- When is root canal filling indicated?
- What are the purposes of temporary filling?
- What material should be used for temporary filling?
- How does filling occur?
- What does pain after filling mean?
- Types of fillings
- Types of pastes
- How much does temporary root canal filling cost?
The period for which a temporary filling is placed is determined by the attending physician.
In most cases, a drug that has a long shelf life is placed under the filling material. After this period, the doctor removes the temporary material. When medicinal pastes are used together with disinfectants and antiseptic medications, there is a significant increase in the effectiveness of treatment. In addition, there will be no cross-contamination of soft and hard tissues between visits to the doctor.
When is root canal filling indicated?
There are general indications for the procedure:
- The root canal is affected. This happens if the patient has a chronic form of pulpitis.
- During the purulent stage of pulpitis, regardless of whether the tooth cavity is closed/open.
- If intraradicular soft tissues are excessively affected.
After mechanical processing is completed, a funnel-shaped channel is formed. It has a minimum diameter at the apex, and a minimum at the mouth. Also, the balance between the “diameter and wall thickness” of the channel is observed.
Indications for temporary filling of root canals
Temporary filling with a paste based on calcium hydroxide is indicated for chronic pulpitis with a closed tooth cavity that has 2 or more root canals; chronic apical periodontitis with a closed tooth cavity having 2 or more root canals; acute apical periodontitis of pulpal origin with a closed tooth cavity.
Temporary filling with a paste based on calcium hydroxide with iodoform is indicated for acute purulent pulpitis with an open and closed tooth cavity; chronic ulcerative pulpitis with an open tooth cavity; chronic hyperplastic pulpitis; pulp necrosis with open and closed tooth cavity; acute apical periodontitis of pulpal origin after the removal of acute phenomena; chronic apical periodontitis with an open tooth cavity.
All patients in need of endodontic treatment are prescribed an X-ray examination at the stages of measuring the working length, filling the root canals, as well as in the long term.
Instrumental treatment, which involves eliminating the source of infection and forming the required shape of the root canal, is carried out using the “Step Back”, “Crown Down” or a mixed method.
After mechanical processing, a funnel-shaped canal is formed with a minimum diameter in the apex area and a maximum at its mouth; a balance is maintained between the diameter of the channel and the thickness of its walls; a constant position of the apical foramen is ensured; an apical stop is created to prevent the filling material from being pushed into the periodontium. Medicinal treatment is carried out, the walls of the root canal are dried using paper points.
In the treatment of pulpitis without symptoms of apical periodontitis (low contamination of the canals), the method of temporary filling of root canals with calcium hydroxide-based paste is used. In case of pulpitis with symptoms of periodontitis, chronic periodontitis, acute and at the acute stage of chronic periodontitis (after acute symptoms have resolved), the root canals are additionally treated with a 2% solution of chlorhexidine (exposure 2 minutes), after which they are temporarily filled with a paste based on calcium hydroxide with iodoform.
Method of temporary filling of root canals
Filling a canal with paste can be done either manually or using a canal filler.
Method of “manual” filling. Using a limiter, the working length of the canal is fixed on a K-file, K-reamer or on a special cannula - a syringe attachment. At the tip of the instrument, a small amount of paste is introduced into the equine canal up to the apex. Condense the paste using a damp cotton pad. The next portion of paste is injected to 2/3 of the working length of the canal.
Condense the paste in the same way. The next portion of paste is injected to 1/3 of the working length of the canal. Excess paste that has accumulated above the mouth is pressed into the canal using a cotton ball. The tooth cavity is hermetically sealed with a temporary filling for 48 hours.
Filling technique using canal filler. The canal filler, a size smaller than the last instrument used to expand the root canal, is fixed in the tip and the working part is immersed in the paste, retaining a small amount of material on the spiral. The instrument is inserted into the canal up to the apex, turned on at low speed (100-120 rpm) for 2-3 seconds, then the instrument is slowly removed from the canal while the drill is running.
