Teeth (dentes)
Located
in the dental alveoli of the upper and lower jaws using a continuous connection - impaction, gomphosis.
Tooth structure:
- Corona dentis - tooth crown
Facies lingualis - lingual surface
Facies vestibularis (facialis) – vestibular (facial) surface
Facies occlusalis [masticatoria] – closure surface [masticatory]
- Radix dentis - tooth root
Apex radicis dentis – apex of the tooth root
Foramen apicis dentis - opening of the apex of the tooth root
- Cervix dentis – neck of the tooth
- Cavitas dentis [pulparis] – dental cavity
Cavitas coronalis [coronae] – crown cavity
Canalis radicis dentis – tooth root canal
Pulpa dentis - tooth pulp
Tooth substance:
- Dentinum - dentin
- Enamelum – enamel
- Cementum - cement
Types of teeth:
- Dentes decidui – milk teeth
Complete dental formula of primary teeth:
| 2 0 1 2 | 2 1 0 2 |
| 2 0 1 2 | 2 1 0 2 |
2. Dentes permanentes - permanent teeth
Complete dental formula of an adult
| 3 2 1 2 | 2 1 2 3 |
| 3 2 1 2 | 2 1 2 3 |
- Dentes incisivi – incisors
- Dentes canini – fangs
- Dentes premolares – small molars (premolars)
- Dentes molares – large molars (molars)
- Dens serotinus – wisdom tooth
Function of teeth
– grasping, separating, crushing, chewing, grinding food, forming speech.
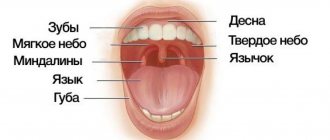
Oral anatomy
The oral cavity is the beginning of the digestive apparatus. The oral cavity is divided into two sections by the alveolar processes of the jaws and teeth: the vestibule of the mouth and the oral cavity itself.
The vestibule of the mouth is the space located between the lips and cheeks on the outside and the teeth and gums on the inside. The vestibule of the mouth opens outward through the oral opening. The transverse oral fissure is limited by the lips, which are muscle folds, the outer surface of which is covered with skin, and the inner surface is lined with mucous membrane.
The oral cavity is located on the inner side of the alveolar processes, limited above by the hard palate and the anterior portion of the soft palate; the bottom is formed by the diaphragm of the mouth and is occupied by the tongue.
The oral cavity is lined by the oral mucosa, covered with stratified squamous non-keratinizing epithelium. It contains a large number of glands. The area of the mucous membrane attached around the neck of the teeth on the periosteum of the alveolar processes of the jaws is called the gum. The oral cavity communicates with the pharynx through the isthmus of the pharynx.
The cheeks are covered on the outside with skin, and on the inside with the oral mucosa, which contains the ducts of the buccal glands and is formed by the buccal muscle. Subcutaneous tissue is especially developed in the central part of the cheek. Between the masseter and buccal muscles is the fatty body of the cheek.
The upper wall of the mouth (palate) is divided into two parts. The hard palate is located in the anterior part of the oral cavity, formed by the palatine processes of the maxillary bones and the horizontal plates of the palatine bones. The palatine bones are covered with a mucous membrane, along the midline of which there is a suture of the palate, and on the sides there are several transverse palatine folds.
The hard palate passes into the soft palate, formed mainly by muscles and aponeurosis of tendon bundles. In the posterior part of the soft palate there is a small conical protrusion, called the uvula, which is part of the so-called velum palatine. Along the edges, the soft palate passes into the anterior palatoglossal arch and the posterior palatopharyngeal arch. Between the arches on each side, in the recesses lie the palatine tonsils. The lower palate and arches are formed mainly by muscles that help swallowing.
The muscle that lifts the velum palatine of the soft palate and narrows the pharyngeal opening of the auditory tube begins on the lower surface of the petrous part of the temporal bone and attaches to the middle section of the aponeurosis of the palate, intertwining with bundles of the muscle of the same name on the other side.
The palatoglossus muscle narrows the pharynx, bringing the anterior arches closer to the root of the tongue. Its beginning is located on the lateral edge of the tongue root, and its attachment point is on the aponeurosis of the soft palate.
The triangle of the velopharyngeal muscle brings the velopharyngeal arches closer together, pulling the lower part of the pharynx and larynx upward. The muscle begins on the back wall of the lower part of the pharynx and attaches to the aponeurosis of the soft palate.
The tongue is a mobile muscular organ located in the oral cavity and facilitates the processes of chewing food, swallowing, sucking and speech production. The tongue is divided into the body of the tongue, the apex of the tongue, the root of the tongue and the dorsum of the tongue.
From above, from the sides and partially from below, the tongue is covered with a mucous membrane, which fuses with its muscle fibers, contains glands, lymphoid formations and nerve endings - receptors. On the back and body of the tongue, the mucous membrane is rough due to the large number of papillae of the tongue, which are divided into four groups:
- Filiform papillae are located throughout the body of the tongue and represent a conical body with racemose appendages at the apexes.
- Fungiform papillae are located on the back of the tongue closer to its edges and have the shape of pineal growths.
- Leaf-shaped papillae are concentrated in the lateral sections of the tongue and represent 5-8 folds separated by grooves. They are unequal in size and are most pronounced in the posterior parts of the tongue.
- Cylindrical papillae, surrounded by a ridge of mucous membrane, the largest, but weakly protruding above the surface, are located on the border between the root and body of the tongue.
