From this article you will learn:
- Dental fissure sealing – what is it?
- what material is better to use,
- non-invasive fissure sealing in children – price, reviews.
The article was written by a dentist with more than 19 years of experience.
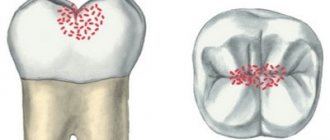
Fissure sealing is a technique for preventing caries of chewing teeth, used in pediatric dentistry, although it can be used with no less success in adults. Fissures are natural grooves that are located on the chewing surfaces of molars (between the chewing cusps). In such grooves, food debris is well retained, which leads to the development of fissure caries in the fissures of milk and permanent teeth.
Dental fissure sealing involves sealing fissures on the chewing surface of teeth - most often using special filling materials (they are called sealants). This leads to the formation of a mechanical barrier from the filling material, which prevents the impact of cariogenic factors on the fissures. An alternative to the use of sealants is the mineral fissure sealing technique, which we will also discuss below.
Fissure sealing: before and after photos
For mineral sealing of fissures, the drug “Enamel-sealing liquid” is used, which consists of fluorine compounds and highly dispersed calcium hydroxide. But in most cases, sealants are still used to seal fissures - these are special sealants that belong to one of the following classes of filling materials:
- composites (light or chemical curing),
- glass ionomer cements,
- compomers.
Important: Different classes of sealants may be optimal for different patients. For example, in newly erupted teeth with very low enamel mineralization, it would be optimal to use glass ionomer cements or use the mineral fissure sealing method. But in almost all other cases, preference should be given to composites (below we will dwell on the pros and cons of different materials).
How does fissure sealing with sealants work?
The main indications for fissure sealing are the average and high risk of developing dental caries (i.e. in the case of more than 1 carious cavity per year). In children under 6 years of age, fissure sealing is carried out in primary molars, and in children over 6 years of age - in erupting permanent molars and premolars. Fissure sealing can be carried out immediately after the chewing surface of the tooth has erupted, without waiting for the entire tooth crown to erupt.
How fissure sealing protects against caries:
- Firstly , with the help of filling material, a barrier is created on the chewing surface of the tooth, which prevents the impact of various cariogenic factors on the fissures. Thus, sealing teeth with sealants prevents the retention of food debris in the depths of fissures, as well as the effects of organic acids produced by cariogenic bacteria.
- Secondly , sealing teeth can increase the resistance of tooth enamel to organic acids produced by cariogenic bacteria (if the material used for sealing fissures contains active fluoride ions). This promotes the mineralization of enamel deep in the fissures and additionally prevents the development of caries.
Important: the effectiveness of this method of caries prevention has been confirmed by numerous clinical studies. For example, professional fluoridation of teeth with varnish leads to a reduction in the increase in caries on treated surfaces by up to 70%. In turn, the fissure sealing method leads to a decrease in the increase in fissure caries over 1 year - already at the level of 92.5% (on average). And even higher efficiency can be achieved if these methods are combined.
Preventing dental problems at home
Rules for the prevention of caries at home, if followed, children will grow up with healthy and strong teeth:
- brush at least twice a day, use dental floss;
- rinse the mouth with fluoride-containing solutions;
- choose toothpastes containing calcium and fluoride;
- buy healthy foods for children, eat solid vegetables and fruits;
- try not to procrastinate with such childhood habits as sucking pacifiers and bottles;
- do not allow biting nails and various hard objects;
- normalize the bite;
- promptly treat respiratory diseases.
It is very important that the child understands the importance of prevention and daily oral hygiene procedures as early as possible.
Fissure sealing in children: price 2022
For fissure sealing in children, the price will range from 600 to 1,200 rubles per tooth (in economy-class and mid-price clinics). This difference in cost will depend on the sealing method - invasive or non-invasive, as well as on the type of material for sealing the fissures.
The method of non-invasive sealing of fissures (without opening them with a drill) is always cheaper. But if you have narrow, deep fissures that will need to be opened with a drill before inserting the material, the price will be around 1,200 rubles without the cost of anesthesia. You will have to pay another 300-400 rubles for pain relief.
Non-invasive sealing technique:
A non-invasive technique is used to seal medium or deep open fissures. The open type of fissures means that they are completely accessible for visual inspection (after all, only this guarantees that the doctor will not miss caries in the area of the bottom or walls of the fissure). The non-invasive sealing technique means that we will not use a drill to expand the fissures.
There are 2 options for non-invasive sealing, which we will discuss below. Firstly, this is a mineral fissure sealing technique, and secondly, a non-invasive sealing technique using sealants. Sealants are special sealants (they can belong to three classes of filling materials - glass ionomer cements, composites or compomers).
1) Mineral fissure sealing –
It is carried out using the drug “Enamel-sealing liquid”, which was specially developed for mineral sealing of dental fissures (method of deep fluoridation of teeth). This is a two-component preparation for sequential application to the enamel. The first bottle contains anhydrous magnesium fluoride silicate, anhydrous copper-II fluoride silicate and sodium fluoride, and the second bottle contains highly dispersed calcium hydroxide.