The canal filler is again enveloped with filling material, inserted into the canal to 2/3 of the working length, the drill is turned on and the material is pumped into the canal, then the procedure is repeated. Excess paste that has accumulated above the mouth is pressed into the canal using a cotton ball. The tooth cavity is hermetically sealed with a temporary filling for 48 hours. If there is painful percussion, the canal is filled again at the next visit.
If the apical opening is wide or it was expanded during instrumentation, then the first portion of the paste is injected and condensed “manually” and only then the canal filler is used.
On the second visit, the remains of the temporary sealer are removed from the root canal using an H-file of the required size using scraping movements. Scraping is periodically alternated with irrigation of the root canal with an antiseptic solution using an endodontic syringe with a needle until the temporary sealer on the H-file is completely removed, after which the root canal is dried with paper points and filled using the sealer and gutta-percha points using the lateral condensation method. For permanent filling, according to indications, sealers are used, which contain calcium hydroxide with iodoform, zinc oxide eugenol, hydroxyapatite, and glass ionomer cement.
Assessment of the quality of endodontic treatment is carried out immediately after treatment and in the long term (after 6, 12 months). The criteria for clinical well-being are: absence of complaints; painless percussion; normal state of the transitional fold in the area of projection of the apex of the root of the tooth under study; positive dynamics or absence of pathological changes in the tissues of the apical periodontium on the radiograph.
Efficiency of temporary filling of root canals
Postgraduate student of the Department of Therapeutic Dentistry of BelMAPO O. V. Fedorinchik assessed the immediate results of endodontic treatment in study groups I (pulpitis without periodontitis) and II (with apical periodontitis).
After treatment, there were no complaints in 75.0% of cases in the control (without the use of calcium hydroxide); after temporary filling, this figure reached 95.2%. Within 1-2 days, complaints of pain when biting were reported in 11 cases (17.2%) in the control group; in the main group they were recorded in only three teeth (4.8%).
On days 3-5, in the control group, pain persisted in 5 teeth (7.8%), while in the main group it was absent.
In group II, complaints of pain after endodontic treatment were absent in the control group in 50.8% of cases, in the main group - in 85.7%. Pain when biting 1-2 days after treatment was noted by 22 patients (36.1%) in the control group and 6 (10.7%) in the study group.
On days 3-5, pain in the control group was 13.1%, i.e. 8 cases, and only 2 (3.6%) in the main group. Thus, when using temporary root canal filling, pain is significantly reduced.
The results of endodontic treatment after 6 months are presented in Table No. 1. In the main group, in 100% of cases there were no complaints of pain in the area of the treated tooth. In the control group, complaints of periodic pain were reported in one case. An X-ray examination in the control group revealed an expansion of the periodontal gap in the apical periodontal tissues in five teeth (7.8%), in the main group this figure was recorded in one case (1.6%).
When using a paste with iodoform for temporary filling, there were no complaints of pain in 98.2% of patients, and periodic pain was observed in only one tooth (1.8%). At the same time, in the control group there were no complaints in 72.1%, and periodic pain in the area of the treated tooth was bothersome in 17 cases (27.9%).
On the radiograph in the control group, there were no changes in the periodontium in 55.7% of cases, in the main group - in 80.4% of treated teeth.
At a follow-up examination after 12 months in group I (pulpitis), there were no complaints of pain in the control group in 95.3% of cases; in the main group there were no complaints in 100% of cases. Periodic pain in the area of the treated tooth was recorded in the control group in 3 cases, 4.7%. X-rays after 12 months showed no changes in the apical periodontal tissues in 85.9% of the teeth in the control group; in the main group, this figure reached 98.4%. In the apical region of 9 teeth (14.1%) in the control group, an uneven expansion of the periodontal fissure was noted, while in the main group these changes were recorded only in one case (1.6%).
