Obliteration - the word comes from the Latin “Obliteratio” (destruction).
In dentistry, this term refers to a pathological process during which the cavity or the entire root canal of a tooth begins to narrow or completely overgrow. As a result, it is less resistant to infections and more difficult to respond to endodontic treatment.
Dentists name several main causes of obliteration:
- Overgrowth of connective tissue, which leads to thickening of the walls.
- The presence of inflammatory processes,
- The presence of cancer, during which tumor growth occurs.
- Body changes associated with age.
- Consequences of poor quality treatment.
There are also several factors that lead to the accumulation of calcium salts in the tooth cavity. After which the patency of the tooth pulp and root canal is impaired.
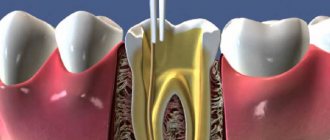
What are root canals
The dental nerve, or pulp, is located not only inside the tooth, its crown, but also inside the roots. Root canals are elongated cavities located inside the roots of teeth. This is where the dental nerve passes within the root. The number of root canals in one root may vary. There may be two or more channels in one root. The root canal can be very thin, thinner than a human hair, so high-quality treatment can take quite a long time. The difficulty is that even with the use of modern microscopes, the doctor cannot see absolutely all parts of the root canal. Work in the deepest part of the root is carried out almost blindly, which requires experience and skill from the doctor.
New technologies for problematic channels
Pulpitis and periodontitis are still the main reasons for tooth extraction. Teeth with elements of destruction at the root apex are foci of chronic infection, sometimes leading to systemic diseases. Many authors attribute the presence of additional unopened canals and great difficulties in monitoring the passage of the canal and its filling as reasons for the low quality of canal sanitation. Back in 1970, Mayer presented reconstructed models of tooth roots, which show how many lateral branches a root canal can have and how extensive the apical delta can be (Fig. 1).
Currently, more and more supporters are gaining the point of view that modern instrumental-mechanical endodontics is fundamentally unable to solve the problems of combating root infection.
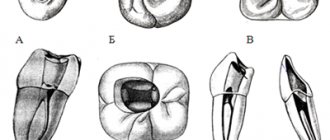
Fig. 1 Variants of the apical delta of root canals
Fig. 2 Cross sections of teeth showing difficult canals
By measuring electrical conductivity with the main hole well open and carefully insulated with varnish prof. A. Knappvost revealed that 70-90% of the flow of substances entering the pulp passes through the lateral (!) canals of the apical delta. The work of Noldin (1994) shows the shapes of channels that are poorly accessible to mechanical instruments (Fig. 2).
At the same time, only complete sterility of the entire canal system is a prerequisite for effective sanitation.
Based on the previously known methods of electrophoresis and iontophoresis of Prof. A. Knappvost has developed a technology for successfully resolving endodontic problems using a unique technology of depophoresis of a substance new to dentists - an aqueous suspension of copper-calcium hydroxide, which has exceptional bactericidal and physicochemical properties.
During treatment under the influence of an electric field, from the depot of the above-mentioned suspension created in the root canal, OH-ions and hydroxycuprate ions [Cu(OH)], which have a strong bactericidal effect, penetrate into the entire canal system, including secondary and lateral canals, up to the openings.
As a result of this, the following processes occur that underlie the therapeutic effect of electrophoresis:
- Proteolysis of biological tissue residues located in the canal system. (Professor A. Knappvost speaks of sterile oligopeptides and saponification mycelia, which, after leaving the canal system, are resorbed by the body).
- Killing remaining microorganisms by removing sulfur from amino acids. Fig. 3 At the apexes of the roots, copper “plugs” are clearly visible, tightly obliterating all exits of the apical delta to the cement surface
- Lining the unfilled part of the root canal, as well as all microcanals, with copper-calcium hydroxide, which ensures long-term sterility and also stimulates the formation of bone tissue in the area of microholes (Fig. 3).
- Stimulation of osteoblast activity in the periapical region as a result of alkalization.