The muscles of the tongue are represented by skeletal muscles and the actual muscles of the tongue. Skeletal muscles connect the root of the tongue to the bones of the skull. The actual muscles of the tongue have points of origin and attachment points in the thickness of the tongue, located in three mutually perpendicular directions: the lower longitudinal muscle shortens the tongue; the superior longitudinal muscle flexes the tongue, shortening it, and raises the tip of the tongue; the vertical muscle of the tongue makes it flat; The transverse muscle of the tongue reduces its diameter and makes it transversely convex upward.
When the mouth is closed, the tongue with its upper surface comes into contact with the palate. The mucous membrane, passing to the lower surface of the tip of the tongue, forms the so-called frenulum along the midline. On either side of it, at the bottom of the mouth, on the sublingual fold, the ducts of the submandibular gland and sublingual gland open, which secrete saliva and are therefore called salivary glands.
The submandibular gland is an alveolar-tubular protein-mucosal gland located in the lower part of the neck in the submandibular fossa, below the mylohyoid muscle.
The sublingual gland is an alveolar-tubular protein-mucosal gland located under the mucous membrane of the mouth on the mylohyoid muscle under the tongue.
The excretory duct of the third, the parotid salivary gland, opens in the vestibule of the mouth on the mucous membrane of the cheek, at the level of the upper second molar.
Teeth, depending on their structure and functions, are divided into large molars, small molars, canines and incisors. All of them are strengthened in the sockets of the alveolar processes of the lower and upper jaws.
Each tooth consists of a part that protrudes above the gum - the crown of the tooth, a part covered by the gum - the neck of the tooth and an internal part - the root of the tooth. Moreover, some teeth have two or more roots.
The bulk of the tooth is dentin, which is covered with enamel in the crown area, and with cement in the neck and root area.
The root of the tooth is surrounded by a root membrane - the periodontium, which, with the help of tooth ligaments, attaches it to the dental alveolus. Inside the crown of the tooth there is a tooth cavity, which continues into a narrow canal of the tooth root. Vessels and nerves pass through a small hole in the apex of the tooth root into the tooth cavity containing the pulp, or pulp.
According to data from dental reference books
A full range of dental services in Istra for adults and children: from consultation to complex operations within one clinic “Doctor Nebolit”
Consultation and appointments daily from 9:00 to 19:00
- +7 (49831) 4-42-12
- Contacts
Exudative erythema multiforme of the oral cavity
The disease begins suddenly with malaise, chills, weakness, and increased body temperature (in severe cases, up to 38 °C and above). Patients complain of headaches, aching pains throughout the body, pain in muscles and joints, and sore throat. After 1-2 days, bluish-red spots appear on the hands, forearms, legs, and sometimes the face and neck, slightly rising above the surrounding skin. Their central part sinks slightly and takes on a bluish tint, while the peripheral part retains a pinkish-red color (cockades). Subsequently, a subepidermal bubble filled with serous or hemorrhagic contents may appear in the central part. Skin rashes are sometimes accompanied by itching and burning or generally go away without pain.
The mucous membranes of the lips, cheeks, floor of the mouth, tongue, and soft palate are most often affected. The first manifestations of exudative erythema multiforme in the oral cavity are diffuse or limited erythema and swelling of the mucous membrane, against which subepithelial blisters of various sizes appear. Damage to the oral mucosa is accompanied by severe pain even at rest. When moving the tongue and lips, the pain increases sharply, making it difficult to eat. Patients are starving, which further worsens their condition. The blisters open quite quickly, forming painful erosions on the oral mucosa, covered with fibrinous plaque. On the red border of the lips, erosions become covered with bloody crusts, making it difficult to eat and open the mouth. In the first days after the opening of the blisters, along the edges of the erosions one can see grayish-white remnants of the covering of the blisters; when pulled, the epithelium cannot be stratified (negative Nikolsky's sign). Poor oral hygiene and the presence of carious teeth aggravate the course of erythema multiforme. Infection of erosive surfaces with oral microflora occurs. Sometimes the course of exudative erythema multiforme is complicated by the addition of fusospirochetosis. Erosion on the oral mucosa becomes covered with a thick layer of yellowish-gray plaque, plaque appears on the teeth and tongue, and bad breath appears. Salivation increases. Regional lymph nodes are enlarged and painful. The period of exacerbation is 2-4 weeks. Erosion epithelializes after 7-12 days; after healing, no scars remain.
The picture of peripheral blood during the period of exacerbation of exudative erythema multiforme corresponds to an acute inflammatory process.
The severity of the course of exudative erythema multiforme is determined mainly by the nature of the damage to the oral mucosa. The severe form is characterized by a pronounced hyperergic reaction of the body, as well as generalized damage to the mucous membranes of the mouth, eyes, genitals and skin.
In the case of a mild course of exudative erythema multiforme, the general condition of the patients does not change significantly; isolated elements of the lesion are detected on the oral mucosa. However, as the duration of the disease increases, its severity worsens. For exudative erythema multiforme of an infectious-allergic nature, a long, relapsing course is typical. Exacerbations of the disease are observed mainly in the autumn and spring periods (1-2 times a year), although there are known cases of more frequent exacerbations of the disease. Sometimes relapses can be triggered by hypothermia, previous infections and other factors that weaken the body’s resistance. Exudative erythema multiforme lasts for years. During periods between exacerbations, there are no changes in the oral mucosa and skin.
Symptomatic (toxicoallergic) exudative erythema multiforme recurs only when the patient comes into contact with the etiological factor (drug-allergen).
Cytological examination of scrapings from the area of erosion reveals a picture of acute nonspecific inflammation.
Histologically, the subepithelial location of blisters is determined in exudative erythema multiforme. There are no signs of acantholysis. The rejected epithelium undergoes necrosis, swelling and inflammatory infiltration in the underlying connective tissue.