediate treatment in a hospital setting. The sooner it is detected, the greater the patient's chances of survival. Types of tests used to diagnose inflammation:
- surgical examination;
- blood analysis;
- Ultrasound of the abdominal cavity and retroperitoneal space;
- radiography;
- computed tomography (CT) of the retroperitoneum.
To make an accurate diagnosis, doctors resort to the differential method. At the initial stage, the pathology has similar symptoms to spinal osteochondrosis and protrusion of the vertebral discs. In the presence of infiltrate, the clinical picture of phlegmon resembles influenza, typhoid, paratyphoid, pyelonephritis and osteomyelitis of the pelvic bones. The latter can accompany inflammation and cause the spread of pus.
Pathogenesis
The pathogenesis of phlegmon is determined by the type of pathogen, the place of its penetration into the body and the reaction of the macroorganism to its penetration. The development and course of phlegmon depends on the concentration of microflora at the entrance gate, the anatomical and topographical characteristics of the tissues, the state of the organs and systems of the body, as well as general/local specific nonspecific protective factors, which determine the nature of the inflammatory reaction.
Penetration and reproduction of the pathogen causes a tissue reaction in the form of exudative inflammation, that is, serous infiltration , but the exudate very quickly becomes purulent in nature. The following stages of the pathological process are distinguished: edema, tissue infiltration, purulent melting, necrosis. In cases of phlegmon, there is no restriction of the purulent focus with the formation of a granulation shaft.
Development mechanism
When an infection enters the subcutaneous environment, inflammation rapidly develops. The high intensity of the pathological process is explained by several factors.
These include:
- Rapid development of intoxication;
- Lack of an adequate immune response of the body;
- Decreased local immunity;
- The presence of optimal conditions for the growth of bacteria.
Due to the rapid development, granulation tissue does not have time to form, which should protect the source of inflammation from healthy tissue. Therefore, the pathological process spreads quickly.
Classification
The classification of phlegmon is based on several characteristics, according to which the following types of phlegmon are distinguished.
- Along the way: acute and chronic phlegmon.
- By location: superficial (the pathological process affects tissues up to the muscle layer) and deep (the pathological process affects tissues deeper than the muscle layer, fatty tissue).
- According to the nature of the exudate: serous-purulent phlegmon , purulent , purulent-hemorrhagic phlegmon and putrefactive .
- By localization: subcutaneous, intermuscular, subfascial, interorgan, organ, retroperitoneal, pelvic, phlegmon of the hand and foot, phlegmon of the neck, phlegmon of the maxillofacial region, phlegmon of the armpit, etc.
- By origin: primary (develops when the pathogen enters the tissues of the body directly) and secondary (occurs when pathogens migrate from other purulent areas).
Possible complications and consequences
In rare cases, after surgery, phlegmon forms again in the retroperitoneal space. This occurs due to violation of sanitation standards during the intervention, improper execution of the procedure or weakened immunity. To re-clean, the sutures are removed, purulent contents are removed and the incision is sutured.
Prevention of subsequent accumulation of infiltrate consists of a course of vitamins and restoratives. The drugs help increase the body's protective properties and help it actively fight harmful microorganisms.
Causes
The etiological factor is predominantly staphylococcus, streptococcus, Proteus, Escherichia coli, anaerobic microflora. In cases where phlegmon develops as a complication of some other purulent disease, the spread of the infectious process occurs from the immediate primary focus through the fascial sheaths and various natural openings or by the lymphogenous/hematogenous route.
The occurrence of phlegmon and its more severe course is facilitated by a decrease in the protective functions of the body, caused by immunodeficiency states, chronic diseases ( tuberculosis , diabetes mellitus , blood diseases, exhaustion), chronic intoxication ( alcoholism ).
Symptoms
The general symptoms of phlegmon are due to the phenomena of intoxication, and taking into account the extensiveness of the process, the symptoms of intoxication are usually very pronounced and are manifested by severe weakness, chills , thirst , headache , and a rapid increase in temperature to 39-40°C. At the same time, deep phlegmons are characterized by more pronounced severity and earlier appearance of general symptoms. The condition quickly worsens, a decrease in blood pressure, shortness of breath , a frequent weak pulse, a decrease in urination, jaundice of the skin and cyanosis of the extremities appear. With superficial phlegmon, redness and swelling appear in the affected area, an increase in regional lymph nodes is noted, and with phlegmon of the extremities, they increase in volume.