Clinical practice
This method is suitable for the treatment of all gangrenous teeth. Especially for difficult-to-reach, partially obliterated and/or severely curved canals, the depophoresis method is the preferred and sometimes the only feasible alternative to traditional methods. After trephination of the tooth, the pulp chamber is opened in the usual way and the orifices of the canals are exposed. The canal is prepared over up to 2/3 of the length, and a width of ISO 35-50 is quite sufficient. It is advisable to expand the channel in the third closest to the mouth a little more in order to create a sufficient depot of the copper-calcium hydroxide suspension. We use the “Original II” device (Fig. 4). A negative needle electrode is inserted into the canal to a depth of 4-8 mm. (The electrode is not secured with any sticky wax.) The positive electrode is placed behind the cheek on the opposite side so that it does not touch the dentition. To reliably ensure the distance and for better conductivity, place a damp cotton swab between the electrode and the cheek. It is recommended to lubricate the corner of the patient's mouth with Vaseline. (The procedure is not performed in a physiotherapy room, but in the doctor’s chair).
Fig.4 Appearance of the “Original-11” device
Turn on the device and slowly increase the current until the patient signals, for example with his hand, that a feeling of warmth or tingling appears in the root area. (This is agreed upon with the patient in advance).
The current is reduced and increased again even more slowly, usually reaching 1 to 2 milliamps (mA). The session lasts 2-5 minutes. The required amount of electricity received by the patient is 5 mA X min.
Using the described method, you should influence each channel separately. During the procedure, bubbles are released from copper-calcium hydroxide into the cavity, which, especially if the tooth is covered with a crown, must be removed from time to time with a swab to avoid the discharge of electric current. Care should be taken that during depophoresis the needle electrode does not come into contact with the metal edge of the crown or filling. This will relieve the patient from unpleasant effects.
Finally, the channels and cavity are washed with distilled water or a 10% suspension of simple calcium hydroxide, but a diluted suspension of copper-calcium hydroxide itself can also be used).
As a tab until the next session, which is usually carried out after 8-10 days, after drying the canal, a fresh portion of copper-calcium hydroxide paste is injected. In most cases, three treatment sessions are sufficient to ensure treatment success. The patient must receive a total amount of electricity per channel (that is, the product of mA X minutes) equal to 15. After the last procedure, the entrance to the channel is filled with atatasamite, a special cement included in the kit (alkaline, copper-containing material). The rest of the canal (up to 1/3 of the apical part) is not filled with anything at all.!!)
Steps demonstrating gradual sterilization of canals
PSHa time between treatment sessions, according to the recommendations of prof. A. Knappvost, the cavity can be left open to prevent the development of pressure during the outflow of the still formed exudate. Recontamination is practically excluded due to the powerful disinfectant activity of medicalcium hydroxide.
Dr.S.Rocholl (Germany) says: “This method personally seemed unreliable to me at first. However, gradually I became convinced that it was completely justified. Currently, in my practice, I almost always use the depophoresis method. Only in rare absolutely “clear” cases after vital extirpation of single-rooted teeth with straight canals and in the absence of apical changes do I use traditional methods.”
Main differences between depophoresis and traditional methods
| Actions | Depophoresis | Mechanical-instrumental method |
| Channel search | No difference | No difference |
| Channel preparation | The apical third is not affected | Expansion throughout the depth of the canal up to the physiological opening |
| Canal sterilization | Complete sterility of the entire apical delta | Reducing the number of microbes in the main channel. The apical delta is unreachable. |
| Canal filling | Only the mouth of the canal | Filling for Pulpitis up to 1-1.5 mm to the apex, for periodontitis - completely |
| Subsequent audit | Hassle-free | Problematic |
| Risk of complications | Insignificantly small | Quite big |
| Treatment success | About 96% | 40-60% |
Indications for treatment using depophoresis
General indications
- functional ability of the tooth in perspective
- possibility of crown reconstruction
- sufficient tooth stability despite periradicular tissue changes (granulomas, cysts)
- satisfactory general condition of the patient (as for other types of endodontic treatment)
Specific indications
- canals with gangrenous contents 4 severely deformed root
- obliterated canals
- after unsuccessful treatment or in the presence of a crown, if most of the root filling can be removed
- channels with wide opening
- after the so-called vital extirpation
Advantages of depophoresis compared to other endodontic methods
- reliably proven treatment success in 96% of cases
- much less loss of tooth substance and therefore preservation of mechanical stability of the root
- much lower risk of perforation
- no need for channel measurement
- minimal risk of the healing or filling substance leaving the root apex
- reliable sterilization of the entire apical delta
- no need for root apex resection
- increase in indications for successfully predicted endodontic treatment - severely curved roots, obliterated canals, wide main opening
- treatment of canals that are not accessible to an instrumental approach
- low probability of hematogenous reinfection
- Osseoid closure of the hole leads to complete physiological cure
- exceptional efficiency (saving time, money, effort of the doctor and patient)
Clinical case 1
Chronic periodontitis 5 bottom left. Depophoresis sessions with copper-calcium hydroxide were performed. Additional filling with gutta-percha/silapex not up to the apex
After 6 months, significant reduction of the lesion
Clinical case 2
Chronic periodontitis 7 bottom left
Image 12 months after 3 sessions of depophoresis and incomplete filling with atacamite - gutta-percha
Root canal treatment
Root canal treatment takes place in several stages. Before treatment, X-rays or computed tomography must be taken. Using CT or X-ray images, the doctor will determine the approximate length of the root canals, shape, and the presence of obstacles to their cleaning.
