A. Zorian , Candidate of Medical Sciences, Department of Hospital Therapeutic Dentistry, Moscow State Medical University
A. Hovsepyan , director of dental clinical training, dentist V. Chilikin , associate professor, candidate of medical sciences, Honored Doctor of the Russian Federation, Department of Hospital Therapeutic Dentistry of Moscow State Medical University
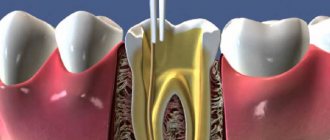
The success of endodontic treatment is largely determined by the quality of root canal filling. High-quality filling today means three-dimensional sealing of the entire branched root canal system, which plays the role of a reliable barrier between the tooth cavity and periodontal tissues.
Over the long history of endodontics, various techniques and materials have been used to fill the root canal.
Until recently, the main method of filling root canals in Russia was the method of filling with one paste. At the same time, pastes based on zinc oxide and eugenol, as well as preparations containing resorcinol and formaldehyde, were very popular. The technique of filling a root canal with paste is quite simple and does not require significant time and material costs. However, filling canals with one paste has a number of significant disadvantages: 1. With this technique, only the main canal is filled with the material, and numerous branches of the root canal system remain open. 2. Very often the paste is discharged beyond the root apex, since there is no adequate control over the filling of the root canal with material. 3. The paste fills the root canal unevenly, leaving voids and not providing adequate sealing. 4. All pastes shrink and dissolve upon contact with tissue fluid. 5. Most pastes have an irritating effect on the periodontium.
Considering all of the above, it is not surprising that the International Dental Association and the American Dental Association do not recommend the use of the root canal obturation technique with one paste.
Endodontic materials
An ideal root canal filling material must meet the following parameters: 1. Provide a reliable seal throughout the entire root canal system. 2. Be non-toxic and have good biocompatibility. 3. Do not irritate the periodontium. 4. Do not shrink in the canal. It is desirable that it expands slightly when introduced into the canal or during the curing process. 5. Have a bacteriostatic effect or at least not support the growth of bacteria. 6. Easy to sterilize before use. 7. Be radiopaque. 8. Do not change the color of the tooth. 9. If necessary, it can be easily removed from the canal. 10. Have a curing time sufficient for comfortable work. 11. Do not dissolve in tissue fluid. 12. Have good adhesion to dentin and filling material.
Such an ideal material does not exist today. However, these requirements are best met by the methods of filling root canals with gutta-percha and sealer. The vast majority of root canals around the world today are filled using gutta-percha.
Cost of services
Consultation with an implant surgeon 0 rub.
1-canal tooth (canal filling with gutta-percha pins) 750 rub.
2-canal tooth (canal filling with gutta-percha pins) 980 rub.
3-canal tooth (canal filling with gutta-percha pins) RUB 1,300.
Placing a temporary filling costs 200 rubles.
Compomer filling for permanent teeth RUB 1,000.
Filling for permanent teeth made of gypsum resin, cotton RUB 1,200.
Filling for permanent teeth made of photocomposite RUB 1,800.
Placement of a light-curing filling for non-carious lesions RUB 2,000.
Placement of a light-curing filling for average caries RUB 2,500.
Placement of a light-curing filling for deep caries RUB 3,000.
Placement of a light polymerization filling for periodontitis (taking into account the formation of a cavity and the application of a lining) RUB 2,350.
Placement of a light polymerization filling for pulpitis (taking into account the formation of a cavity and the application of a gasket) RUB 2,370.
Restoration of the crown part of a tooth using light polymerization materials (caries) RUB 3,050.
Restoration (caries, pulpitis) RUB 4,650.
Filling root canals with gutta-percha
Gutta-percha is a hard, but at the same time elastic and flexible coagulation product of the latex of tropical gutta-percha plants. Gutta-percha is divided into two types - alpha and beta - which differ greatly in physical properties.
For the production of gutta-percha points, beta-gutta-percha is traditionally used, which has greater hardness and spatial stability and less stickiness. Beta gutta percha requires higher temperatures to soften. However, recently, more fluid and sticky alpha gutta-percha has become increasingly popular, providing, when used in a heated state, a more homogeneous filling of the entire branched root canal system.
Alpha gutta-percha is used for techniques that involve working with thermoplasticized (heated) gutta-percha: vertical condensation and thermoplastic injection techniques. In addition, there is a special type of gutta-percha used to produce Thermafil obturators. This patented type of gutta-percha is similar in chemical properties to beta-gutta-percha, but at the same time has the physical characteristics of alpha-gutta-percha.
The production of gutta-percha points is mainly concentrated in Southeast Asia. One of the largest suppliers of gutta-percha is Korea. However, recently gutta-percha points have begun to be produced in Brazil.
Pins are divided into standard pins, which have a 2% taper and ISO sizes from 10 to 140, and tapered pins, which have a 2% to 12% taper and sizes from 20 to 30.
Gutta-percha points are made either manually (“hand-rolled”) or by machine. It is believed that the manual method provides higher precision in making pins. Machine-made pins often do not guarantee accurate calibration. It should be especially noted that all pins made in Brazil are machine-made.