Upon palpation of phlegmon, a motionless, sharply painful, hot-to-the-touch formation with glossy skin above it, which has no clear boundaries, is noted. Movement is painful, and the pain increases with changes in body position. Subsequently, soft tissue softens in the area of inflammation and a purulent cavity is formed, pus from which can either break out to form a fistula or spread to adjacent tissues, causing an inflammatory process. Acute phlegmon is characterized by rapid progress, accompanied by the involvement of new areas of fatty tissue and anatomical formations located nearby in the pathological process, which is accompanied by severe intoxication.
Each of the forms of phlegmon (depending on the nature of the exudate) has its own specific course:
- Serous phlegmon . It is characteristic of the initial period of phlegmon development, in which serous inflammation predominates: exudate accumulates in the area of localization of the pathological process, while leukocytes infiltrate the fatty tissue cells. Accordingly, the fiber is saturated with a turbid, watery liquid and acquires a gelatinous appearance, and the border (pyogenic membrane) between healthy and diseased tissues is practically absent. The serous form can transform into purulent/putrefactive phlegmon. The general condition suffers slightly.
- Purulent phlegmon . It is formed as a result of the melting of tissue with the gradual formation of pus ( histolysis ) with the formation of a whitish-yellow-green cloudy exudate. With this form of phlegmon, as a result of tissue melting, frequent formation of fistulas, ulcers and cavities is observed, as well as the spread of a purulent-inflammatory process to adjacent tissues and structures. Purulent phlegmon is characterized by an acute onset, chills, a sudden increase in body temperature to high levels, and protective (painful) muscle contracture.
- Putrid phlegmon . There is tissue destruction in the area where the process is localized with the formation of gases that have an unpleasant odor. With such phlegmon, the tissues acquire a dark green/dirty brown color, become loose and quickly collapse, transforming into a semi-liquid mass. As a result of intense putrefactive decay of tissues, severe intoxication develops: chills, a sharp increase in body temperature, a decrease/fall in blood pressure. Putrid infection spreads much faster than purulent infection and is accompanied by lymphangitis / lymphadenitis .
- Necrotic phlegmon . It is manifested by the formation of many foci of necrosis, which either subsequently melt or are rejected, forming a wound surface. The general condition suffers, accompanied by chills and high fever. In cases of a favorable course, the inflammation zone is limited to the leukocyte shaft and the granulation barrier from healthy tissues surrounding the phlegmon, that is, the process is localized with the formation of abscesses, which can later open independently or be drained surgically.
- Anaerobic phlegmon . Caused by non-spore-forming anaerobes. Characterized by a widespread serous inflammatory process with the rapid formation of large areas of tissue necrosis, accompanied by the release of gas bubbles from the tissues with a foul odor. When palpating such phlegmons, a soft crunching sound (crepitus) is detected, due to the presence of gas. Accompanied by severe intoxication and severe general condition of the patient.
Let's consider the general and local manifestations of phlegmon depending on its location.
Phlegmon of the upper extremities
Cellulitis of the hand is most common on the upper extremities . Cellulitis of thenar (elevation at the base of the thumb)/hypotenary is distinguished supra- subgaleal phlegmon of the median palmar space; U-shaped (cross cellulitis); commissural phlegmon (in the distal part of the palm); supra- subgaleal phlegmon of the dorsum of the hand.
Cellulitis of the thenar area - patients complain of swelling, pain and redness of the skin in the thenar area. When palpating this area, there is sharp pain, and movements in the first finger are also painful. Among the common manifestations is low-grade body temperature.
Phlegmon of the hypothenar - manifested by pain and tissue tension on palpation, moderate swelling, hyperemia. The pain intensifies with movement of the fifth finger. There are no signs of severe intoxication.
Commissural phlegmon - most often develops when cracks in the callused/rough skin of the palm appear in the area of the metacarpophalangeal joints. The inflammatory focus is localized in the commissural spaces of 2-5 fingers. Swelling of the distal part of the two surfaces of the hand and severe pain are characteristic; the fingers located adjacent to the purulent focus are bent at the interphalangeal joints and slightly separated, and their extension is painful due to the tension of the inflamed aponeurosis of the palm.