In the main group II (apical periodontitis) there were no complaints in 100% of cases, in the control there were no complaints in 93.4%.
During X-ray examination, the absence of changes in the apical periodontal tissues was noted in 73.8% of cases in the control group. In the main group, this figure reached 92.9%. The expansion of the periodontal fissure in the area of the apical periodontium was preserved in 12 teeth of the control group (19.7%). In the main case - in 4 cases (7.1%).
Conclusion
Studies have shown that temporary filling of root canals can statistically significantly reduce the incidence of complications in both pulpitis and periodontitis. 6 months after treatment of pulpitis, the number of complications was minimal.
Complaints about pain and radiological changes in the area of the treated tooth were significantly less common in the main group. After 12 months, positive radiographic dynamics were more often observed in the main group, where a paste based on calcium hydroxide with iodoform was used.
LITERATURE
- Antanyan A. A. // Endodontics today. - 2007. - No. 1. - P. 59 - 69.
- Kazeko L. A., Fedorova I. N. Calcium hydroxide in endodontics: yesterday, today, tomorrow // Modern dentistry, 2009. - No. 2. - P. 4 - 9.
- Lopatin O. A., Fedorinchik O. V. The use of calcium hydroxide preparations in the treatment of complicated caries // Modern dentistry, 2007. - No. 3. - P. 33 - 37.
- Lutskaya I.K. Restorative dentistry: equipment, tools, auxiliary materials. - Rostov-on-Don: Phoenix, 2008. - 202 p.
- Lutskaya I.K., Martov V.Yu. Medicines in dentistry. - M.: Medical literature, 2007. - 384 p.
- Lutskaya I.K., Chukhrai I.G., Novak N.V. Endodontics: A Practical Guide. - Moscow: Medical literature, 2009. - 191 p.
- Bartlett D. A difference in perspective - the North American and European interpretation of tooth wear / D.Bartlett, K.Phillips, B.Smith // Int. J. Prosthodont. - 1999. - Vol. 12, No. 5. - P. 401 - 408.
- Basrani B., Santos JM et al. // Oral Surgery Oral Medicine Oral Pothalogy Oral Radiology & Endodontics. — 2002. — Aug; 94(2). — P. 240—245/
- Cwikla S., Belanger M., Giguere S., Vertucci F. // J. Endod. - 2005. - V.31, No. 1. - R. 50-52.
- Gomes B., Souza S., Ferraz C. // Intern. Endod. J. - 2003. - V. 36. - P. 267-275.
- Ingle JI, Bakland LK Endodontics. - Baltimore$ Philadelphia et al., 1994. - P. 230-241.
- Katebzadth N., Hupp J., Trope M. Histological signs of periapical inflammation after obturation of infected root canals of teeth in dogs // Journal of Endodontics 25, 1999: 364 -8.
A complete list of references is in the editorial office.
What material should be used for temporary filling?
There are special requirements for the material used for filling:
- Creating complete tightness, which is achieved by penetrating even the smallest cracks. This helps create a kind of barrier that prevents the development of bacteria. If microorganisms develop a small cavity into which they can penetrate, the inflammatory process will re-develop.
- The materials should be clearly visible on x-ray. Thanks to this, the doctor is convinced that high-quality work has been done.
- High aesthetics. The material should not be visible through tooth enamel.
- Saliva, hard or soft tissues of the oral cavity should not provoke an allergic reaction by contacting the filling mass.
- Materials for temporary filling of root canals should be easily removed from the roots. After the substance hardens, a slight shrinkage effect may appear, but no cavities are formed.
How is canal filling done with paste?
Proper filling of root canals promotes a speedy recovery without any complications. To do this, it is necessary to use proven and high-quality drugs, as well as sterilized dental instruments. Only a highly qualified doctor can perform the procedure correctly, so we recommend contacting only reputable dental clinics.