Preparation for root canal treatment involves administering anesthesia and isolating the tooth from saliva using a rubber dam. If a tooth is severely damaged, the doctor can first restore its walls using temporary filling material.
Pulp is the general name for the “internal organs” of a tooth. To understand what root canal treatment is, why it is needed, and what the criteria are, let’s look at the structure of the tooth.
A tooth has two main parts: the crown and the root. Inside each tooth there are cavities that are filled with loose fibrous connective tissue - pulp. In the past, root canal treatment was called “removing the nerve.” But the nerve is only one of the components of the pulp.
tooth structure
A tooth is a whole living organ. Through the apex of the tooth root – the apex – a bundle of blood and lymphatic vessels and nerve endings enter the tooth. When, due to advanced caries or as a result of injury, the enamel and dentin of a tooth are damaged, the infection penetrates inside, into the pulp, and inflammation of the internal tissues of the tooth occurs - pulpitis.
Depulpation or treatment of pulpitis includes two main points: cleaning and filling . This is significantly different from installing a regular filling. During cleaning, the doctor removes all the inflamed pulp from the coronal part and all the root pulp. In order to do this efficiently, there are modern diagnostic methods, including computed tomography (CT) and work with a microscope. They allow you to accurately assess the number of root canals, their location, shape and degree of destruction.
depulpation
Until some point, it was believed that the upper sixth teeth had three roots, but now in 80% of cases there is an additional fourth root canal. The lower incisors have one canal, but additional branches can often be seen on a CT scan or under a dental microscope. Previously, they went unnoticed, which means they were infected. The infection spread, complicated inflammation occurred, and the tooth was destroyed. Modern dental techniques, such as the use of CT scans and microscopes, give doctors more opportunities for accurate diagnosis.
The first important criterion in the treatment of pulpitis is maximum cleaning of the canals. They need to be passed all the way to the apex, to the very apex, where the neurovascular bundle enters the tooth. This is done mechanically using special tools, so-called files. After this, the root canal is expanded, removing all the inflamed pulp, and a taper is created so that it can be properly filled with filling material.
Channels are often curved, have micro-branches, and their mechanical processing is limited. On the first visit, after mechanical cleaning, a preparation is left in the tooth, which chemically sterilizes the branches of the canals that are inaccessible for mechanical treatment. After a while, the canals are filled and the tooth crown is restored.
We always try to keep teeth alive so that they perform their functions well. A pulpless tooth is a dead organ. It is like a prosthesis that is neither capable of regeneration nor of perceiving too cold or hot to protect itself. But there are situations when, due to caries or injury, the pulp is damaged, becomes inflamed, and that very familiar toothache occurs, which, due to a natural change in the blood supply to the body, intensifies by night. Previously, arsenic was applied under a temporary gluten filling, and then the nerve was mechanically removed. For such manipulations, dentists are feared at the genetic level. But today in modern clinics, treatment of any pulpitis is accompanied by anesthesia, and patients do not experience any pain.