Phlegmon of the middle space . The skin of the central part of the palm bulges, is tense, and is sharply painful on palpation. The swelling is especially pronounced on the dorsum of the hand. A significant increase in pain is caused by an attempt to actively/passively extend 2-5 fingers. If treatment is delayed, they may be complicated by the breakthrough of purulent contents into the thenar fissure. The inflammatory process is accompanied by headaches, increased body temperature, and changes in the peripheral white blood.
U-shaped cellulitis . Refers to the most severe form of phlegmon of the hand. Represents a joint lesion of the ulnar/radial synovial bursae of the palm. The fingers are slightly brought towards the palm, active/passive movements significantly increase the pain. On palpation, severe pain in the proximal part of the hand and in the projection area of the flexor tendons of the 1st and 5th fingers. Accompanied by severe intoxication (general weakness, headache, high body temperature). It is particularly dangerous due to the high risk of spread of the purulent-inflammatory process to the entire cellular and fascial space of the hand.
Subcutaneous phlegmon . Subcutaneous phlegmon of the dorsal surface is the mildest form of phlegmon of the hand. Hyperemia and tissue edema are diffuse in nature and it is difficult to establish the boundaries of the purulent focus. The general condition is practically not affected.
Subgaleal phlegmon . On palpation, diffuse tenderness of a denser infiltrate is determined, accompanied by hyperemia/edema of the dorsum of the hand. Symptoms of intoxication may be present.
Phlegmons of the lower extremities (phlegmons of the thigh, lower leg, foot, popliteal fossa)
Thigh phlegmon - superficial phlegmon of the thigh with localization in the femoral triangle is accompanied by a high risk of spread of a purulent inflammatory process through the deep intermuscular spaces/lymphatic ducts and through the superficial fascia with the formation of deep phlegmon of the thigh.
Phlegmon of the leg . They are localized mainly in the anterior, posterior and external fascial bed. Deep phlegmon of the thigh and lower leg is characterized by general symptoms in the form of chills, lethargy, loss of appetite, general weakness, diffuse pain at the site of localization and an increase in body temperature to high numbers, enlargement and soreness of nearby lymph nodes. The onset is acute and rapid development is characteristic. Locally: swelling and tension of tissues (skin.) As a result of disruption of venous outflow, the limb significantly increases in volume. With superficial phlegmon, swelling and hyperemia of the skin, as well as a symptom of fluctuation, can be noted.
Phlegmon of the popliteal fossa . In most cases, this is adenophlegmon, since their source is inflammation of the popliteal lymph nodes with the formation of pus. Adenophlegmons of the popliteal fossa usually arise as a result of festering wounds in the area of the Achilles tendon/posterior part of the heel area. Palpation shows a local increase in temperature, a softening area is palpated. The function of bending the leg at the knee joint suffers, the limb takes on a forced position and the pain intensifies with movement.
Phlegmon of the foot . Most often, phlegmon of the foot occurs when injuries to the sole penetrate through the aponeurosis (deep subaponeurotic phlegmon). At the same time, the process often involves the digital phalanges, metatarsal bones and joints of the foot with the development of purulent arthritis and osteomyelitis of the bones of the foot. It manifests itself as sharp pain when stepping on the foot, swelling, and pain on palpation. The general condition suffers. Dorsal subfascial phlegmons of the foot are localized in the cellular space between the dorsal and intrinsic muscular fascia of the feet. They manifest themselves as swelling at the site of localization, hyperemia and pain when pressed.
Cellulitis of the neck . Neck phlegmon is a serious illness that requires immediate hospitalization. Below is a photo of neck cellulitis.
Superficial phlegmons of the neck are predominantly localized above the deep fascia of the neck in the submandibular/mental areas and, due to their superficial location and easy accessibility for surgical intervention, do not pose a great danger.
Clinically, they are manifested by general malaise, headaches, and increased body temperature to 38-40°C. In the blood there is leukocytosis and a shift to the left of the leukocyte formula. If not treated adequately/timely, they may spread to the face.
Putrefactive-necrotic phlegmon of the face and neck is especially dangerous. More often, the infectious process spreads from the oral cavity ( pharyngitis , laryngitis , dental caries ).
Deep phlegmon of the neck is the most dangerous disease, since necrotic processes can spread into the mediastinal tissue with the subsequent development of mediastinitis . Due to the lack of clear diagnostic signs of the disease, since the focus is localized under the deep fascia of the neck and diagnosis of deep phlegmon of the neck is often difficult.