Filling is performed in stages with a clear sequence of actions:
- All affected tissue is removed. In some cases, the practice is used to remove healthy tissue in order to gain unhindered access to each section of the canal.
- Pulp extraction.
- Channel length analysis. Note that the length of the canals varies; the root and its bends play a special role in this matter.
- Mechanical processing of channels. The channels are carefully processed along their entire length to create the maximum possible space. If this is neglected, the material will not be able to spread throughout the entire volume of the channel.
- Canal filling with gutta-percha. The last stage of work. Its effectiveness will directly depend on the correct measurement of the channel length, as well as on the quality of the machining.
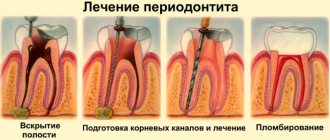
How does filling occur?
Before temporary filling of the canals begins, the patient is sent for an X-ray examination. Using the image, the extent and depth of the lesion is determined. Then a technique is selected and the procedure begins. It consists of the following steps:
1. Administration of anesthesia. Local anesthesia is used. Many patients have a fear of the sound of the drill, even if there is no pain. These patients are given intravenous sedation.
2. Clean the tissues affected by caries (enamel, dentin).
3. The dental nerve is removed.
4. Probe the root passage. Its depth is determined.
5. The width of the passage is expanded and drilled.
6. Wash with an antiseptic solution and dry.
7. If necessary, a pin is inserted.
8. Material is placed into the cavity, taking into account the developed technique.
9. Carrying out a control x-ray examination.
Materials for filling the canals of permanent formed teeth
Modern pediatric dentistry has access to a wide selection of plastic hardening agents for final filling of dental roots, differing in composition and properties. Most often, in the treatment of periodontitis in children and the treatment of other diseases that require canal cleaning, materials based on the following components are used:
- eugenol and zinc oxide;
- polymers and resins (silicone, composite compounds, epoxy resins);
- calcium compounds (hydroxyapatite, calcium hydroxide);
- glass ionomers (cements);
What does pain after filling mean?
The presence of discomfort for three to five days after the procedure is normal. The reason for their appearance is irritated gum tissue and pulp. The patient may complain of a feeling of fullness inside the treated tooth. This is also normal.
To avoid negative consequences, you should contact only an experienced and qualified specialist. Otherwise, the following consequences may arise due to mistakes made:
- A through hole is formed in the root canal.
- Secondary inflammation develops under the filling material.
- Flux and fistula develop.
- A cyst or granuloma forms.
- Allergic reaction to the material.
By choosing a clinic that has a good reputation, you can not be afraid of the above problems.
Materials for root fillings
Prices for dental canal filling depend on the chosen procedure method and the consumables used. We, as modern dentistry, use:
- plastic material, gutta-percha, for the main filling of the tooth canal
- and special sealers and pastes to ensure maximum tightness.
Gutta-percha is the most modern material with antibacterial activity. It does not dissolve and does not lose its properties throughout the life of the tooth. The sealer we use (AH plus, Dentsply, USA) is recognized as the “gold standard” for root canal treatment all over the world.
Types of fillings
There are 2 types - temporary and permanent root canal filling.
The first method uses a non-hardening paste, which is distinguished by the presence of medicinal properties. Getting a good result occurs due to calcium hydroxide. The use of temporary filling is indicated for advanced pulpitis, when the inflammatory process has spread quite deeply. A special material is placed into the cavity and covered with a filling. Installation of a permanent filling may take several days or even months.
The second method (permanent filling) is carried out for more than a dozen years. The procedure is allowed immediately during the first visit to the doctor, if there is no inflammatory process, or after treatment with temporary material has ended.
Preparation for the procedure
Proper preparation is the most important aspect of endodontic treatment. If you do not provide for all possible nuances, the effectiveness of the procedures may be reduced to zero. Before filling directly, it is necessary, first of all, to thoroughly clean the root canal of any plaque that has formed, and also remove all damaged tissue.