What are the criteria for treating teeth with pulpitis? They often think that it is enough that the tooth does not hurt and there is a filling. But even if the tooth hurts for 3-4 days or a week without treatment, the pulp dies. Due to infection, the nerve, blood vessels and tooth become dead. But if the pain goes away, this does not mean that the tooth has recovered! It becomes a hidden source of infection, and the next stage may develop when the infection progresses further. The tooth is secured in its bed by a system of ligaments. The space between it and the jaw is filled with connective tissue - periodontium. If the pulp in the tooth has already died, it will become a source of infection, which passes into the periodontium and then we get periodontitis - inflammation of the root tips and tissues around the tooth. In this case, the body tries to localize the source of inflammation, and a cyst may appear (from the Greek κύστις “bubble”). This is a cavity that fills with exudate (pus), and from which bone destruction can begin.
In a living tooth, a possible reaction to cold/hot due to enamel defects quickly passes because the tooth is restored. But if the pulp is inflamed, then under the influence of chemical and mechanical irritants it will hurt for a long time. Depending on the stage of inflammation, the duration of pain increases. As soon as the inflammatory process moves to the periodontium, we begin to feel pain when biting. This happens because the ligaments on which the tooth is suspended in its socket normally absorb pressure. But if the tooth is sick, then the inflamed receptors perceive any pressure as an excessive load and signal about it.
The immune system can hold back the development of such hidden inflammatory processes for some time, but as soon as the immune system is weakened, due to banal hypothermia, the amount of exudate can begin to increase sharply, and then we see gumboil and facial asymmetry. This is already inflammation of the periosteum. There is also a milder course of periodontitis, when a fistulous opening is formed on the gum, and during exacerbation, pus comes out of it. In patients, it happens that something swells, then goes away, an abscess appears and goes away. The presence of a fistula may be an indication that there is a problem with the roots of the teeth.
It is important for patients to know that even high-quality root canal treatment involves depulping the tooth. The tooth becomes dead, and this has much more difficulties than treating caries.
Timely diagnosis, prevention and treatment will save you from complex root canal treatment. But if it has come to this, it is important to understand that this is a responsible operation. It is not quick, it is not cheap, but it is necessary. Root canal treatment can take a long time – two to three visits. This depends on the number, shape of the root canals and the degree of infection.
Cleaning and expansion of root canals
Root canal cleaning begins with measuring its length. A special instrument that resembles a needle in appearance is inserted into the root canal. A special apparatus is attached to this instrument - an apex locator. When the root apex is reached, the device beeps and the distance to the apex appears on its display.
After measuring the length, the doctor begins to clean the canal from the remnants of the nerve and expands it. Root canals can be expanded using hand instruments that the doctor holds in his hands or using machine or rotary instruments. Rotary instruments are inserted into a special tip - an endomotor. Development with machine tools is more modern and more expensive. It speeds up the process and provides higher quality processing. In order for a doctor to achieve a similar effect using hand instruments, the doctor will need much more time. After each insertion of each instrument, the doctor rinses the root canal with a chlorine-containing antiseptic.
After processing and drying the root canal, it is filled.
Medical Internet conferences
Tooth perforation is the formation of a pathological communication between the internal cavities and canals of the tooth with the surrounding tissues.
The reasons for the development of this complication:
1. Insufficient opening of the tooth cavity;
2. Insufficient knowledge of the topography of the dental cavity;
3. Wrong choice of tool and violation of the methodology for its use;
4. Excessive expansion of the mouths;
5. Significant bends of the root canals.
Clinically, perforation of the bottom or walls of a tooth manifests itself in the form of a characteristic “sinking” of the instrument, bleeding and sharp pain in the patient in the case of treatment without anesthesia, and probing in the perforation area also causes acute pain. However, for a more accurate diagnosis of perforation, an apex locator and x-ray should be used. The best prognosis is observed in cases where the perforation is closed immediately, which minimizes trauma and infection of surrounding tissue. The most unfavorable localization of perforation is the area of root furcation. Almost any perforation in this area leads to destructive changes in the periodontium [1].
The main goal of endodontic treatment is to eliminate infection and restore the integrity of the body's tissue barriers against microbial invasion. Materials that come into contact with living tissues must be biocompatible. There are many materials available for closing perforations: amalgam, composites, and glass ionomer cements. The main negative properties of these materials are microleakage, toxicity, and sensitivity to moisture. The ProRoot MTA material does not have all these disadvantages.
This material was developed at Loma Linda University (USA, California) by Professor of the Department of Endodontics Mahmoud Torabinejad [2].