Facial phlegmon
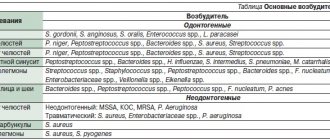
Phlegmons of the maxillofacial area can be conditionally divided into two groups depending on the source of their occurrence: odontogenic ( the main cause of periodontal disease, bone tissue of the hard tissues of the tooth) and non-odontogenic (caused by tissue infection as a result of mechanical trauma, tonsillitis , rhinitis , otitis ) . Depending on the location of phlegmon, they are distinguished:
- Phlegmon with localization near the upper jaw, in which the structures of the eye are involved in the pathological process (phlegmon of the orbit of the orbit, phlegmon, phlegmon of the temporal, infratemporal, orbital region, phlegmon of the lacrimal sac or eyelid, hard/soft palate).
- Phlegmons localized near the lower jaw (adenophlegmon of the submandibular region, chin, submandibular region - peripharyngeal, mandibular submasseterial space, parotid salivary gland, etc.)
- Phlegmon of the upper/lower sections of the floor of the mouth (phlegmon of the tongue, sublingual region, phlegmon/abscess of the maxillo-lingual groove, diffuse phlegmon of the floor of the mouth, etc.).
General clinical manifestations and phlegmon of the maxillofacial area include the phenomenon of severe intoxication (loss of appetite, general weakness, chills, sweating, increased breathing/pulse), changes in peripheral blood, impaired thermoregulation (increase in temperature to 39-40 ° C); phenomena of toxic nephritis .
The local inflammatory reaction manifests itself in the form of hyperemia, infiltration and edema at the site of phlegmon localization. Characteristic is impaired mobility of the lower jaw to one degree or another, up to the development of inflammatory contracture, impaired salivation, disorder of articulation, speech, and, less often, breathing, severe pain/disturbance in the act of chewing. The diversity of the clinical picture is determined by the localization of phlegmon and its prevalence (in one/two or three cellular spaces). Common phlegmons are characterized by a rapidly progressing severe course, and endogenous intoxication increases as the volume of the purulent process increases.
Chronic phlegmon develops with high resistance of the patient's body against the background of microflora with low virulence and is accompanied by the formation of a dense, woody infiltrate.
Diagnostic procedures
The diagnosis is made on the basis of anamnesis and external examination of the patient. The presence of acute or chronic infectious diseases is taken into account. Auxiliary diagnostic procedures are prescribed to determine the severity of the pathology.
During diagnosis, it is extremely important to determine the type of infection that provokes the pathology. This will allow further effective antibacterial treatment.
To determine the type of pathogen, a puncture biopsy is performed, during which purulent contents are collected, which are further studied in the laboratory.
Cellulitis in children
Cellulitis in children is a fairly common occurrence, which is due to frequent household trauma to the skin. Cellulitis of newborns is of particular importance. The penetration of infection through the skin of newborns is facilitated by its damage, violation of aseptic rules during medical procedures and when caring for the child. Cellulitis in newborns is often caused by staphylococcal infection . Inflammation initially occurs around the sweat glands, and then spreads deep into the skin and subcutaneous fat, followed by the development of necrosis , which is facilitated by the production of hyaluronidase by staphylococci, which increases the permeability of connective tissue.
Clinically, a limited area of hyperemia with a diameter of up to 2 cm initially appears on the skin, which within a few hours quickly increases in diameter like an “oil stain”; at the same time, infiltration and swelling appear in the affected area. After 1-2 days, a focus of softening appears in the center of the extensive hyperemia with clear edges, and starting from the 3rd day, small fistulous tracts with serous-purulent discharge are formed. On the 5-7th day, rejection of the anesthetized areas begins, thereby forming a wound defect. Next, necrosis can spread to deeper tissues.
After 1.5-2 weeks, necrotic tissue is rejected, inflammatory phenomena subside, and granulations form in the wound. The most common places for its formation include the surfaces of the chest, lower back, sacral area, and less often - on the buttocks and limbs. Clinically, a toxic-septic form of phlegmon is distinguished, in which the general condition of the child initially suffers. Phlegmon manifests itself rapidly, starting with symptoms of intoxication: the child is restless and then becomes lethargic, refuses to breastfeed, vomiting is possible, febrile fever appears, heart sounds are muffled, the skin has a grayish tint, diarrhea with the rapid development of the phenomenon of exicosis .