In general, all preparatory actions are quite standard. They are carried out in stages and have the following action plan:
- carious lesions are eliminated, as well as dead tissue (specialized drills are used for this);
- pulp is removed from open canals;
- An x-ray is taken to determine the specific shape and length of the canal;
- The root canal is expanded to the required size using various attachments and other tools.
Please note that strict adherence to all of the above points is the key to effective treatment. If you neglect at least one of these stages, with a high degree of probability the current situation will only worsen.
Types of pastes
Paste containing an antibiotic and a corticosteroid
In most cases, such a paste contains 2-3 broad-spectrum antibacterial drugs and a corticosteroid. Basically, it is dexamethasone. The paste contains it in a certain amount, therefore, while reducing inflammation and allergic reactions, there is no disruption of the periodontal protective reactions. The third component is a radiopaque filler. Thanks to him, it is possible to objectively assess how well the channels have been filled. This paste has a strong, but not long-lasting effect. The duration of their presence in the dental canals varies from three to seven days.
Paste containing metronidazole
This component helps to effectively suppress pathogenic microflora in the root canals, stop kagabolic tissue destruction, and block the inflammation process. The patient will not have an allergic reaction to such a paste, and there is also no need to be afraid of addiction.
A paste with this component is used in case of excessive infection of the canals. In addition, such a remedy can cure the acute stage of periodontitis. As a result, re-infection can be easily prevented. Also, the disease progresses much easier.
Paste based on a long-lasting antiseptic mixture
This type of paste consists of antiseptic components that have a strong effect - camphor, thymol, cresol, menthol, etc. This is a radiopaque paste, it does not harden, and gradually dissolves in the root canal. Indications for the use of such a paste are the presence of pulpitis, periodontitis, and problems with baby teeth.
Calcium hydroxide paste
A highly alkaline reaction occurs; when the canal is filled with this substance, various bacteria are destroyed and necrotic tissue is destroyed. In addition, stimulation of ostogenesis, dentinogenesis and cementogenesis begins.
The use of a non-hardening paste, which includes calcium hydroxide, is necessary for severe periodontitis, cystogranuloma. This mass is placed in the channel; a special channel filler is used for this purpose.
After six weeks, the paste is replaced. A new portion is placed into the root canals. After this, the paste is changed every eight weeks until the desired result is achieved. If the pain and inflammation have disappeared, and exudation has stopped, the doctor cleans the canals and fills them with permanent filling material.
Injection (liquid) gutta-percha technique
In this technique, gutta-percha is used in the form of blocks, which are placed in a heating device, in which gutta-percha is heated to a temperature of 185-200°C and fed into the canal in liquid form. alloescort
The liquid gutta-percha technique, when performing the protocol, ensures the penetration of gutta-percha and sealer into both the main root canal and the dentinal tubules . The increase in temperature on the outer surface of the root is insignificant and has minimal damaging effects on the tissue.
The effective use of this technique, however, is determined by the doctor's skills, developed and honed on extracted teeth.
Filling with hot gutta-percha
Sealing the root passages with heated gutta-percha can be done in several ways. The most common of them are:
- injection method (filling the channel with material heated to 200 degrees);
- method of vertical condensation (laying filling material into the canal, distributing it with instruments along the side canals, installing a softened pin on top of it);
- continuous wave method (introducing a basic central pin into the tooth using a heated instrument, placing side pins around it, completely sealing the canal).
Filling with chilled gutta-percha
Gutta-percha is a resinous compound obtained from the milky sap of a number of plants and is a high-molecular hydrocarbon similar in composition to natural rubber. There are several methods for sealing root passages using this material:
- single pin technique (the treated root course will have a shape identical to the shape of the pin, after which the gutta-percha pin is placed in the prepared hole);
- lateral condensation technique (initially the base pin is inserted into the center of the stroke, then the side ones);
- sealing using a rotating capacitor;
- filling with gutta-percha softened with chemicals.