The commercial name “gutta-percha pins” has taken root well and is used everywhere, although the content of gutta-percha itself in these pins is about 20%. The main component of the pins (60-70%) is zinc oxide. The remaining 10% consists of barium sulfate, wax, dyes and other additives.
The main advantage of gutta-percha is the predictability of root canal obturation. Its advantages also include good biocompatibility and low toxicity, the ability to condense, ensuring dense and uniform filling of the root canal, softening when heated, which allows for three-dimensional obturation of the root canal system, spatial stability (in the hardened state it practically does not change its volume) and ease of its removal from the root canal if re-treatment is necessary.
Despite all the obvious advantages, gutta-percha also has a number of disadvantages associated with the peculiarities of its physical and chemical properties and the technology of application. The disadvantages of gutta-percha are as follows: 1. It cannot be used without a sealer, since it does not have adhesion to dentin. 2. Gutta-percha does not have a bactericidal or bacteriostatic effect. 3. Thin pins have very high flexibility and softness, which requires high qualifications and experience of the doctor, especially when filling narrow canals, and can also lead to deformation of the pins during their fitting. 4. Thermoplasticized gutta-percha shrinks when cooled. To compensate for this shrinkage, it is necessary to continue the condensation process until it cools.
Sealers for root canal obturation
It should be noted that the need to use a sealer is a relative disadvantage, since there is currently no material that can provide predictable filling of the main channel, and at the same time be fluid enough to fill all its branches.
The sealer acts not only as a sealant that fills all branches of the root canal system and ensures adhesion of gutta-percha to the canal walls, but also as a lubricant that ensures free sliding of gutta-percha pins in the root canal.
The sealer must meet the following requirements: 1. After mixing, it must have a sticky consistency in order to ensure good adhesion to the canal walls after curing. 2. Seal the canal hermetically. 3. Be radiopaque. 4. Do not shrink during the curing process. 5. Do not stain tooth tissue. 6. Have a bacteriostatic effect or at least not support the growth of microorganisms. 7. Harden slowly. 8. Do not dissolve in tissue fluids. 9. Do not irritate periapical tissues. 10. Dissolve in standard solvents if it is necessary to unseal the canal. 11. Do not cause immune reactions in periapical tissues. 12. Do not have a mutagenic or carcinogenic effect.
None of the sealers presented on the modern market can meet all the requirements placed on it. Basically, either natural root cements or polymeric materials are used as sealers today. Natural sealers – Endomethasone (Septodont), Cortisomol (Pierre Rolland), Tubli-seal (Kerr), etc. – which are based on zinc oxide, dissolve in tissue fluid, which can lead to disruption of the tightness of the root canal system. In addition, they have low adhesion to dentin and can cause staining of tooth tissue. At the same time, polymer sealers - AH Plus (Dentsply), Adseal (META Biomed), etc. - are less soluble in tissue fluid, do not stain tooth tissue and have better adhesion to root dentin.
Until now, the question to what level to fill the root canal remains open. There is intense debate as to whether gutta-percha should not reach the anatomical apex by 0.5 mm or stop directly at it. Today, the only indisputable fact is that the less we expand the apical narrowing, the better the quality of obturation, the more reliable the isolation of periodontal tissues. In addition, it must be remembered that the theory of active apical therapy has shown its inconsistency. In modern endodontics, removal of sealer beyond the root apex is not encouraged, even in the presence of inflammatory processes in the periodontium, although studies have shown that when a small amount of sealer is removed into the periapical tissue, no serious complications are observed after treatment.
***
There are various methods for filling root canals with gutta-percha: the single (central) pin method, lateral condensation, thermomechanical condensation, filling the root canal with chemically softened cold gutta-percha, intracanal hot vertical condensation, thermoplastic injection technique and the use of thermophiles.
Filling root canals with cold gutta-percha
Single pin method
This method consists in the fact that after appropriate treatment of the canal, which means giving it a taper of 4, 6 or 8%, a sealer is applied to its walls using a paper point. After this, a pre-selected pin with an appropriate taper and tip size is inserted into the canal. The pin should fit snugly against the canal walls. Some authors recommend shortening the tip of the pin by 0.5 mm. Using a heated tool, the pin is cut at the level of the mouth and its condensation is carried out in the vertical direction.
This technique can be a good alternative for doctors who prefer to fill canals with monopaste, but this only ensures filling the lumen of the main canal, and not three-dimensional obturation of the entire root canal system.
Concept of procedure
The procedure for removing old fillings from dental root canals is called disobturation. The filling is completely removed, after which all dental cavities are cleansed of its remains. The future fate of the diseased tooth depends on the quality of such actions.
During the procedure, special instruments are used to clean from the crown of the tooth to the apical part. In this case, expansion is carried out first with smaller devices, and then with larger ones. Only in this option will cleaning be complete and effective.
Method of lateral condensation of cold gutta-percha
This scheme involves filling with gutta-percha pins with lateral pressing of each of the pins against the canal walls. For a long time, this technique was the “gold standard” with which all other canal obturation techniques were compared.