Enamel-sealing liquid:
When applied sequentially, very small particles of calcium fluoride are formed (about 10 nanometers). The resulting crystals are located not only on the surface of the enamel, but also penetrate in large quantities into the smallest defects of the enamel, and even foci of demineralization. In the depths of these lesions, they will be located in a thixotropic silicic acid gel environment, which protects them from being washed out (due to this, they remain inside the enamel from 6 months to 2 years). In this case, the particles will constantly release fluoride ions in a concentration sufficient for remineralization.
The effectiveness of mineral fissure sealing:
- A clinical study (Knappwost et al.) showed the very high effectiveness of this method. It was found that 4-5 years after mineral sealing of fissures in 715 permanent teeth, the fissures remained unaffected by caries in 95.2% of them.
- Scientific work “Comparative effectiveness of deep fluoridation and fissure sealing of the first permanent molars” (authors – Adamchik Yu.A., Varno A.A.).
A clinical study showed that 6 months after mineral sealing of fissures in children aged 6-7 years, fissures remain unaffected by caries in 95.3% of first permanent molars. This study compared mineral sealing with non-invasive sealing using the filling material Fissurit F. So, the preservation of the sealant and its loss (while maintaining healthy intact fissures) was observed only in 29.2% and 25.0% of teeth, respectively, and in other cases fissure caries was observed. Thus, some studies show that mineral fissure sealing may be even more effective than non-invasive sealants in some cases. - Scientific work “Clinical and laboratory justification for the choice of fissure sealing method for permanent and temporary teeth in children” (author – I.V. Kravchuk). The study showed that the use of the deep fluoridation method for the prevention of fissure caries in permanent and temporary teeth in children 6-8 years old allows us to achieve 66.9% and 74.6% reduction in caries growth over 1.5 years.
2) Non-invasive fissure sealing with “sealants” –
Of course, the best materials for non-invasive fissure sealing are composite sealants. One of the most popular representatives of this class of materials is the light-curing sealant “Fissurit F”, which also has the property of releasing fluoride ions into the surrounding tooth tissue. However, composites require preliminary etching of the enamel with orthophosphoric acid, and therefore their use is contraindicated in patients with a low level of fissure mineralization (low AIM).
Non-invasive fissure sealing: Before and After photos
Stages of sealing fissures with composites (Fig. 5-10):
First, the surfaces of the teeth are thoroughly cleaned using a polishing brush and paste (Fig. 5). Next, the tooth is isolated from saliva, after which the surface of the fissures is etched for 15-30 seconds using a gel with 37% phosphoric acid (Fig. 6). After this, the gel is washed off with a stream of water, and the surface of the teeth is dried. Please note that the acid-etched surface of the fissures will have a chalky color (Fig. 7).
Next, a composite sealant is applied (for example, “Fissurit F”) and carefully distributed over all fissures (Fig. 8-9). After applying the sealant, the material must be given 15-20 seconds to flow into the depth of the fissure. Next, the sealant is illuminated for 20 seconds with a polymerization lamp (Fig. 10), after which the chewing surface of the tooth is grinded and polished.
Stages of fissure sealing in the photo:
Indications for non-invasive sealing with composites:
- Erupting and maturing molars with an average level of fissure mineralization (average UIM). Moreover, before sealing the fissures, it would be optimal to carry out a 1-month course of remineralization therapy and/or 3-4 dental fluoridation procedures (at intervals of 5-10 days) to speed up the processes of enamel mineralization.
- Permanent molars and premolars in children and adults – with a medium or high risk of developing caries.
- Before fixing braces.
Important:
for teeth with a high level of fissure mineralization (high UIM), fissure sealing is usually not recommended (in this case, it is optimal to maintain good hygiene + periodically treat the teeth with fluoride varnish).
Non-invasive sealing of teeth in children (video) –
Non-invasive sealing with glass ionomer cements and compomers –
It must be said that fissure sealing can be carried out not only with composites, but also with glass ionomer cements (GIC) and compomers. GICs have some advantages over composites, for example, they do not require preliminary etching of the enamel, and are also less sensitive to moisture (which is important in young children). However, their disadvantages are insufficient strength, rapid abrasion, insufficiently good marginal fit, and low fluidity.
Most scientific works agree that the use of GIC for fissure sealing may be advisable only in one case - in newly erupted teeth with extremely low fissure mineralization (with low UIM). As for compomer sealants, they are a cross between composites and GIC. The biggest disadvantage of compomers is a very high degree of abrasion; for example, they completely disappear in just 1.5-2 years.
Reviews
Practice shows that timely prevention is the most effective way to reduce the incidence of dental diseases. This is evidenced by the reviews of our patients.
Thank you for choosing Natadent clinic and coming back to us again.