In the simple form, a subacute onset is noted: initially pallor appears, appetite decreases, and body temperature gradually increases. The child develops anxiety almost from the first hours of illness. Local manifestations progress faster than the general condition. A characteristic sign is the presence of a swollen, rapidly spreading area of soft tissue with signs of fluctuation and a cyanotic reddish color of the skin over them.
The child needs to be hospitalized in the neonatal surgery department. Drug treatment in the initial stage includes the prescription of antibacterial drugs: Oxacillin IV + Clindamycin in age-appropriate dosages. If there is resistance to oxacillin, Vancomycin or Linezolid . In severe cases, aminoglycosides ( Amikacin ) are recommended. Locally, it is recommended to apply bandages to the affected area with Levomekol . If there is no effect, the phlegmon is opened, drained and a bandage is applied.
Treatment
The nature of therapeutic procedures depends on the severity of phlegmon and its location. The pathology is potentially life-threatening, and therefore requires hospitalization of the patient.
Drug therapy
Treatment involves taking medications in strict accordance with the dosages prescribed by the doctor.
The following groups of drugs are used:
- Treatment involves taking medications in strict accordance with the dosages prescribed by the doctor.
Antibiotics. The action is aimed at destroying pathogenic microflora, thereby stopping the development of inflammation. Antibacterial therapy is most effective at an early stage, before tumor formation. In later stages, antibiotics are used as an adjuvant. Patients are prescribed intramuscular injections of Erythromycin, Cefuroxime and Gentamicin. On average, the duration of therapy is 3-5 days.
- Anti-inflammatory drugs. They are used to reduce tissue swelling, eliminate hyperemia, and pain. Medicines are prescribed by a doctor taking into account pharmacological interactions with antibiotics. In most cases, drugs based on Diclofenac and Nimesulide are used.
- Local antiseptics. Used for local treatment of phlegmon, which is required in the formation of a purulent fistula. For disinfection, a solution of chlorhexidine, Furacilin, and less commonly Boric acid and hydrogen peroxide are used.
Surgery
The operation can be performed during planned treatment or urgently, if the patient’s condition worsens.
Purulent phlegmon is treated surgically. The operation can be performed during planned treatment or urgently, if the patient’s condition worsens.
The presented treatment option is considered more preferable than drug therapy, as it eliminates the risk of complications and re-development of the pathology.
The main indication for surgery is the presence of an inflammatory focus and elevated body temperature of the patient.
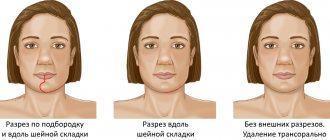
The procedure is performed under general anesthesia. The phlegmon is opened with a wide incision, which allows for the outflow of purulent substance.
After the pus is released, the affected area is washed and disinfected. Bandages containing antibacterial ointments are applied to the incision. If the skin does not heal well, dermoplasty is performed.
Physiotherapy
The use of physiotherapeutic procedures is considered appropriate only at the early stage of pathology. Physiotherapy methods can also be used for symptomatic treatment.
Basic methods:
- UHF therapy;
- Ultraviolet irradiation;
- Light therapy;
- Ultrasonic treatment of opened phlegmon;
- Laser treatment of the wound.
Alternative medicine
Traditional methods are not recommended for use in acute illness. The use of unconventional methods is possible during the period of postoperative rehabilitation.
For better healing of affected skin, it is recommended to apply sea buckthorn or rosehip oil. For general strengthening of the body, medicines made from the herbs Eleutherococcus, Chinese magnolia vine, ginseng, and rose hips are used.
List of sources
- Fomichev E.V., Robustova T.G. Diagnosis and treatment of atypically current purulent-inflammatory diseases of the maxillofacial area. Russian dental journal. 2003; 4: 18-20.
- Purulent-inflammatory diseases of the head and neck. Etiology, pathogenesis, clinical picture, treatment. /Ed. MM. Solovyova, O.P. Bolshakova, D.V. Galetsky - M., MEDpress-inform., 2016.
- Abscesses, phlegmons of the head and neck. / Ed. Solovyova M.M., Bolshakova O.P. - St. Petersburg: KN, 1997.
- Fedorov V.D., Svetukhin A.A. Selected course of lectures on purulent surgery. M. 2007. 365 p.
- Gostshtsev V.K. Guide to purulent surgery. M.: Medicine, 1996, - 300 p.