After drying the root canal using paper points, its walls are coated with sealer. Then a master pin selected to size is inserted into the canal, the tip of which is moistened in the same sealant. A spreader is then used to condense the master pin against the canal walls, providing sufficient space for the insertion of additional pins. The density of canal obturation depends on the depth of penetration and the shape of the spreader. According to Chohayeb (1993), ISO-standardized hand spreaders should be inserted into the root canal up to 1 mm from the tip of the gutta-percha point, which improves the homogeneity and density of the filling. After the master pin condenses, additional pins are condensed to it and the channel walls, the tips of which are also wetted in the sealant. Each subsequent pin enters the canal to a shallower depth. Lateral compaction of the pins is carried out until the canal is homogeneously filled, the criterion for which is the impossibility of inserting the spreader into the canal. The recommended time for pressing the pins against the canal walls with a spreader, according to various authors, is 15–30 seconds. After this, the protruding ends of the gutta-percha pins are cut off using a heated instrument, and the mouth of the canal is closed by vertical condensation of gutta-percha.
The quality of root canal obturation during lateral condensation of cold gutta-percha is influenced by many factors. First of all, this is the shape of the processed channel. The root canal must have a uniform taper along its entire length and an apical ledge that prevents material from being removed beyond the apex during condensation. The ratio of gutta-percha to sealer is also of great importance. The following ratio is recommended: 95% gutta-percha, 5% sealer.
Long-term use of the lateral condensation technique of gutta-percha has shown its high clinical effectiveness, ease of use and reliability. Many researchers point to the high filling density of the root canal when performing lateral condensation. However, other authors demonstrate that when performing lateral condensation, there is a risk of longitudinal root fracture due to the forces applied, especially when the root is weakened (for example, when the canals in thin roots are over-expanded). In addition, with this technique it is not possible to achieve homogeneity of the material and filling the lateral and apical branches of the canal with gutta-percha, which can lead to the development of complications from periodontal tissues - the development (or maintenance) of an inflammatory reaction, destruction of bone tissue.
It should be added that when working with cold gutta-percha, in order to adequately seal the mouth of the root canal, it is advisable to use a heated instrument to cut off the pins 2-3 mm deeper than the mouth of the canal and fill the remaining part with heated gutta-percha by injecting it.
In order to improve technologies for filling root canals with cold gutta-percha, various techniques have been proposed, which are currently of interest mainly only from the point of view of the history of the development of endodontics. Such techniques include thermomechanical condensation and filling with chemically softened cold gutta-percha.
Thermo-mechanical condensation (or filling root canals with a rotating condenser)
This method is currently practically not used. With this technique, a tool that has in its design elements of an H-file (but with a reverse thread) and a channel filler is used to soften the gutta-percha and move it in the apical direction. This instrument is called a condenser or gutta condenser. To soften the gutta-percha and condense it, the instrument must be rotated clockwise at a speed of at least 8000 rpm.
A standard gutta-percha pin should be 1–2 sizes larger than the last instrument used to process the canal, that is, 1–2 mm shorter than the working length. Control of the level of gutta-percha filling is ensured by inserting the instrument, 1.5 mm short of the apical constriction.
The disadvantages of the method are the unpredictability of the level of filling, the high risk of breaking off the instrument in the canal, and the likelihood of voids forming in the gutta-percha due to its gluing to the instrument. In addition, this technique also does not provide reliable obturation of the lateral branches of the canal.
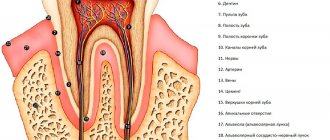
What can be seen in the photo?
The canal must be completely sealed, that is, to the top - the material in this case is highlighted in a bright white color, which should be filled to its entire length.
It should not only be filled to its entire length, but also have no gaps on the sides - this means that the material should be tightly obturated. The image should not show pieces of hanging gutta-percha, smeared material or dark gaps.
By following all stages of filling, you can avoid tooth inflammation. Otherwise, you will have to waste a lot of time and effort restoring the lost tooth.
Filling root canals with chemically softened cold gutta-percha
Filling techniques using chemically softened cold gutta-percha are also called “immersion methods.” Historically, these methods appeared almost simultaneously with the beginning of the use of gutta-percha. For obturation of gutta-percha softened with solvents (chloroform, some oils), no sealer was used. This led to micro-seepage due to shrinkage of the gutta-percha after the solvent evaporated and the root filling hardened. Therefore, the incidence of complications when using such techniques was very high. Despite the fact that later various sealers began to be used with “immersion” methods, these techniques are currently practically not used due to the inability to control the shrinkage and deformation of gutta-percha and the quality of canal obturation.
Modern technologies in the field of tooth refilling
Dental treatment under a microscope is one of the newest services that has appeared in dentistry. High-tech equipment allows specialists to fill the dental canal with better quality, more accuracy and efficiency. Thanks to the use of such a device, the likelihood of causing harm to healthy tissue is close to zero. In addition, the treatment is carried out very delicately. Microscope glasses allow you to view the tooth at multiple zooms. This will allow you to see all the affected areas that may simply not be visible during normal examination.
A microscope allows dentists to perform root canal treatment faster and safer for the patient.