LEAVE FEEDBACK
Invasive sealing technique:
Indications for invasive fissure sealing:
- In the presence of narrow deep fissures in teeth with weak enamel mineralization (if the bottom and walls of the fissures cannot be subjected to visual or instrumental control). In this case, it becomes impossible to guarantee the absence of foci of carious lesions in the area of the bottom and walls of the fissures. In addition, in the presence of deep narrow fissures, it is extremely difficult to achieve good filling of the fissure with filling material.
- Initial fissure caries.
- The presence of pigmented fissures in teeth with weak enamel mineralization (with good enamel mineralization, pigmented fissures do not require mandatory invasive sealing).
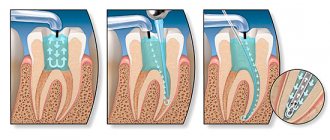
Expansion of fissures with a drill during invasive sealing –
Unlike non-invasive techniques, invasive fissure sealing involves expanding the fissures with a drill. In Fig. 11-12 you can see the initial situation (narrow deep fissures and a small amalgam filling), as well as the appearance of the fissures after they were expanded with a drill. In Fig. 13 we can already see fissures filled with composite sealant.
Video of fissure treatment with a drill –
Stages of the procedure
Sealing the fissures of primary and permanent teeth takes place in several stages:
- Professional teeth cleaning to remove plaque and food debris from fissures and enamel surfaces.
- The next step is to rinse and cover the teeth with cotton to block saliva from reaching the enamel.
- Coating the enamel with a specialized adhesive that makes its surface rough.
- Drying teeth and applying sealant.
- Distribution of the sealing composition along the fissure and removal of sealant residues.
- Using a curing lamp to harden the composition.
- Check to see if there is any discomfort when closing the jaws.
- (if necessary) Correcting the position of the sealant, removing its residues.
The total duration of the procedure is about 15-20 minutes. The cost of fissure sealing in children varies depending on numerous factors, so it is determined individually, after an initial examination by a specialist.
What is the best way to seal fissures?
We have already said above that 3 groups of sealants are used to seal fissures. These are chemical or light-curing composites, glass ionomer cements (GIC), and compomers. Below we will tell you how long materials of different classes are preserved in fissures. And the scientific work “Methodology of sealing dental fissures and comparative characteristics of modern materials for sealing” (authors Nelovko, Mehdiyeva) will help us with this.
- Composite materials – these materials are made from a special composite resin and can be cured either with light or chemically. Materials of this class are divided into 2 subgroups: unfilled and filled sealants. The former have high fluidity, and therefore penetrate even the narrowest and deepest fissures; in addition, they adhere more tightly to the enamel surface, but wear out faster and require replacement.
Filled sealants have less fluidity and penetration depth, and therefore they are more often used for invasive fissure sealing technology (see below). Their disadvantage is also their high sensitivity to moisture and complex application technology. Pros: high abrasion resistance.Important: this class of materials allows you to protect your teeth from fissure caries for a long time (up to 5-8 years). The degree of preservation of the composite sealant 3 years after application is up to 90%. The best composite sealants include the following 3rd generation light-curing sealants: “Fissurit”, “Helioseal”, “Estisial LC” and especially those containing fluorine – “Fissurit F” and “Admira Seal”. The release of fluoride from Fissurit F continues for more than 190 days from the moment of application!
- Glass ionomer cements (GIC) – GIC-based sealants include the following materials: “Dyract seal”, “Fuji”, “Glass Ionomer”, “Aqua Ionoseal”. These materials have a pronounced cariesstatic effect due to the presence of aluminum, zinc, calcium, and especially due to the fluoride content. These materials are chemically cured; a big plus is that they do not require etching of the enamel with 38% acid before application (unlike composite materials).
Compared to composite materials, GICs have low fluidity, which does not allow their use in deep fissures without opening them with a drill, and also have a greater degree of edge leakage and wear out faster. There is an opinion that the use of GIC as fissure sealants is justified when it comes exclusively to newly erupted teeth (with extremely low mineralization of fissure enamel). In the latter case, it is not advisable to etch the enamel with acid, and for the use of composites, the enamel must always be etched.The safety of GIC 1, 6, 12 and 24 months after application is 90, 80, 60 and 20%, respectively, and after 3 years it is only 10% (in turn, the composite sealant is 90%). However, this class of materials reduces the occurrence of caries in fissures by 80-90% in 2 years.
- Compomers - they are classified as light-hardening composite materials, however, components have been added to their composition that give them the positive properties of glass ionomer cements. Advantages compared to traditional composites: greater tolerance to humid environments, greater fluidity and the ability to release fluoride in small quantities. It should be noted that these advantages had to be paid for with a greater degree of abrasion (in 2 years the compomer almost completely disappears). Materials of this class include “Dyrect Seal” (Dentsply).
The best material: Composites are undoubtedly the most effective materials, but when it comes to sealing fissures in newly erupted teeth (the enamel of which has extremely weak mineralization), then glass ionomer cement should be preferred. Also, preference should be given to glass ionomer cements when sealing fissures in children with little contact, for whom it is difficult to achieve good isolation of the tooth surface from saliva