The ProRoot MTA (Mineral Trioxide Aggregate) system is a powder consisting of small hydrophilic particles that turn into a solid cement paste in the presence of water due to hydration of the powder in less than four hours.
Composition: 75% Portland cement, 20% bismuth oxide, 5% dehydrated calcium sulfate [3].
Indications for use of the material:
1. perforation of the root and bifurcation area;
2. vital amputation;
3. apexification;
4. retrograde filling of the root apex;
5. elimination of root resorption [4].
Method of using the ProRoot MTA system to restore root canal perforation:
1. Having applied a rubber dam, we clean the root canal of sawdust and half-life products;
2. Dry the root canal system with paper points and isolate the perforation site;
3. Obturate all canals located apically from the perforation;
4. Prepare the ProRoot MTA material in accordance with the attached instructions;
5. Using the supplied application probe, place the material in the defect area. We compact the material in the cavity;
6. We make sure that the material is placed correctly using an x-ray;
7. Place a moistened cotton swab into the cavity and fill the canal with temporary restoration material for at least 4 hours;
8. After 4 hours, or during the next appointment, we inspect the ProRoot MTA material. The material must be hard. If this is not the case, wash and repeat application;
9. When the material has hardened, we obturate the remaining part of the canals. ProRoot MTA should remain as a permanent part of the root canal filling [5, 6].
Measles canal filling
The procedure for filling root canals is carried out in various ways, for example: by the method of cold lateral (side) condensation of gutta-percha pins (reliable and affordable). Pins that resemble gutta-percha sticks in appearance are inserted into the root canal. After insertion, these sticks are compacted against one of the walls of the root canal. Between the gutta-percha there is a special paste for filling the canals.
The most modern method is filling the root canals using the vertical condensation method of hot gutta-percha. With this method, the doctor seals the top of the root canal using a heated gutta-percha pin. After this, the remaining volume is filled with hot liquid gutta-percha. This method is more expensive.
After the filling, if everything is done well, the doctor removes excess gutta-percha and sealer, and then installs a temporary filling. X-ray control is required. Permanent tooth filling in one visit is carried out only in exceptional cases, since it is necessary for the material to cool completely.
After root canal filling, discomfort may persist for some time. The tooth may be sensitive when biting. Within a few days the pain goes away.
Causes of obliteration of tooth canals
The main and most common causes of tooth root obliteration are:
- injuries;
- chronic inflammatory processes;
- age-related changes;
- poor quality treatment;
- the presence of cancer associated with the proliferation of connective tissue.
There are also factors that increase the likelihood of root canal obliteration. These include:
- malocclusion;
- heredity (in particular with marble disease and Stanton-Capdepont syndrome);
- metabolic and endocrine system disorders;
- exposure to chemicals on teeth over a long period of time;
- decreased functionality or inactivity of the tooth during chewing.
How to understand whether the root canal is filled properly
Signs of a properly treated canal are visible on x-ray: filling to the tops of the root, dense filling of the canal without any excess or voids. It is not desirable to have material residues outside the root canal. If the paste does not dissolve, an inflammatory process may develop in the future. But the quality of work depends not only on the attending physician: the patient himself also plays an important role. By following all the dentist’s recommendations, observing the rules of oral hygiene, as well as a careful approach to the health of your teeth, this is the only way you can achieve the desired results.
Root canal treatment and filling should always be trusted only to experienced specialists. An experienced dentist in Minsk is waiting for you at the Family Dentistry Center. Comfortable treatment, modern equipment of European quality, highly qualified specialists and an individual approach to each patient. Thanks to the use of drug sedation, all procedures can be performed without stress and pain, and children's fears of the dental office will go away on their own.
Treatment methods for root canal obliteration
Treatment of a tooth with root canal obliteration is quite difficult. Most often, in such cases, surgical removal of the part of the tooth affected by the pathological process is used, as well as chemical devitalization, in which tissue mummification is performed using special injections.
Treatment of root canal obliteration is a rather painful procedure, since due to the obstruction of the tooth patency, injection anesthesia is ineffective. The complexity of treatment causes the possibility of complications. These include perforation of the root canal and/or dental crown and possible pain due to incomplete elimination of canal obstruction.
Posted in Articles | Tags: 3-D CT, clinical case, CBCT